Role of Oncostatin M in the prognosis of inflammatory bowel disease: A meta-analysis
2024-03-07YueYangKanZuoFuGuPan
Yue Yang,Kan-Zuo Fu,Gu Pan
Abstract BACKGROUND Oncostatin M (OSM) is a pleiotropic cytokine which is implicated in the pathogenesis of inflammatory bowel disease (IBD).AIM To evaluate the prognostic role of OSM in IBD patients.METHODS Literature search was conducted in electronic databases (Google Scholar,Embase,PubMed,Science Direct,Springer,and Wiley).Studies were selected if they reported prognostic information about OSM in IBD patients.Outcome data were synthesized,and meta-analyses were performed to estimate standardized mean differences (SMDs) in OSM levels between treatment responders and non-responders and to seek overall correlations of OSM with other inflammatory biomarkers.RESULTS Sixteen studies (818 Crohn’s disease and 686 ulcerative colitis patients treated with anti-tumor necrosis factor-based therapies) were included.OSM levels were associated with IBD severity.A meta-analysis found significantly higher OSM levels in non-responders than in responders to therapy [SMD 0.80 (0.33,1.27);P=0.001],in non-remitters than in remitters [SMD 0.75 (95%CI: 0.35 to 1.16);P < 0.0001] and in patients with no mucosal healing than in those with mucosal healing [SMD 0.63 (0.30,0.95);P < 0.0001].Area under receiver operator curve values showed considerable variability between studies but in general higher OSM levels were associated with poor prognosis.OSM had significant correlations with Simple Endoscopic Score of Crohn’s disease [r=0.47 (95%CI: 0.25 to 0.64);P < 0.0001],Mayo Endoscopic Score [r=0.35 (95%CI: 0.28 to 0.41);P < 0.0001],fecal calprotectin [r=0.19 (95%CI: 0.08 to 0.3);P=0.001],C-reactive protein [r=0.25 (95%CI: 0.11 to 0.39);P < 0.0001],and platelet count [r=0.28 (95%CI: 0.17 to 0.39);P < 0.0001].CONCLUSION OSM is a potential candidate for determining the severity of disease and predicting the outcomes of anti-tumor necrosis factor-based therapies in IBD patients.
Key Words: Inflammatory bowel disease;Crohn’s disease;Ulcerative colitis;Oncostatin M;Prognosis
lNTRODUCTlON
Inflammatory bowel disease (IBD) is a disease of the gastrointestinal tract with two main types: Crohn’s disease,and ulcerative colitis.Crohn's disease can affect any part of the gastrointestinal tract,whereas ulcerative colitis mainly affects the colon.IBD may arise at any age but usually onsets at early adulthood[1].Primary surgery is required for approximately 32%,55%,70%,and 82% of Crohn’s disease patients after 5,10,15,and 20 years of diagnosis,respectively[2].It is speculated that an altered immune response to gut flora depending on individual's hereditary variability and environmental influences may be involved in the etiology of IBD.Age at onset,location,behavior,perianal disease in Crohn's disease and disease extent in ulcerative colitis are important determinants of disease condition[3].
There is an increasing trend in the prevalence of IBD.In the United States,the prevalence of IBD has increased from 0.8% (1.8 million) in 1999 to 1.3% (3 million) in 2015[4].Globally,the prevalence of IBD is rising in newly industrialized countries[5].Concomitantly,the prevalence rates of pediatric-onset IBD are also increasing even in regions where this disease was not previously reported[6].IBD is clinically difficult-to-treat disease that affects younger individuals and leads to long-term morbidity.Resistance to therapeutic agents is a hallmark of its management that necessitates personalized medicine research and development.Use of alternative drugs is frequent,but prediction of disease course and response to a particular therapy can profoundly benefit to patients.
