Predictive value of bilirubin and serum γ-glutamyltranspeptidase levels in type-2 diabetes mellitus patients with acute coronary syndrome
2024-01-26JieChenWanChaoZhangXiaoQiangTangRuoHanYinTaoWangXiaoYuWeiChangJiePan
Jie Chen,Wan-Chao Zhang,Xiao-Qiang Tang,Ruo-Han Yin,Tao Wang,Xiao-Yu Wei,Chang-Jie Pan
Abstract BACKGROUND Cardiovascular disease is a major complication of diabetes mellitus (DM).Type-2 DM (T2DM) is associated with an increased risk of cardiovascular events and mortality,while serum biomarkers may facilitate the prediction of these outcomes.Early differential diagnosis of T2DM complicated with acute coronary syndrome (ACS) plays an important role in controlling disease progression and improving safety.AIM To investigate the correlation of serum bilirubin and γ-glutamyltranspeptidase (γ-GGT) with major adverse cardiovascular events (MACEs) in T2DM patients with ACS.METHODS The clinical data of inpatients from January 2022 to December 2022 were analyzed retrospectively.According to different conditions,they were divided into the T2DM complicated with ACS group (T2DM+ACS,n=96),simple T2DM group (T2DM,n=85),and simple ACS group (ACS,n=90).The clinical data and laboratory indices were compared among the three groups,and the correlations of serum total bilirubin (TBIL) levels and serum γ-GGT levels with other indices were discussed.T2DM+ACS patients received a 90-day follow-up after discharge and were divided into event (n=15) and nonevent (n=81) groups according to the occurrence of MACEs;Univariate and multivariate analyses were further used to screen the independent influencing factors of MACEs in patients.RESULTS The T2DM+ACS group showed higher γ-GGT,total cholesterol,low-density lipoprotein cholesterol (LDL-C) and glycosylated hemoglobin (HbA1c) and lower TBIL and high-density lipoprotein cholesterol levels than the T2DM and ACS groups (P < 0.05).Based on univariate analysis,the event and nonevent groups were significantly different in age (t=3.3612,P=0.0011),TBIL level (t=3.0742,P=0.0028),γ-GGT level (t=2.6887,P=0.0085),LDLC level (t=2.0816,P=0.0401),HbA1c level (t=2.7862,P=0.0065) and left ventricular ejection fraction (LEVF) levels (t=3.2047,P=0.0018).Multivariate logistic regression analysis further identified that TBIL level and LEVF level were protective factor for MACEs,and age and γ-GGT level were risk factors (P < 0.05).CONCLUSION Serum TBIL levels are decreased and γ-GGT levels are increased in T2DM+ACS patients,and the two indices are significantly negatively correlated.TBIL and γ-GGT are independent influencing factors for MACEs in such patients.
Key Words: Acute coronary syndrome;Type-2 diabetes mellitus;Total bilirubin;Major adverse cardiovascular events
INTRODUCTION
Acute coronary syndrome (ACS) is a common cardiovascular disease (CVD) manifested by chest tightness and chest pain,which can cause heart failure,arrhythmia and even sudden death[1].In recent years,ACS,as the most serious ischemic heart disease,has become one of the primary causes of death worldwide[2].Despite the treatment recommended by current guidelines,some ACS patients are still at high risk of recurrent cardiovascular events.This risk is especially high among patients with type-2 diabetes mellitus (T2DM),who account for approximately one-third of ACS cases[3-5].T2DM is a frequently occurring disease,and diabetes,as is well known,has become one of the primary causes of morbidity and mortality in most countries[6].The incidence of diabetes is rising,affecting an estimated 346 million people worldwide[7],and the World Health Organization (WHO) predicts that it will be the seventh leading cause of death worldwide by 2030[8].CVD is one of the major complications of diabetes,causing 50% to 80% of early deaths.According to related research,ACS often occurs in patients with diabetes rather than nondiabetic patients.Overall,mortality from ACS is four times higher in men with diabetes and seven times higher in women with diabetes than in those without diabetes[9].In addition,a linear positive association has been reported between hyperglycemia on admission and post-ACS mortality[10].Therefore,early differential diagnosis of T2DM complicated with ACS plays an important role in controlling disease progression and improving safety.
