Development of a new Cox model for predicting long-term survival in hepatitis cirrhosis patients underwent transjugular intrahepatic portosystemic shunts
2024-03-11YiFanLvBingZhuMingMingMengYiFanWuChengBinDongYuZhangBoWenLiuShaoLiYouSaLvYongPingYangFuQuanLiu
Yi-Fan Lv, Bing Zhu, Ming-Ming Meng, Yi-Fan Wu, Cheng-Bin Dong, Yu Zhang, Bo-Wen Liu, Shao-Li You, Sa Lv, Yong-Ping Yang, Fu-Quan Liu
Abstract BACKGROUND Transjugular intrahepatic portosystemic shunt (TIPS) placement is a procedure that can effectively treat complications of portal hypertension, such as variceal bleeding and refractory ascites. However, there have been no specific studies on predicting long-term survival after TIPS placement.AIM To establish a model to predict long-term survival in patients with hepatitis cirrhosis after TIPS.METHODS A retrospective analysis was conducted on a cohort of 224 patients who underwent TIPS implantation. Through univariate and multivariate Cox regression analyses, various factors were examined for their ability to predict survival at 6 years after TIPS. Consequently, a composite score was formulated, encompassing the indication, shunt reasonability, portal venous pressure gradient (PPG) after TIPS, percentage decrease in portal venous pressure (PVP), indocyanine green retention rate at 15 min (ICGR15) and total bilirubin (Tbil) level. Furthermore, the performance of the newly developed Cox (NDC) model was evaluated in an internal validation cohort and compared with that of a series of existing models.RESULTS The indication (variceal bleeding or ascites), shunt reasonability (reasonable or unreasonable), ICGR15, postoperative PPG, percentage of PVP decrease and Tbil were found to be independent factors affecting long-term survival after TIPS placement. The NDC model incorporated these parameters and successfully identified patients at high risk, exhibiting a notably elevated mortality rate following the TIPS procedure, as observed in both the training and validation cohorts. Additionally, in terms of predicting the long-term survival rate, the performance of the NDC model was significantly better than that of the other four models [Child-Pugh, model for end-stage liver disease (MELD), MELD-sodium and the Freiburg index of post-TIPS survival].CONCLUSION The NDC model can accurately predict long-term survival after the TIPS procedure in patients with hepatitis cirrhosis, help identify high-risk patients and guide follow-up management after TIPS implantation.
Key Words: Transjugular intrahepatic portosystemic shunt; Long-term survival; Predictive model
INTRODUCTION
The techniques for and practical experience with transjugular intrahepatic portosystemic shunt (TIPS) placement have significantly evolved over the past three decades[1,2]. These advancements have led to the recommendation of these guidelines as the primary method for treating complications such as cirrhosis and portal hypertension, particularly refractory ascites and gastrointestinal bleeding[3,4]. However, despite advancements in treatment, a subset of patients still succumb to mortality due to factors such as liver failure, refractory hepatic encephalopathy (HE), and rebleeding after surgery[5,6]. Therefore, accurate assessment of prognostic risk is crucial for preoperative screening of high-risk patients, postoperative follow-up management, and patient care.
Several scoring models have been used in clinical practice to assess the prognosis of patients who underwent TIPS implantation. The most widely used tool is the model for end-stage liver disease (MELD), which mainly predicts 3-month mortality among patients with cirrhosis[7,8] and is more accurate than the traditional Child-Pugh score in assessing the severity of liver disease[9]. The MELD score was subsequently modified by incorporating the serum sodium level, resulting in the MELD-sodium (MELD-Na) score, which is used for the prioritization of liver transplantation[10]. In Aschaet al[11]’s study of 261 patients, emergent TIPS placement, age, splenectomy, MELD score, and Child-Turcotte-Pugh class B and C were identified as significant predictors of long-term mortality post-TIPS, with a median survival of 26 months. In recent years, a new model [the Freiburg index of post-TIPS survival (FIPS)] based on total bilirubin (Tbil), creatinine (Cr), age, and albumin has been proposed to predict six-month survival after TIPS placement[12]. However, the novel FIPS exhibited inconsistent discrimination in external validation studies, and its superiority over conventional scores remains undetermined. Despite the continuous development of the TIPS procedure, there is currently no predictive model available for assessing the long-term survival of patients with hepatitis cirrhosis after the TIPS procedure. Hence, the objective of this study was to construct a prognostic model that accurately reflects the extended (6-year) survival of patients diagnosed with hepatitis cirrhosis following TIPS placement through a comprehensive analysis of clinical and follow-up data obtained from Beijing Shijitan Hospital over several years.