IBD is a lifelong incurable disease that alternates with remission and relapse.Management may require 5-aminosalicylates,thiopurines,steroids,and biologics such as antibodies against tumor necrosis factor alpha (TNFα),vedolizumab,ustekinumabetc.[7].TNFα is involved in IBD onset and progression.Anti-TNFα antibody-based drugs including infliximab,adalimumab,certolizumab,and golimumab are the mainstay in the treatment of IBD[8].However,about 40% of patients do not respond to anti-TNF therapies,and among those who initially respond,several develop resistance to treatment.This necessitates IBD research to focus not only on the development of newer drugs,but also to identify biomarkers that can predict response to a therapy in advance[9].
Oncostatin M (OSM) is a proinflammatory cytokine belonging to the interleukin-6 family.OSM is produced mostly in hematopoietic tissues including T-lymphocytes,monocytes,macrophages,dendritic cells,neutrophils,eosinophils,and mast cells[10].It is a pleiotropic factor that participates in several organismic processes including hematopoiesis,differentiation,regeneration,and inflammation.On the other hand,several pathological processes including arthritis,ossification,dermatitis,fibrosis,gingivitis,and carcinogenesis are found to have OSM mediation[11].In colorectal cancer,higher OSM levels are associated with advanced disease and metastasis[12].One of the major pathological processes in which the involvement of OSM has been found critical is the inflammation of various parts including the joints,skin,lungs,and intestine[10].
The role of OSM in the pathogenesis of IBD was first described in a discovery of single nucleotide polymorphism in OSM receptors[13].OSM mediates its effects by binding to a glycoprotein called gp130 and this complex then activates the OSM receptor for signaling[14].OSM is highly expressed in inflamed mucosa of IBD patients in comparison with normal individuals.Elevated OSM levels are also found in serum of IBD patients.Moreover,higher OSM levels are observed in first-degree relatives of multiple-affected families in comparison with normal families[15].Several studies have evaluated the prognostic role of OSM in IBD patients.However,there are variabilities in the degree of associations between OSM and disease or interventional outcomes.This necessitates a systematic review of this area.The aim of the present study was to identify studies that evaluated the prognostic role of OSM in IBD patients in order to synthesize the reported outcomes and to perform meta-analyses of statistical indices for seeking up-to-date evidence of the prognostic role of OSM in IBD prognosis.
MATERlALS AND METHODS
Inclusion and exclusion criteria
Studies were included in this meta-analysis if they: (1) Evaluated IBD patients receiving a therapy who were subjected to OSM measurements in serum or tissue;(2) evaluated prognostic role of OSM in predicting disease outcomes and reported statistical indices of this relationship;and (3) reported correlations between baseline OSM and other important indicators of disease.Exclusion criteria were: (1) Studies involving the prognostic role of OSM in combination with other biomarkers;(2) molecular studies not providing any prognostic outcome;(3) molecular studies evaluating a possible role of OSM in IBD therapeutics;(4) preclinical studies;and (5) reviews and congress abstracts.
Literature search
The literature search was conducted in electronic databases (Google Scholar,Ebsco,PubMed,Science Direct,Springer,and Wiley) using the most relevant keywords.Primary search strategy was: Inflammatory bowel disease OR Crohn’s disease OR ulcerative colitis AND oncostatin M AND prognosis OR prognostic OR predictor.The literature search encompassed original research articles published in English language from the date of inception of the database till September 2023.
Data analysis
The quality assessment of the included studies was performed with the Newcastle-Ottawa Scale for the Quality Assessment of Observational Studies.Demographic information,disease pathological indices,previous treatments,study design and conduct features,and study outcome data including OSM levels at baseline,OSM levels in association with response,remission,and mucosal healing rates,statistical data depicting the relationship between baseline OSM levels and outcomes of disease,and correlation coefficients between OSM and other variables of IBD etiology were extracted from research articles of the included studies and were organized in datasheets.Important characteristics of the included studies were tabulated,and outcome data were synthesized for use in analyses.
Area under the receiver-operator curve (AUC) values depicting the relationship between OSM and disease indicators including response rate,remission rate,and mucosal healing rate reported by individual studies were tabulated.A metaanalysis of standardized mean differences (SMDs) in OSM levels between responders and non-responders,remitters and non-remitters,and in patients with mucosal healing and no mucosal healing was performed.Correlation coefficients between OSM and other variables of disease etiology reported by the individual studies were first converted to z-scores and were pooled under random-effects model by deriving variance from respective sample sizes.Overall estimates were back transformed into correlation coefficients.