Current studies have shown that serum γ-glutamyltranspeptidase (γ-GGT) can be used as a predictor of metabolic syndrome,and its level can reflect the severity of oxidative damage to cells by oxygen free radicals in the body,which is an early sensitive index to evaluate the degree of oxidative stress[11].Meanwhile,serum γ-GGT levels can reflect liver function,and an increase in its level is an independent risk factor for multiple CVDs[12].Recent studies have linked its elevated serum levels to many pro-atherosclerotic factors,such as insulin resistance,obesity,elevated plasma cholesterol levels,hypertension,and myocardial infarction[13-15].Therefore,γ-GGT levels can be detected to understand whether ACS occurs in T2DM patients in a timely manner,providing a clinical basis for diagnosis and treatment.Bilirubin (BIL) is a natural antioxidant factor in the body and is a kind of bile pigment formed by the metabolism of the end products after ferroheme decomposition.Total bilirubin (TBIL) is the decomposition product of senescent red blood cells[16],with a potent antioxidant capacity,which can remove harmful substances produced by oxidative stress and protect various organs of the body from damage[17].Elevated serum TBIL levels are a potential protective factor for the onset of T2DM[18].The human body has an antioxidant protection system.Peroxidation and antioxidant are in a dynamic balance under normal circumstances that cause no damage to the human body,but an imbalance between them can lead to increased lipid peroxidation[19].With the deepening of research on serum BIL,BIL has been found to be a member of the oxygenation system,which can protect lipid peroxidation[17] and protect lipids and lipoproteins from oxidation,reducing arterial damage and atherosclerotic plaques[20] and lowering the possibility of developing coronary heart disease or ACS[21].Heme oxygenase (HO) is the initiating enzyme and rate-limiting enzyme for BIL production and is available in HO-1 and HO-2 forms.Studies have shown that myocardial HO-1 activity in patients with acute myocardial infarction is obviously upregulated,and the serum TBIL level is strongly correlated with the occurrence of coronary artery disease[22].
However,whether serum TBIL and γ-GGT levels can be used as predictors of ACS in patients with T2DM and whether they are related to the incidence of major adverse cardiovascular events (MACEs) in T2DM+ACS patients has not been confirmed.Based on this,by studying changes in serum TBIL and γ-GGT levels in diabetes patients complicated with ACS and exploring their correlations with MACEs,this study provides more valuable information for the prognostic assessment of such patients and provides a theoretical basis for early clinical intervention in the future.
MATERIALS AND METHODS
Study subjects
The clinical data of inpatients in The Affiliated Changzhou No.2 People's Hospital of Nanjing Medical University from January 2022 to December 2022 were analyzed retrospectively.According to different conditions,patients were divided into the T2DM complicated with ACS group (T2DM+ACS,n=96),simple T2DM group (T2DM,n=85),and simple ACS group (ACS,n=90).Inclusion criteria were as follows: (1) T2DM patients all met the diagnostic criteria for T2DM formulated by the WHO,namely,fasting blood glucose ≥ 7.0 mmol/L or 2-hour postprandial blood glucose ≥ 11.1 mmol/L,and glycosylated hemoglobin (HbA1c) ≥ 6.5% (48 mmol/mol);(2) ACS patients had unstable angina,non-ST-segment and ST-segment elevation myocardial infarction confirmed by coronary angiography (CAG),electrocardiogram (ECG),dynamic ECG,and troponin level detection,with a stenosis ≥ 50% of at least one vessel;(3) the T2DM group received CAG and ECG after admission to confirm no coronary lesions;(4) patients in the T2DM+ACS group were confirmed by CAG and ECG to meet the above diagnostic criteria for T2DM and ACS;(5) patients had a normal mental state and cognitive function;and (6) patients had complete clinical data and follow-up information.The exclusion criteria were as follows: (1) Secondary diabetes caused by type 1 diabetes,gestational diabetes and other endocrine diseases;(2) constitutional jaundice,old myocardial infarction,symptomatic heart failure,pulmonary hypertension,and pulmonary heart disease;(3) digestive system diseases,abnormal liver function,lung diseases and malignant tumors;(4) renal dysfunction with an estimated glomerular filtration rate < 30 mL/(min·1.73 m2) or a history of renal replacement therapy,severe hepatic insufficiency with alanine transaminase or aspartate transaminase ≥ 5 times the upper limit of normal;(5) previous use of steroids,statins,etc.that affect liver or kidney function;and (6) incomplete clinical data and follow-up information.This study was approved by the Ethics Committee of The Affiliated Changzhou No.2 People's Hospital of Nanjing Medical University.
