Refining core competencies of first-line nurse managers in the hospital context: A qualitative study
2023-11-26JokoGunwnYupinAungsurochMryFishrCollnMrzilliNzlinsyhEtyHstuti
Joko Gunwn ,Yupin Aungsuroch ,*,Mry L.Fishr ,Colln Mrzilli ,Nzlinsyh ,Ety Hstuti
a Faculty of Nursing, Chulalongkorn University, Bangkok, Thailand
b Indiana University School of Nursing, Indianapolis, IN, USA
c College of Nursing, University of Florida, Gainesville, FL, USA
d University of Maine, School of Nursing, Orono, ME, USA
e Department of Nursing, Politeknik Kesehatan Kementrian Kesehatan Pangkal Pinang, Bangka Belitung, Indonesia
f dr.H.Marsidi Judono General Hospital, Belitung, Indonesia
Keywords:Clinical competence Core competencies Head nurses Indonesia Social skills
ABSTRACT Objective: As the world moves towards a new normal,challenges continue to emerge while simultaneously inspiring us with new solutions.Strengthening the skills of first-line nurse managers(FLNMs)to fulfill a wide range of complex roles and responsibilities effectively necessitates refining core competency guidelines or standards.This study aimed to explore the perceived core competencies of Indonesian FLNMs within the context of the post-pandemic era.Methods: The study employed a qualitative descriptive design.Face-to-face interviews were conducted in a public hospital in Indonesia from January 2022 through August 2022.Seven head nurses with direct experience managing a unit during the COVID-19 pandemic were selected.The interviews were audiorecorded,transcribed verbatim,and validated by re-listening.Data were analyzed using thematic analysis.Results: Four main themes of the core competencies developed,including 1) managerial core competencies,2) clinical core competencies,3) technological core competencies,and 4) socio-emotional skills/personal traits consisting of the following:be brave,fast,patient,optimistic,consistent,and responsible.Conclusions: The findings demonstrate that the managerial and clinical core competencies of the FLNMs must be aligned,while technological core competencies are the mediating component of both.Personal traits are essential for FLNMs as they undergird the other three core competencies and the success of the FLNMs.
What is known?
· The COVID-19 crisis has emphasized the importance of first-line nurse managers acquiring additional skills,such as managing hybrid workflows,efficiently allocating human resources during emergencies,and implementing innovative leadership strategies.
· While several studies have explored the core competencies of nurse managers,there has been a shortage of specific focus on first-line nurse managers.Furthermore,these studies have predominantly been conducted before the pandemic and within country-specific contexts.
· Given the ongoing transition towards a new normal,refining the core competencies of first-line nurse managers in the hospital context is crucial to align with the evolving demands and challenges of the post-pandemic era.
What is new?
· The findings of this study offer valuable insights and serve as a foundation for hospital managers and nurse managers in developing their leadership plans,designing effective training and development programs,and creating assessment tools to evaluate the core competencies of first-line nurse managers.
· The identified core competencies,encompassing managerial,clinical,technological,and socio-emotional skills/personal traits,contribute to the existing body of nursing knowledge concerning the core competencies specific to first-line nurse managers.This research holds particular relevance in the context of post-pandemic situations,where the roles of first-line nurse managers have become more significant and multifaceted.
1.Introduction
Core competencies,defined as a set of skills,attributes,and behaviors necessary for employees in a specific role,significantly contribute to the effective performance of job responsibilities [1].For first-line nurse managers (FLNMs),core competencies encompass a combination of skills,knowledge,attitudes,and behaviors that enable them to navigate the complexities of the healthcare system,adapt to changing circumstances,and ensure the delivery of high-quality care for the success of healthcare organization[2,3].