RESULTS
Sixteen studies[16-31] were included in this review (Figure 1).In these studies,1353 IBD (818 Crohn’s disease and 686 ulcerative colitis) patients were evaluated.Important characteristics of the included studies are presented in Supplementary Tables 1 and 2.The quality of these studies was generally good.The lack of unexposed cohort was the main constraint which was observed for 7 studies.One of the included studies was double-blind,randomized,placebocontrolled with high quality.An assessment of the quality of other included studies with the Newcastle-Ottawa Scale is presented in Supplementary Table 3.

Figure 1 A flowchart of study screening and selection process.OSM: Oncostatin M;IBD: Inflammatory bowel disease.
OSM levels in patients with Crohn’s disease and ulcerative colitis were generally similar.In Caoet al[18],fecal OSM levels (mean ± SD;pg/mL) were 7 ± 3 in Crohn’s disease and 11 ± 4 in ulcerative colitis patients.In Caoet al[19],serum OSM levels (mean ± SD;pg/mL) were 119.4 (range: 34.8 -240.6) in Crohn’s disease and 122.1 (range: 58.7 -294.9) in ulcerative colitis patients.In Verstocktet al[28],OSM expression levels (NPX;OLINK proximity extension technology values) were 6.4 (IQR: 5.5,7) in Crohn’s disease and 6.5 (IQR: 4.35,4.9) in UC patients.In the study of Westet al[29],log 2 OSM mRNA expression levels relative to control were 5 (IQR: 4,8) in Crohn’s disease and 5.2 (IQR: 4.5,7) in ulcerative colitis patients.
However,OSM levels were associated with disease severity.In Caoet al[18],fecal OSM levels (mean ± SD;pg/mL) were 7 ± 2 in mild,8 ± 5 in moderate,and 14 ± 4 in severe IBD cases whereas in Caoet al[19],serum OSM levels (mean ± SD;pg/mL) were 10 ± 27 in mild,220 ± 240 in moderate,and 340 ± 150 in severe IBD cases.Mohamedet al[24] reported serum OSM levels to be 109.5 ± 25.5 in mild,116.2 ± 27.6 in moderate,and 144.8 ± 33.5 in severe IBD cases.In Westet al[29],OSM expression relative to control was 2 (IQR: 0,2.2) in mild,5 (IQR: 4,5.2) in moderate,and 4 (IQR: 3,4.5) in severe IBD cases.
A meta-analysis found significantly higher OSM levels in non-responders than in responders to therapy [SMD 0.80 (95%CI: 0.33 to 1.27);P=0.001].OSM levels were also significantly higher in non-remitters in comparison with remitters [SMD 0.75 (95%CI: 0.35 to 1.16);P< 0.0001] and in patients with no mucosal healing than in those with mucosal healing [SMD 0.63 (95%CI: 0.30 to 0.95);P< 0.0001;Figure 2].OSM levels and tissue expression data of all included studies are presented in Supplementary Table 4.

Figure 2 A forest graph showing the outcomes of a meta-analysis of standardized mean differences between responders and nonresponders,remitters and non-remitters,and mucosal healers and non-healers of anti-tumor necrosis factor-based therapies in patients with inflammatory bowel disease.OSM: Oncostatin M;TNF: Tumor necrosis factor;SMD: Standardized mean difference.
A synthesis of AUC values of treatment outcomes revealed that anti-TNF treatment had poor outcomes in patients with higher OSM levels in most studies (Tables 1 and 2).AUC values of OSM predicting the response of anti-TNF treatment in IBD patients ranged from 0.56 [95%CI: 0.31 to 0.82] to 0.91 [95%CI: 0.81 to 1.0] whereas the AUC values of OSM in distinguishing between responders and non-responders (including remission and mucosal healing) to anti-TNF therapy ranged from 0.52 to 0.9.Two studies did not report numeric data.Among these,O’Connellet al[26],who studied 21 patients with ulcerative colitis,did not find an association of pretreatment colonic OSM expression with the outcomes of infliximab therapy,and Mateoset al[21],who studied 22 patients with Crohn's disease,reported that OSM levels measured before induction therapy predicted response to infliximab treatment.