Outcome measures
(1) General data: Age,sex,body mass index (BMI),smoking status,alcohol consumption status and other basic information of all subjects were collected;(2) Laboratory examination: Fasting venous blood was collected from all patients the morning after patient admission and after 12 h of fasting and uniformly submitted for examination.Using a Hitachi 7600 automatic biochemical analyzer (Hitachi,Japan),TBIL,serum γ-GGT,total cholesterol (TC),triacylglycerol (TG),low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C),and HbA1c levels were quantified;and (3) Cardiac function tests: Echocardiography was performed using color doppler ultrasonography (Hewlett-Packard,United States) within 72 h of admission,mainly measuring left ventricular ejection fraction (LVEF).
Follow-up
All T2DM+ACS patients received a 90-day follow-up after discharge and were divided into either the event or nonevent group according to the occurrence of MACEs: Recurrent myocardial infarction,revascularization,heart failure,and cardiogenic death.
Statistical analyses
All analyses were performed in SPSS 25.0 at a significance level of α=0.05.Measurement data are expressed as the mean ± SD;ttest was used for intergroup comparisons,one-way analysis of variance for multigroup comparisons,and the lysergic acid diethylamide method for pairwise comparisons.Count data are expressed as percentages and were analyzed by theχ2test.Pearson linear correlation analysis was performed to determine the correlations of serum TBIL and γ-GGT levels with other indicators in T2DM patients with ACS.The influencing factors were analyzed by logistic regression.
RESULTS
General information
We collected the clinical data of each group for comparative analysis.No marked differences were identified in sex,age,BMI,drinking history,smoking history,or family history of coronary heart disease (P> 0.05),but the proportion of hypertension history was significantly different (P< 0.05),as shown in Table 1.

Table 1 Comparison of clinical data among groups
Laboratory indicators
Serum indices were significantly different among the three groups (P< 0.05).Specifically,the T2DM+ACS group exhibited notably higher γ-GGT,TC,LDL-C and HbAlc and lower left ventricular ejection fraction (LEVF),TBIL and HDL-C levels than the T2DM and ACS groups (P< 0.05),as shown in Table 2.
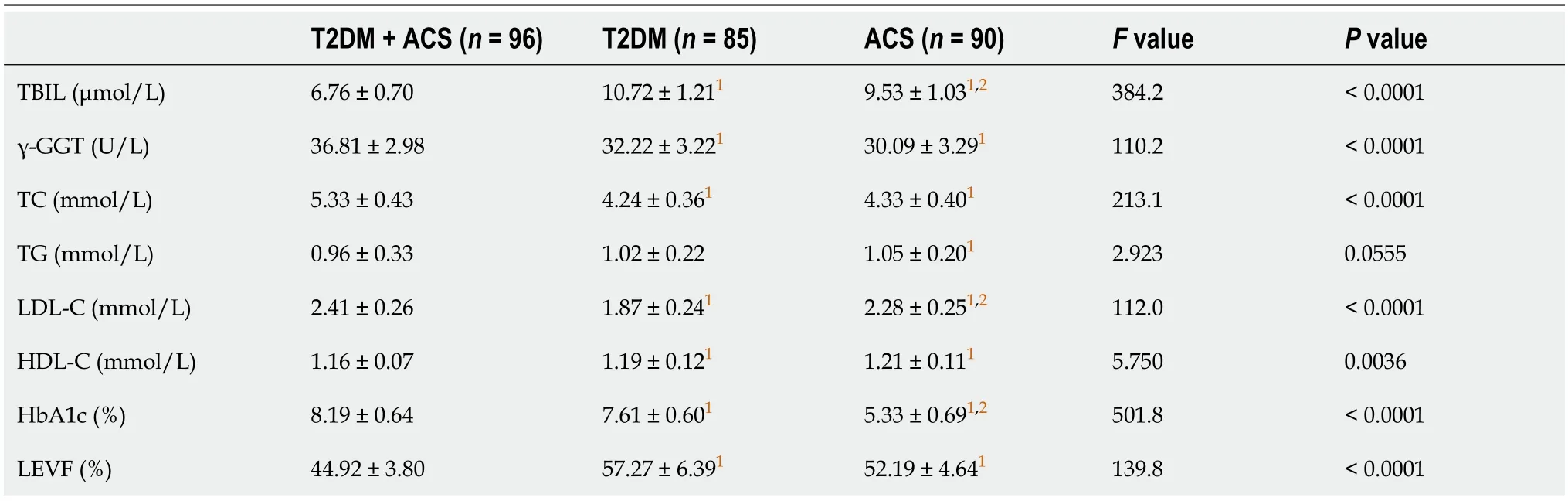
Table 2 Comparison of laboratory indexes among group
Correlation between TBIL level and other indices in the T2DM + ACS group
According to Pearson correlation analysis,serum TBIL was negatively correlated with γ-GGT,TC,LDL-C and HbAlc (P< 0.05) but was not related to TG,HDL-C and LEVF (P> 0.05),as shown in Table 3.