MATERIALS AND METHODS
Patient selection
Patients aged 18-80 years with hepatitis cirrhosis who underwent elective TIPS implantation for the management of refractory ascites and variceal bleeding were retrospectively recruited from January 2013 to January 2017 at Beijing Shijitan Hospital. Eighteen patients with hepatocellular carcinoma, 26 patients with missing clinical data, 9 patients with severe cardiorenal disease, 36 patients who were lost to follow-up within a year, and 7 patients who underwent TIPS revision procedures were excluded. In brief, the final dataset consisted of 224 patients who were randomly divided into a training set (n= 157) and a validation set (n= 67) at a 7:3 ratio (Figure 1). The diagnosis of hepatitis cirrhosis and portal hypertension was established through the utilization of imaging and endoscopic studies, clinical observations, and laboratory examinations. The decision to proceed with the TIPS procedure was made in accordance with established guidelines[3,13-15].
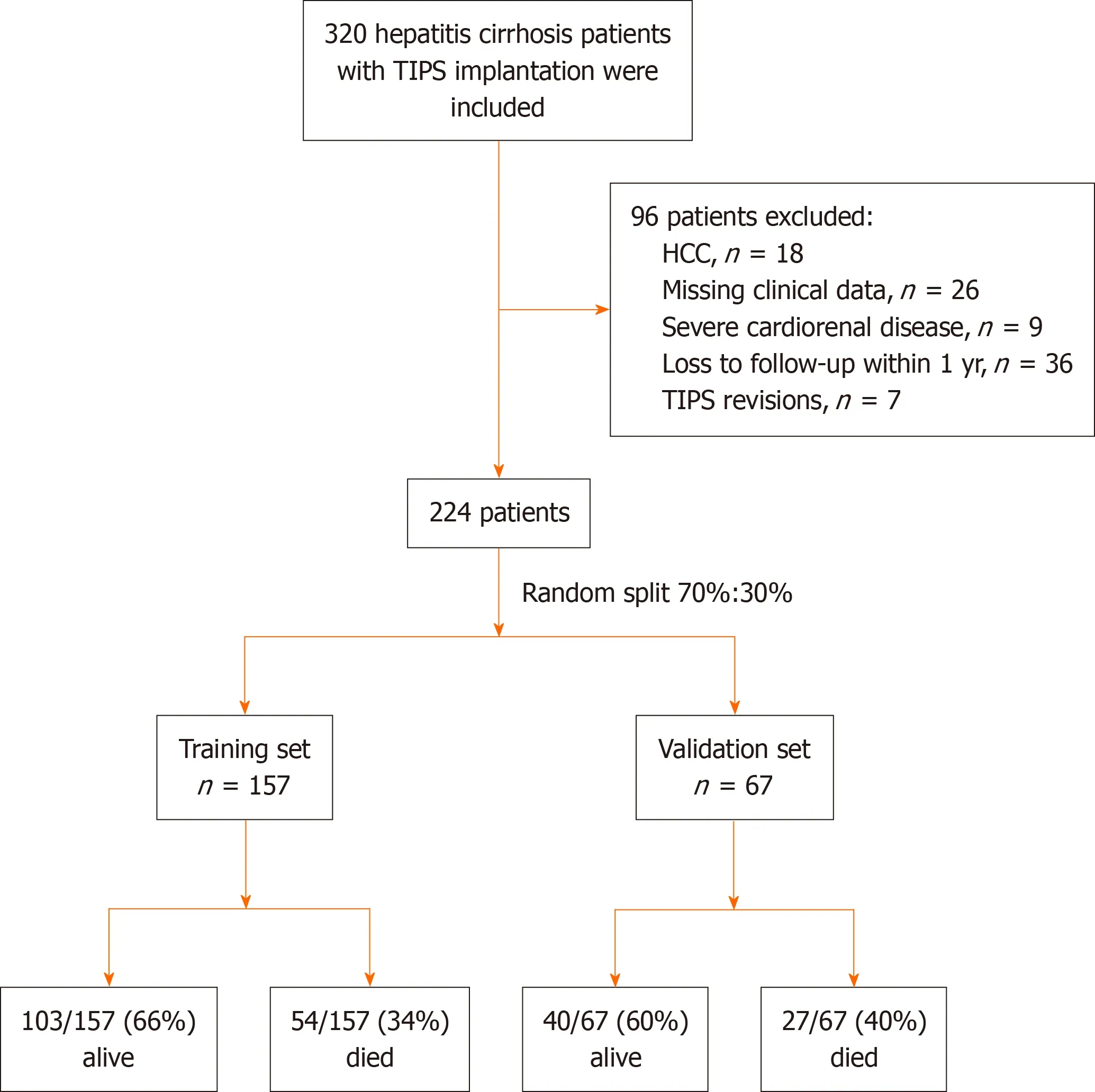
Figure 1 Flow chart of patient inclusion and allocation. TIPS: Transjugular intrahepatic portosystemic shunt; HCC: Hepatocellular carcinoma.
All clinical and laboratory characteristics that were assessed within 72 h prior to the TIPS procedure were collected by 2 physicians from the medical records. The collection of follow-up data was conducted through telephone interviews and outpatient visits, with the follow-up endpoints being death, liver transplantation, or study closure (January, 2023). Survival time was calculated from the date of the TIPS intervention. Patients who underwent liver transplantation after the TIPS procedure were censored on the day of transplantation. The study was reviewed and approved by the Beijing Shijitan Hospital Institutional Review Board and was performed in accordance with the Declaration of Helsinki.