The correlation coefficients between OSM and Simple Endoscopic Score and Mayo Endoscopic Score were 0.47 [95%CI: 0.25 to 0.64] (P< 0.0001) and 0.35 [95%CI: 0.28 to 0.41] (P< 0.0001) respectively.The correlation coefficients between OSM and fecal calprotectin,C-reactive protein,and platelet count were 0.19 [95%CI: 0.08 to 0.3] (P=0.001),0.25 [95%CI: 0.11 to 0.39] (P< 0.0001),and 0.28 [95%CI: 0.17 to 0.39] (P< 0.0001) respectively (Figure 3).The correlation coefficients between OSM and other inflammatory/hematological markers observed in the included studies are given in Supplementary Table 5.
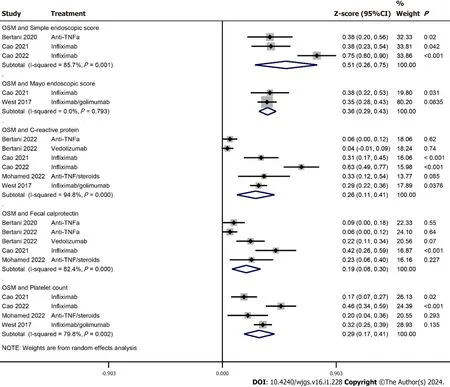
Figure 3 A forest graph showing the outcomes of a meta-analysis of correlation coefficients between baseline Oncostatin M and other baseline inflammatory biomarkers/disease indicators. OSM: Oncostatin M;TNF: Tumor necrosis factor.
DlSCUSSlON
OSM has emerged as an important biomarker for determining disease condition and response to anti-TNF therapies in IBD patients.Higher OSM levels are found to be associated with disease severity and therapeutic non-response.AUC values reported by the individual studies showed that higher OSM levels predicted poor response and could be used to distinguish responders from non-responders of anti-TNF therapy.OSM had significant correlations with Simple Endoscopic Score,Mayo Endoscopic Score,fecal calprotectin,C-reactive protein,and platelet count.
Where there is always a need to search for newer drugs,there is also a need to identify markers which can predict the effectiveness of a therapy in advance.Although C-reactive protein is a commonly used marker for predicting response to a therapy,it is non-specific to IBD[16,32,33].Fecal calprotectin is more important for IBD outcome prediction.Higher FC levels are found to be associated with no response to therapy[34-36].Caoet al[18] found higher AUC value for fecal calprotectin (0.834) than fecal OSM (0.763) in predicting response to anti-TNF therapy.In the meta-analysis of correlation coefficients,we have found a significant correlation between OSM and fecal calprotectin in IBD patients.
It has been observed that OSM predicts therapeutic response better to anti-TNF than to other pharmacological treatments.Bertaniet al[17] found OSM to be a useful biomarker for predicting response to anti-TNF therapy (AUC 0.91) but not to vedolizumab (AUC 0.56).Verstocktet al[28] also found low AUC values for distinguishing remitters from nonremitters after vedolizumab therapy both by serum OSM (0.51) and colonic OSM (0.685).Nishiokaet al[25] found a relatively higher AUC value for mucosal OSM expression in distinguishing resistant from sensitive patients to anti-TNF therapy (0.83) compared to ustekinumab (0.77).

Table 1 Area under receiver operator curve values for the prediction of treatment outcomes by the Oncostatin M
Minaret al[23] found no association between clinical remission and OSM 3 months after anti-TNF therapy but observed a significant association between OSM and clinical response one year after treatment.They suggested that duration of response evaluation may affect the outcomes.However,Caoet al[18] found higher AUC value (0.76) of serum OSM to predict nonresponse at week 28 in comparison with AUC value observed at week 54 of treatment (0.64).Verstocktet al[28] found no significant association between serum OSM and endoscopic remission after 6 months of anti-TNF therapy.On the other hand,Bertaniet al[16,17] and Guoet al[20] found significant associations between serum OSM and response to anti-TNF therapy after one year of treatment.