Table 3 Correlation between serum total bilirubin level and laboratory indexes
Correlations of γ-GGT level with other indices in patients in the T2DM + ACS group
As indicated by Pearson correlation analysis,serum γ-GGT was inversely associated with TBIL (P< 0.05) and positively correlated with TG and LDL-C (P< 0.05),but it had no correlation with TC,HDL-C,HbAlc or LEVF (P> 0.05),as shown in Table 4.

Table 4 Correlation between serum γ-glutamyltranspeptidase level and laboratory indexes
Univariate analysis of MACEs
Fifteen patients in the T2DM+ACS group developed MACEs,including 3 recurrent myocardial infarction,6 revascularization,3 heart failure and 3 cardiogenic deaths.No patients died in the nonevent group.Univariate analysis showed that age (t=3.3612,P=0.0011),TBIL levels (t=3.0742,P=0.0028),γ-GGT levels (t=2.6887,P=0.0085),LDL-C levels (t=2.0816,P=0.0401),HbA1c levels (t=2.7862,P=0.0065),and LEVF levels (t=3.2047,P=0.0018) were significantly different between the event and nonevent groups (P< 0.05),as shown in Table 5.

Table 5 Univariate analysis of major adverse cardiovascular events
Multivariate logistic regression analysis
Multivariate logistic regression analysis based on univariate results showed that age,serum TBIL,serum γ-GGT and LEVF were independent influencing factors of ACS in T2DM patients (P< 0.05),in which the TBIL level and LEVF was a protective factor,while age and γ-GGT levels were risk factors,as shown in Table 6.

Table 6 Logistic analysis of major adverse cardiovascular events
DISCUSSION
T2DM is an important factor causing atherosclerotic thrombosis.Insulin resistance and increased blood sugar can accelerate the development of atherosclerosis and increase the risk of ACS[23].The mechanism of T2DM-induced atherosclerosis and thrombosis is complicated and is mainly due to lipid metabolism disorders induced by persistent hyperglycemia that promotes lipid deposition,leading to a microinflammatory state in the body and promoting thrombosis[24].At present,there is still a lack of reliable indicators to evaluate the progression of T2DM complicated with ACS,and a great breakthrough has not been made in improving patient prognosis.Thus,it is necessary to seek ideal markers to provide a basis for clinical diagnosis and treatment.