TIPS procedure
TIPS implantation mainly involves creating a shunt between the portal vein and the hepatic vein to reduce pressure in the portal system[16]. The procedure is conducted by a radiologist who utilizes fluoroscopic guidance to insert a catheter through the jugular vein into the hepatic vein. Following this, hepatic venography was performed to ascertain the exact location and anatomical features of the hepatic vein and inferior vena cava (IVC) junction. Subsequently, the portal vein was punctured, portal venography was conducted, the parenchymal tract was dilated, and a reasonable shunt was established (Figure 2). All patients received polytetrafluoroethylene-covered stent grafts, and an analysis of the portal venous pressure gradient (PPG) was performed before and after stent placement.

Figure 2 Reasonable shunts, indicated by orange arrows.
Remarkably, there is no universally accepted criterion for shunt reasonability, which is related to various factors, such as the shunt channel diameter[17] and the spatial relationship between the stent and the blood vessels. In terms of safety, the core factors considered are short-, medium- and long-term efficacy and quality of life. Thus, a reasonable shunt should result in a 30%-50% decrease in portal venous pressure (PVP) or a decreased PPG of 6-12 mmHg[18]. Additionally, the covered stent portion should exhibit a lack of angular formation and instead appear either straight or parallel to the IVC and portal vein. Consequently, the blood flow within the stent should be characterized by a smooth trajectory, and the covered part of the stent should completely cover the proximal and distal puncture points.