In a transcriptomic gene expression study,Zhouet al[31] found that on week 12 of PF-00547659 (anti-human mucosal addressin cell adhesion molecule-1 antibody) treatment the OSM expression and serum levels decreased profoundly from baseline in patients with ulcerative colitis who achieved response,remission,or mucosal healing.Whereas the change in serum OSM levels was 1.4-fold among responders,the change in OSM expression among responders and those achieving mucosal healing was 6.1-fold and 7.4-fold respectively[31].Verstocktet al[28] who found mucosal OSM to predict response to anti-TNF therapy,did not find serum OSM to do the same.In the study of Zhouet al[31],baseline OSM expression did not predict therapeutic outcomes.Whether this difference can be attributed to the mechanism of action of drug (PF-00547659vsanti-TNF based therapies) remains to be evaluated.OSM acts synergistically with TNF to promote inflammation in stromal cells and this phenomenon may not be exhibited by the other modulators such as human mucosal addressin cell adhesion molecule-1.
Verstocktet al[28] performed immunohistochemical staining on resected tissues and found OSM expression in the macrophages lying in superficial lamina propria as well as in the epithelial granulomas and multinucleated giant cells.In this study,macrophagic OSM expression had a strong correlation with mucosal OSM.OSM expression is found consistently higher in inflamed parts of intestine where it promotes inflammation in gut stromal cells in response to microbial challenges[22].O'Connellet al[26] who studied 21 acute severe ulcerative colitis patients observed a greater degree of immunostaining in the mucosal epithelial cells rather than stromal cells which provides impetus for studying OSM immunostaining in different IBD phenotypes.This study did not find an association between OSM expression levels and response to infliximab used as rescue therapy.
We found that OSM levels were not much different between patients with Crohn’s disease and those with ulcerative colitis[19,28,29].However,Caoet al[18] found fecal OSM levels to be significantly higher in patients with ulcerative colitisthan in Crohn’s disease.On the other hand,OSM levels were associated with disease severity as there was an increasing trend of OSM levels from mild,to moderate and severe disease[18,19,24,29].OSM levels are also found higher in IBD patients in comparison with healthy controls[18,21,24,28].These outcomes are similar to a study that characterized serum inflammatory protein profile and found a differential regulation of OSM between patients with ulcerative colitis and healthy controls but not between patients with Crohn's disease and ulcerative colitis[37].

Table 2 Area under receiver operator curve values for identifying/distinguishing treatment response by OSM
Although,most of the studies included herein identified OSM as a potential biomarker of IBD severity and predictor of response to anti-TNF therapies,some studies could not find so.Ezirike Ladipoet al[21] who studied 98 children with IBD reported that OSM or OSM receptor expression did not predict response to anti-TNF treatment,although OSM was associated with disease severity.Mohamedet al[24] reported that OSM did not have an appreciable ability to predict the response to therapy.O'Connellet al[26] also reported that colonic OSM expression was unable to predict infliximab treatment outcomes.Verstocktet al[28] reported that serum OSM levels had an AUC value of 0.52 in distinguishing between remitters and non-remitters after anti-TNF therapy.In the study of Zhouet al[31],baseline OSM levels were unable to predict response to PF-00547659.
Westet al[29] reported that among the 64 cytokines evaluated,the OSM and its receptor were most intensely overexpressed in the inflamed mucosa of IBD patients.They suggested that OSM may also be involved in developing resistance to anti-TNF therapies.According to Westet al[29],haematopoietically derived OSM appears to mediate intestinal pathology by promoting inflammatory behavior in gut-resident stromal cells which is a novel system of leukocyte-stromal cell cross talk that may have relevance in multiple mucosal tissues.Because of its stabilizing interactions with extracellular matrix components,OSM may play a critical role in the etiology of disease.Thus,OSM may act as an inflammatory amplifier and driver of disease chronicity by promoting chemokines,cytokines,and adhesion factor production from intestinal stromal cells.