The COVID-19 pandemic has significantly transformed various aspects of society over the past three years and profoundly impacted FLNMs.In addition to the fundamental changes in working,socializing,and mobility,FLNMs have faced unique challenges arising from the pandemic and the emergence of new events and diseases [4].This double burden has necessitated developing and enhancing core competencies among FLNMs to effectively manage these complex and evolving circumstances while adapting to different environments,maintaining care quality,and fulfilling hospitals’missions and visions[5].As the world transitions toward an endemic phase of COVID-19,FLNMs should prepare themselves by improving their core competencies and equipping themselves with the necessary support available to navigate the new normal conditions.The term “new normal” refers to the need to adapt to new ways of living and working since the world will not return to how it was before the pandemic.Therefore,FLNMs must be ready to face these new challenges and adapt to changing conditions[4].
Acknowledging the shifting roles and responsibilities of FLNMs,it becomes evident that the core competencies required to excel in their positions have also evolved.While existing core competencies may have been applicable before the pandemic,the COVID-19 crisis has highlighted the need for FLNMs to acquire additional skills,such as managing hybrid workflows,quickly allocating human resources in emergencies,demonstrating caring for their staff in offline and online settings,and implementing innovative leadership strategies amidst uncertainty,resource constraints,and increased patient loads [6].Furthermore,FLNMs have often found themselves directly involved in patient care[7].
FLNMs worldwide have implemented various strategies to address the challenges brought about by the pandemic effectively.For example,in Jordan,approaches included establishing support teams,field hospitals,and new units and modifying emergency plans and policies [8].In addition,efforts were made to enhance medical supplies,personal protective equipment (PPE),and safety standards,alongside providing virtual training for staff.These experiences enhanced leadership competencies and emphasized selfawareness and personal growth [8].Similar initiatives were observed in Egypt [9] and Spain [10],equipping FLNMs with disaster management competencies,ethical decision-making abilities,and competencies to navigate uncertainty and prioritize staff well-being.In addition,Iranian nurse managers required flexible and situational management to recruit,retain and compensate nurses [11] and emphasized the religious spirit as they served as role models for their staff during the pandemic [5].
Furthermore,regarding the current literature on core competencies,a recent study [3] identified eight essential competencies for nurse managers,including “decision-making,relationship management,communication skills,listening,leadership,conflict management,ethical principles,and collaboration and team management skills.” However,the study did not differentiate between the core competencies of different levels of nurse managers and focused on all nurse managers in the Spanish health system.Additionally,a scoping review [12] synthesized the most-cited competencies of nurse managers into 22 most-cited competencies,but these competencies were not specific to FLNMs.Moreover,a study in Ghana [13] examined essential management competencies based on Katz's model,which assessed technical,human,and conceptual skills without exploring other core competencies in the current context.
Therefore,it remains unclear whether the core competencies identified in previous studies adequately capture the core competencies required for FLNMs in Indonesia and best fit today's new normal.This raises important questions:Are the core competencies dimensions of FLNMs essentially different among countries or specific contexts? Are these skills necessarily required,or can we retain the same core competencies as before the pandemic?These cannot be answered without further evidence and validation.
To our knowledge,few published researches specifically examined FLNMs' core competencies as perceived by Indonesian nurse managers during and post-pandemic.While two local studies explored related topics,such as staff scheduling [14] and hospital preparedness during the early stages of the pandemic[15],they did not directly address FLNMs’ core competencies.Therefore,further investigation into this area is warranted.
To bridge the gap,our study aimed to explore the core competencies of Indonesian FLNMs within the context of the new normal.The research question for this study was “What are the perceived core competencies of Indonesian FLNMs in the post-pandemic era?” Understanding the core competencies in this context will inform the development of tailored standards and guidelines that empower FLNMs to effectively navigate future challenges,ensuring high-quality care and resilience in the face of uncertainties.
It is noteworthy that,although in international contexts,FLNMs are referred to by various titles such as ward managers,head nurses,ward sisters,unit managers,and charge nurses [2];however,in Indonesia,a first-line nurse manager refers to a clinical nurse holding positions such as head nurse,ward manager,ward head nurse,or unit manager.Charge nurses and ward sisters are not considered equivalent to FLNMs.The first-line nurse manager is known as “Kepala Ruangan” in Indonesian [2].