Statistical analyses
This retrospective study was conducted to determine the predictive value of an alternative score for 6-year survival in patients after TIPS implantation for refractory ascites or/and secondary prophylaxis for variceal bleeding. SPSS (version 27.0, IBM Corp., Armonk, New York) and R (version 4.3.1, R development Core Team) were used for the statistical analyses. SPSS is primarily used for basic statistical tests, such as between-group comparisons of qualitative or quantitative variables, while R is favored for more advanced statistical modeling and graphing. Continuous variables are presented as the mean with standard deviation, and categorical variables are presented as absolute and relative frequencies [n(%)]. Student’sttest or the Mann-WhitneyUtest was used to assess the differences in quantitative variables between groups. The chi-square test was used for analyzing unordered categorical variables, while the Mann-WhitneyUtest was applied for examining ordered categorical variables. The Kaplan-Meier (K-M) method was used to analyze differences in mortality risk among patients at different scoring levels, which were tested using the log-rank test. Cox regression was used to analyze the effect of each scoring model on the long-term prognosis of patients treated with the TIPS procedure. Receiver operating characteristic (ROC) curves and calibration curves were used to evaluate the discrimination and calibration ability of the models. A nonparametric approach (Delong-Delong & Clarke-Pearson)[19] was used for pairwise comparisons of the areas under the ROC curves (AUCs). Two-tailedPvalues < 0.05 were considered to indicate statistical significance.
RESULTS
Patient characteristics
A total of 320 patients who underwent TIPS placement were included in this study. Based on the given inclusion and exclusion criteria, 224 patients were eventually included. Table 1 describes the basic and clinical characteristics of the patients. The main etiology was hepatitis cirrhosis, and the indications for TIPS implantation were refractory ascites (training: 21%vsvalidation: 24%), secondary prophylaxis for variceal bleeding (training: 57%vsvalidation: 55%) and both (22%vs21%). The survival rates were similar in the training and validation cohorts (49.9%vs39.1%,P= 0.233).

Table 1 Baseline characteristics of patients in the training and validation cohorts
Development of the predictive model
First, univariate Cox proportional hazards regression analysis was carried out to select potentially important prognostic factors (P< 0.05) for multivariate Cox regression analysis (Table 2). The Akaike information criterion (AIC) was applied in a backward stepwise regression to select the best model, with smaller AICs indicating better results. To avoid multicollinearity, the Child-Pugh, MELD, MELD-Na, and FIPS scores were not included in the model, and preoperative HE was not analyzed in the model because most of the included patients did not have HE. The results of the multivariate analysis showed that the indication (variceal bleeding or ascites), shunt reasonability (reasonable or unreasonable), indocyanine green retention rate at 15 min (ICGR15), preoperative and postoperative portal venous pressure gradient (pre-PPG and post-PPG), percentage of PVP decrease (PVP%) and Tbil were found to be independent factors affecting survival after TIPS placement. The pre-PPG was not included in the final model because the overall C statistic of the model decreased by 0.45% (P= 0.17), and there was a correlation between the pre-PPG and post-PPG (Spearman correlation coefficient 0.62,P< 0.05). Using the regression coefficients (Table 2), the linear predictor was calculated as follows: Linear predictor = 1.45 × indication (0-variceal bleeding, 1-ascites) or 1 × indication (0-variceal bleeding, 1-both) + 1.83 × shunt reasonability (0-unreasonable, 1-reasonable) + 0.05 × ICGR15 + 0.27 × post-PPG + (-0.04) × PVP% + 2.24 × Log10(Tbil). Finally, the newly developed Cox (NDC) model was developed in the form of a nomogram (Figure 3).

Table 2 Univariate and multivariate Cox proportional hazards regression models for prognostic factors after transjugular intrahepatic portosystemic shunt placement

Figure 3 Nomogram of the newly developed Cox model for predicting 6-year survival after transjugular intrahepatic portosystemic shunt implantation in patients with hepatitis cirrhosis. ICGR15: Indocyanine green retention rate at 15 min; PVP: Portal venous pressure; Tbil: Total bilirubin.