There are some limitations of this review.There were inconsistencies in the outcome data of individual studies in measuring OSM levels/expression and their numerical presentations due to which not all data could be meta-analyzed.Moreover,in some studies,numerical outcome data were not accompanied by the variance.To account for such constraints,we either performed a meta-analysis of SMDs or tabulated the outcomes systematically.This constraint also precluded us from having a generalized estimate of OSM levels/concentrations.Moreover,for data where meta-analyses were possible,we observed higher statistical heterogeneity.Methodological differences of individual studies could have also played a role in the variabilities observed in this review.
CONCLUSlON
Most of the studies attempting to seek relationship between OSM and disease or treatment outcomes have found that higher OSM expression/levels to be associated with worse disease outcomes which shows that OSM can be used as a s surrogate marker of poor prognosis in IBD patients treated with anti-TNF treatments.This makes OSM an attractive biomarker for patient selection and clinical decision-making.However,some studies could not recognize such associations and others found non-significant correlations between OSM and other indicators such as fecal calprotectin,Creactive protein,and platelets.Therefore,more studies are required to validate present day evidence and to explore the behavior of OSM for IBD treatments other than anti-TNF drugs.
ARTlCLE HlGHLlGHTS
Research background
Oncostatin M (OSM) is a pleiotropic factor that participates in several physiological processes such as hematopoiesis,differentiation,regeneration,and inflammation,and pathological processes such as arthritis,ossification,dermatitis,fibrosis,gingivitis,and carcinogenesis.
Research motivation
Higher OSM levels in patients with inflammatory bowel disease (IBD) provided impetus for reviewing the outcomes of studies that evaluated the prognostic role of OSM in IBD patients.
Research objectives
The objective of this research was to systematically review relevant studies and perform meta-analyses of statistical indices for seeking current evidence about the role of OSM in IBD prognosis.
Research methods
After a literature search in electronic databases,studies were identified for synthesis.Meta-analyses were performed to estimate standardized mean differences in OSM levels between responders and non-responders,and to pool correlations of OSM with other inflammatory biomarkers.
Research results
OSM levels were associated with disease severity and were significantly higher in non-responders,in non-remitters,and in patients with no mucosal healing after anti-tumor necrosis factor (anti-TNF) therapy.Area under receiver operator curve values showed considerable variability between studies but in general higher OSM levels were associated with poor prognosis.OSM had significant correlations with Simple Endoscopic Score of Crohn’s disease,Mayo Endoscopic Score,fecal calprotectin,C-reactive protein,and platelet count.
Research conclusions
OSM can potentially determine IBD severity and can predict the outcomes of anti-tumor necrosis factor-based therapies.
Research perspectives
Future studies may refine the outcomes reported herein.It could also be interesting to explore the role of OSM in achieving response to non-anti-TNF therapies.
FOOTNOTES
Co-first authors:Yue Yang and Kan-Zuo Fu.
Author contributions:Yang Y and Fu KZ wrote the manuscript;Yang Y,Fu KZ,and Pan G collected and analyzed the data;all authors read and approved the final manuscript.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
PRlSMA 2009 Checklist statement:The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Gu Pan 0009-0009-9248-5714.
S-Editor:Gong ZM
L-Editor:A
P-Editor:Xu ZH
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Sarcopenia in cirrhotic patients: Does frailty matter while waiting for a liver transplant?
- Novel prognostic factors after radical resection of hepatocellular carcinoma: Updating an old issue
- Paravertebral block's effect on analgesia and inflammation in advanced gastric cancer patients undergoing transarterial chemoembolization and microwave ablation
- Predictive factors and model validation of post-colon polyp surgery Helicobacter pylori infection
- Practical effect of different teaching modes in teaching gastrointestinal surgery nursing
- Predictive value of NLR,Fib4,and APRl in the occurrence of liver failure after hepatectomy in patients with hepatocellular carcinoma