This study explored serum TBIL and γ-GGT levels in T2DM patients with ACS and their correlations with MACEs.T2DM+ACS patients were found to have higher γ-GGT,TC,LDL-C and HbAlc levels than simple T2DM and ACS patients,while their levels of TBIL and HDL-C were significantly lower.In addition,serum TBIL was found to be inversely associated with γ-GGT,TC,LDL-C and HbAlc,but it had no correlation with TG and HDL-C.Serum γ-GGT was negatively correlated with TBIL and positively correlated with TG and LDL-C but not with TC,HDL-C or HbAlc.Both serum TBIL and HbA1c are risk factors for coronary heart disease.The former is a natural endogenous strong antioxidant with the functions of inhibiting lipid peroxidation,anti-ischemia and eliminating free radicals,which can protect LDL-C in the human body from oxidation[25].The latter is a common clinical index that plays a key role in the formation and development of atherosclerosis and is mainly formed by the (irreversible) enzymatic reaction of hemoglobin and glucose[26].BIL has been shown to prolong the survival time of ventricular myocytes by resistingoxygen free radical-induced damage.Gulluet al[27] showed that high BIL levels can protect coronary blood flow reserve and coronary microvascular endothelial function.BIL,with antioxidant and anti-inflammatory activities,has been reported to reduce atherosclerosisin vivo[28].Atherosclerosis is known to be the pathological basis of CVD[29].Erdoganet al[30] reported that increasing TBIL levels promote collateral angiogenesis in chronic total occlusion of the coronary artery.Furthermore,Bil can improve the activity of HO,which has an antiatherosclerotic effect[31].The isozyme HO-1 participates in the anti-stress ability of cardiovascular system tissues and cells under pathological conditions and maintains the integrity and constancy of cardiovascular system function[32].At the same time,Bil can increase cholesterol dissolution,promote cholesterol excretion from bile,reduce plasma cholesterol concentration,and prevent the development of atherosclerosis[33].This study found that the level of TBIL was negatively correlated with TC and LDLC,which also suggests that low Bil can be related to the occurrence of coronary heart disease through the increase in blood lipids.In patients with T2DM,glucose abnormalities are often accompanied by dyslipidemia,which together promote the formation of atherosclerotic plaques[34].Our experimental results also prove that the influence of elevated serum γ-GGT levels on ACS in T2DM patients is related to abnormal lipid metabolism.γ-GGT levels are highest in people with ACS and lowest in healthy people[35].Increased γ-GGT levels contribute to the development and progression of ACS caused by T2DM.In this study,Pearson analysis showed that γ-GGT was positively correlated with LDL-C and TG.It can be concluded that an increase in γ-GGT levels will cause abnormal lipid metabolism,a decrease in lipid peroxidation,the release of inflammatory factors,and damage to the vascular endothelium,which will affect the stability of plaques,causing damage to the plaques,increasing the plaque size,and inducing ACS.Moreover,LEVF levels were found to be significantly different between patients with MACEs and those without.Coronary artery microcirculatorydisorders may cause myocardial fibrosis and even cardiac insufficiency[36].Myocardial ischemia,hypoxia,and reperfusion injury ultimately lead to diastolic dysfunction[37].The measurement of LVEF can sensitively and specifically reflect changes in left ventricular function in left ventricular dysfunction and secondary ventricular remodeling[38].Studies have shown that the severity of coronary artery disease,myocardial ischemia,and myocardial cell injury or apoptosis are associated with decreased LVEF[39].Finally,through univariate and multivariate logistic analyses,age,LEVF,serum TBIL levels,and serum γ-GGT levels were confirmed as independent influencing factors of ACS in T2DM patients,of which the TBIL level and LVEF levels were protective factors,while age and γ-GGT levels were risk factors.
However,some limitations of this study need to be addressed.First,due to the fact that this is a single-center retrospective analysis,the research materials and subjects were limited,warranting a larger sample size for further analysis.Second,other risk factors for ACS such as socioeconomic status,dietary patterns,physical activity,hormone levels and medication were not included in our study.In addition,lipids,which are risk factors for ACS,were not discussed in this study.Third,the samples studied were hospital-based and may not be representative of the general T2DM patient population.Fourth,the sample size of this study was relatively small.Therefore,further studies with larger sample sizes and more measures are needed.
CONCLUSION
In summary,serum TBIL levels and serum γ-GGT levels can be used as indicators to assess patients’ condition and predict long-term adverse cardiovascular events in diabetes patients with ACS.However,as this is a retrospective,singlecenter study with a small sample size,it is necessary to increase the sample size for more in-depth clinical research on whether patients with ACS complicated with diabetes can be accurately evaluated and predicted based on the detection of serum TBIL and γ-GGT levels.
ARTICLE HIGHLIGHTS
Research background
To provide more credible clinical evidence for the prognostic assessment of type-2 diabetes mellitus (T2DM) patients complicated with acute coronary syndrome (ACS) and a theoretical basis for early clinical intervention in the future.
Research motivation
Serum total bilirubin (TBIL) levels and γ-glutamyltranspeptidase (γ-GGT) levels can be used as indicators to assess patients’ condition and predict long-term adverse cardiovascular events in T2DM patients with ACS.