Discrimination and calibration of the NDC model
The discrimination of the NDC score was assessed by calculating the AUCs for predicting 6-year survival compared to the Child-Pugh, MELD, MELD-Na, and FIPS scores (Table 3, Figure 4). The NDC score predicted 6-year survival with AUCs of 0.906 in the training set and 0.956 in the validation set, which were distinctly better than those of the Child-Pugh score [0.689 (P= 0.002) and 0.670 (P= 0.007)], the MELD score [0.649 (P= 0.001) and 0.661 (P= 0.007)], the MELD-Na score [0.666 (P= 0.001) and 0.748 (P= 0.02)], and the FIPS score [0.583 (P< 0.001) and 0.691 (P= 0.02)]. The excellent calibration of the nomogram was observed in the calibration plots (Figure 5), which were used to analyze the consistency between the observed and predicted probabilities.

Table 3 The areas under the receiver operating characteristic curves of the newly developed Cox model compared to those of the Child-Pugh, model for end-stage liver disease, model for end-stage liver disease-sodium and the Freiburg index of post-transjugular intrahepatic portosystemic shunt survival models

Figure 5 Calibration plots for the actual and predicted probabilities of the nomograms predicting 6-year survival after transjugular intrahepatic portosystemic shunt. A: The training cohort; B: The validation cohort.
According to the median risk score of the training set (3.85), the training set and the test set were divided into a highrisk group and a low-risk group (patients with a risk score of 3.85 were classified as the low-risk group, and patients with a risk score > 3.85 were classified as the high-risk group). K-M survival analysis was performed for the high- and low-risk groups in the training set and validation set, and the results showed that the survival prognosis was worse in the highrisk group than in the low-risk group (P< 0.001; Figure 6).

Figure 6 Kaplan-Meier survival plot of overall survival after transjugular intrahepatic portosystemic shunt in patients with hepatitis cirrhosis, stratified according to the newly developed Cox risk groups. A: The training set; B: The validation set.
DISCUSSION
It has been widely accepted that TIPS placement can be an important treatment for the complications of portal hypertension[3,4]. The survival rate following the TIPS procedure has demonstrated consistent improvement owing to technological advancements and innovations, despite the occurrence of certain complications associated with shunting, including HE and liver failure. However, the survival rate after TIPS placement can be influenced by various factors, such as the patient's condition, the presence of comorbidities, intraoperative techniques and the severity of liver disease[11,20]. It is important to identify patients at high risk of poor outcomes in clinical practice before deciding whether to perform the TIPS procedure. To accurately predict the postoperative outcome of TIPS patients, a series of liver scoring models have been developed. The MELD score, which has been used to predict short-term (3-month) survival after TIPS placement, has remained the best validated prognostic tool for patients with liver disease[21]. The MELD score is based on the serum Cr concentration, Tbil concentration, and international normalized ratio; these levels are labile and can be altered by the inherent disease state and iatrogenic interventions. Therefore, its predictive value declines dramatically over time. Additionally, the MELD score has been demonstrated to overestimate mortality[22]. The MELD-Na score, an updated version of the MELD score that includes the serum sodium concentration along with other MELD variables, has replaced the MELD score for organ allocation in liver transplantation. Several studies have compared the performance of the MELD and MELD-Na scores in predicting mortality after TIPS placement, and the MELD score has shown superiority[23]. The Child-Pugh score is also widely used for predicting the prognosis of patients with cirrhosis and can be used to determine the necessary treatment and need for liver transplantation. Nevertheless, the score has certain limitations, such as the failure to account for renal function and the subjective assessment of ascites and encephalopathy[24]. In 2021, Bettingeret al[12] constructed a new scoring model (FIPS) based on Tbil, Cr, age and albumin to predict the survival outcome of patients six months after TIPS. Importantly, the FIPS has not been validated in all populations, and its performance may vary depending on the population studied[25]. However, there are currently few models for predicting long-term survival after TIPS placement.
In the present study, we revealed that the indications for TIPS, shunt reasonability, post-PPG, PVP%, ICGR15 and Tbil were independent long-term prognostic factors in hepatitis cirrhosis patients. Ascites is associated with a higher mortality rate than variceal bleeding is, suggesting that it is a better indicator of advanced cirrhosis. Standards for shunt reasonability have been introduced previously. Importantly, the quality of the shunt tract is influenced by numerous factors, including portal vein pressure, stent selection, shunt location, stent extension into the IVC, portal vein length, blood flow, shunt angle, diameter, morphology, and other related variables. The post-PPG and PVP percentages reflect hemodynamic changes after TIPS placement and can be used to assess the effectiveness of surgery. The ICGR15 and total bilirubin concentration are both used to assess liver function. The NDC model containing the above indicators performed better than did the Child-Pugh, MELD, MELD-Na and FIPS scores in predicting long-term survival. Our study used the median score as a cutoff to stratify patients into two groups according to prognostic risk. K-M analysis revealed that the difference was highly significant, indicating that patients with a risk score > 3.85 should undergo closer follow-up after TIPS placement.
This study has several limitations. The patients included in this study were mainly those with hepatitis cirrhosis, and the other four scoring models were mainly based on Western populations with alcoholic cirrhosis. The inconsistency of the characteristics, occurrence, and development of liver injury in patients with cirrhosis of various etiologies may contribute to potential bias in model accuracy. Moreover, in this study, the patients’ renal function was basically normal, and their serum Cr and urea nitrogen levels were basically within the normal ranges, which may reduce the overall predictive performance of models containing the serum Cr concentration as a scoring factor. Additionally, it needs to be confirmed whether Cr can be used as an index for long-term survival in patients with cirrhosis in China following TIPS surgery. This study is also limited by the fact that it was a single-center retrospective analysis with a certain number of participants who were lost to follow-up, potentially resulting in a statistically significant reduction in the mortality rate.
In conclusion, we developed a new prognostic model to predict long-term survival in patients with hepatitis cirrhosis after TIPS placement, which can help identify high-risk patients and guide follow-up management after TIPS implantation. It will be important to conduct further studies with larger sample sizes to test this new model in the future, particularly through prospective, multicenter trials.
CONCLUSION
The NDC model can accurately predict long-term survival after the TIPS procedure in patients with hepatitis cirrhosis, help identify high-risk patients and guide follow-up management after TIPS implantation. Notably, the development of the NDC model offers a robust tool for predicting long-term survival post-TIPS, surpassing traditional models such as the Child-Pugh, MELD, MELD-Na, and FIPS in terms of accuracy and reliability. However, there is still a need for more comprehensive prediction models leveraging large-sample, multicenter datasets to improve the assessment of long-term survival in patients undergoing TIPS placement in the future.
ARTICLE HIGHLIGHTS
Research background
The transjugular intrahepatic portosystemic shunt (TIPS) represents a therapeutic modality for addressing complications associated with portal hypertension. This technique involves the creation of shunt pathways within the hepatic parenchyma, connecting the hepatic vein and the portal vein. The TIPS represents a valuable interim tool for patients with cirrhosis who are experiencing decompensation, as well as for individuals awaiting liver transplantation. Its applications encompass the management of conditions such as esophageal variceal bleeding and refractory ascites related to portal hypertension. However, there have been no specific studies on predicting long-term survival after TIPS placement.
Research motivation
The pressing need for a more accurate model for assessing long-term survival rates to guide treatment decisions in patients with chronic liver disease is emphasized. Therefore, we are committed to developing a model to predict the longterm survival of patients with hepatitis cirrhosis after TIPS.
Research objectives
The aim of our study was to establish a model to predict long-term survival in patients with hepatitis cirrhosis after the TIPS procedure.