Research objectives
T2DM+ACS patients were found to have higher γ-GGT,total cholesterol (TC),low-density lipoprotein cholesterol (LDLC) and glycosylated hemoglobin (HbA1c) levels than patients with T2DM or ACS alone,with significantly lower levels of TBIL and high-density lipoprotein cholesterol (HDL-C).In addition,serum TBIL was found to be inversely associated with γ-GGT,TC,LDL-C and HbAlc,but it had no correlation with triacylglycerol and HDL-C.Through univariate and multivariate logistic analyses,age,left ventricular ejection fraction (LEVF),serum TBIL levels,and serum γ-GGT levels were confirmed as independent influencing factors of ACS in T2DM patients,of which TBIL and LVEF levels were protective factors,and age and γ-GGT levels were risk factors.
Research methods
The clinical data of inpatients were analyzed retrospectively.According to different conditions,they were divided into the T2DM complicated with ACS group (T2DM+ACS,n=96),simple T2DM group (T2DM,n=85),and simple ACS group (ACS,n=90).The general data and laboratory indexes were compared among the three groups,and the correlations of serum TBIL and γ-GGT levels with other indicators were evaluated.T2DM+ACS patients received a 90-day follow-up after discharge and were further divided into event (n=15) and nonevent (n=81) groups according to the occurrence of major adverse cardiovascular events (MACEs).Univariate and multivariate analyses were further used to screen the independent influencing factors of MACEs in patients.
Research results
There is still a lack of reliable indicators to evaluate the progression of T2DM complicated with ACS,and a great breakthrough has not been made in improving patient prognosis.Therefore,it is necessary to seek ideal markers to provide a basis for clinical diagnosis and treatment.
Research conclusions
By studying changes in serum TBIL and γ-GGT levels in T2DM patients complicated with ACS and exploring their correlations with MACEs,it is confirmed that serum levels of TBIL and γ-GGT can be used to assess patients’ condition and predict long-term MACEs in such patients.
Research perspectives
Cardiovascular disease is one of the major complications of diabetes,causing 50%-80% of early deaths.According to related research,ACS often occurs in patients with diabetes rather than nondiabetic patients.
FOOTNOTES
Co-first authors:Jie Chen and Wan-Chao Zhang.
Author contributions:Chen J and Zhang WC conceived and designed the experiments;Chen J,Zhang WC,Tang XQ,Yin RH,Wang T and Pan CJ collected and analyzed the data;Wei XY and Pan CJ contributed to the data collection;Chen J and Zhang WC overall supervise the study.All authors have approved the manuscript.Chen J and Zhang WC contributed equally to this work and are co-first authors,including design of the study,acquiring and analyzing data from experiments,and writing of the actual manuscript.
Supported byScience and Technology Major Project of Changzhou Science and Technology Bureau,No.CE20 205047;Natural Science Foundation of Xinjiang Uygur Autonomo us Region,No.ZD 202220;Changzhou A major scientific research project of the Municipal Health Commission,No.2022D01F52.
Institutional review board statement:The study was reviewed and approved by the The Affiliated Changzhou No.2 People's Hospital of Nanjing Medical University (Approval No.YLJSA302).
Informed consent statement:Patients were not required to give informed consent to the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent.
Conflict-of-interest statement:There is no conflict of interest.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Ruo-Han Yin 0000-0003-1080-4582;Chang-Jie Pan 0000-0002-8464-4529.
S-Editor:Lin C
L-Editor:A
P-Editor:Chen YX
杂志排行

World Journal of Diabetes的其它文章
- Effects of Tai Chi in diabetes patients: Insights from recent research
- Management of monogenic diabetes in pregnancy: A narrative review
- Prediabetes: An overlooked risk factor for major adverse cardiac and cerebrovascular events in atrial fibrillation patients
- Clinical study of different prediction models in predicting diabetic nephropathy in patients with type 2 diabetes mellitus
- Heterogeneously elevated branched-chain/aromatic amino acids among new-onset type-2 diabetes mellitus patients are potentially skewed diabetes predictors
- Investigating the relationship between intracranial atherosclerotic plaque remodelling and diabetes using high-resolution vessel wall imaging