Research methods
We conducted a retrospective study of 224 patients with PHT who received elective therapy and randomized them into training and validation sets. Continuous variables are presented as the mean with standard deviation, and categorical variables are presented as absolute and relative frequencies [n(%)]. Student’sttest or the Mann-WhitneyUtest was used to assess the differences in quantitative variables between the groups. The chi-square test was used for analyzing unordered categorical variables, while the Mann-WhitneyUtest was applied for examining ordered categorical variables. The Kaplan-Meier method was used to analyze differences in mortality risk among patients at different scoring levels, which were tested using the log-rank test. Cox regression was used to analyze the effect of each scoring model on the long-term prognosis of patients treated with the TIPS procedure. Receiver operating characteristic (ROC) curves and calibration curves were used to evaluate the discrimination and calibration ability of the models. A nonparametric approach (Delong-Delong & Clarke-Pearson) was used for pairwise comparisons of the area under the ROC curves.
Research results
We devised a newly developed Cox (NDC) model for predicting long-term survival after TIPS in patients with hepatitis cirrhosis, which outperformed existing scoring models, such as the Child-Pugh, model for end-stage liver disease (MELD), MELD-sodium (MELD-Na) and the Freiburg index of post-TIPS survival (FIPS) scores, for predicting long-term survival.
Research conclusions
The NDC model can accurately predict long-term survival after the TIPS procedure in patients with hepatitis cirrhosis, help identify high-risk patients and guide follow-up management after TIPS implantation. Notably, the development of the NDC model offers a robust tool for predicting long-term survival post-TIPS, surpassing traditional models such as the Child-Pugh, MELD, MELD-Na and FIPS in terms of accuracy and reliability.
Research perspectives
We can learn from this study that the NDC model can predict long-term survival after TIPS, and its performance was better than that of other scores, such as Child-Pugh, MELD, MELD-Na and FIPS. Future studies should focus on developing more comprehensive prediction models with large-sample, multicenter datasets to improve the assessment of long-term survival in patients who underwent TIPS placement.
FOOTNOTES
Co-first authors:Yi-Fan Lv and Bing Zhu.
Author contributions:Lv YF and Zhu B analyzed the data and wrote the paper; Meng MM, Wu YF, Dong CB, Zhang Y, Liu BW, You SL and Lv S performed the research; Liu FQ and Yang YP designed the research; Liu FQ and Yang YP reviewed and edited the manuscript; Lv YF and Zhu B contributed equally to this work as co-first authors; All the authors read and approved the manuscript.
Supported bythe Talent Training Plan during the "14th Five-Year Plan" period of Beijing Shijitan Hospital Affiliated to Capital Medical University, No. 2023LJRCLFQ.
Institutional review board statement:The study was reviewed and approved by the Beijing Shijitan Hospital Institutional Review Board and was performed in accordance with the Declaration of Helsinki.
Informed consent statement:All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
Conflict-of-interest statement:The authors declare that they have no conflicts of interest.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Yi-Fan Lv 0000-0002-0339-8822; Bing Zhu 0000-0003-0190-6384; Ming-Ming Meng 0000-0003-3560-1052; Yi-Fan Wu 0000-0003-2709-2729; Cheng-Bin Dong 0000-0003-1643-1460; Yu Zhang 0000-0001-9895-175X; Bo-Wen Liu 0000-0001-8837-7870; Shao-Li You 0000-0001-8689-8509; Sa Lv 0000-0003-0156-0766; Yong-Ping Yang 0000-0002-8307-1095; Fu-Quan Liu 0000-0003-1972-7712.
S-Editor:Zhang H
L-Editor:A
P-Editor:Xu ZH
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Actuality and underlying mechanisms of systemic immuneinflammation index and geriatric nutritional risk index prognostic value in hepatocellular carcinoma
- Mutational landscape of TP53 and CDH1 in gastric cancer
- Phospholipase A2 enzymes PLA2G2A and PLA2G12B as potential diagnostic and prognostic biomarkers in cholangiocarcinoma
- Classification of anatomical morphology of cystic duct and its association with gallstone
- Will partial splenic embolization followed by splenectomy increase intraoperative bleeding?
- Influence of donor age on liver transplantation outcomes: A multivariate analysis and comparative study