Moreover,it is common for the terms “first-line nurse managers”and“front-line nurse managers”to be used interchangeably,describing nurses in managerial positions responsible for overseeing daily operations within a specific unit.Generally,both terms denote the exact role of nursing management at the frontline.The variation in terminology can depend on the context,with“first-line nurse managers”emphasizing the hierarchical position and“frontline nurse managers” highlighting their direct involvement in patient care.In Indonesia,nurse managers are categorized into different levels within the management hierarchy.First-line nurse managers are classified as low-level managers,while middle managers include area managers and heads of sub-nursing departments.Top-level managers comprise the heads of nursing departments and directors or vice directors of nursing[2].Therefore,to align with the specific context of our study and maintain consistency,we exclusively utilized the term “first-line nurse managers” (FLNMs)throughout the article.
2.Methods
2.1.Study design
This study used a qualitative descriptive design as outlined by Lambert and Lambert[16].The design was a suitable choice for our research as it facilitated a direct and straight description of the phenomenon,especially the core competencies of Indonesian FLNMs.This design collected data from FLNMs and analyzed thematically,allowing for a comprehensive exploration of the core competencies.The focus was on providing a descriptive summary of the findings without requiring extensive theoretical competency development[16].This approach ensured that the study remained grounded in the participants’ experiences and perspectives,providing a clear and concise account of the FLNMs’ core competencies.There was no manipulation or commitment to any theoretical view in this design,as there was no philosophical or epistemological strand.The findings were purely derived from the data codes,reflecting the naturalistic inquiry [16].A qualitative descriptive design was selected over a grounded theory design as the constant comparative analysis was employed,but no theory was developed.In addition,the qualitative descriptive design was chosen over a phenomenological approach because it included less interpretive illustrative components [16].
2.2.Ethical consideration
The study approval was obtained from the Research Ethics Committee,Department of Health of Indonesia,Indonesia (Ref code: 800/0375/RSUD dr.H.M.JD,approved on January 27,2022).Study permission was also given by the hospital.Participants had to sign an informed consent with the stated study objectives to participate in this study.It is noted that this study was voluntary,and participants could withdraw from participation after data collection was concluded.Confidentiality of the data was highly maintained and stored in a secured computer.The researchers did not use real names in reporting the study.Instead,numbers were used (P1-P7).
2.3.Participants
Seven FLNMs were selected using purposive sampling.The advantage of purposive sampling is to enable researchers to obtain rich information from those who understand a phenomenon [17].The participants’ inclusion criterion was FLNMs who had direct experience managing a unit during the COVID-19 pandemic,specifically since the early stage of the crisis in Indonesia(from March 2020),to provide the actual phenomenon and details in the field,based on their perspectives.
2.4.Data collection
Data were collected from January 28,2022 to August 10,2022,in a public hospital in Belitung,Indonesia,after obtaining the study permit.The top nursing manager,as directed by the hospital director,assisted the researchers by providing the names and phone numbers of the FLNMs who had direct experience managing a unit during the COVID-19 pandemic.Subsequently,the researchers contacted the FLNMs through short message service (SMS) and phone calls.Additionally,the middle-line nurse manager contacted the FLNMs to encourage their participation in the study.All FLNMs,according to inclusion criteria,were invited to participate,and those who were available and accepted the invitation were scheduled for an interview at a mutually agreed upon time.
Semi-structured face-to-face interviews were the primary method for data collection.The interviews were audio-recorded,transcribed verbatim,and validated by re-listening.The interviews for this study were conducted by three researchers,namely NN,JG,and EH.Based on their convenience,the interviews took place either in a meeting room at the hospital or at the participant’s home.However,it should be noted that EH,who held a middle-line nurse manager position,participated in the interview only once.This decision was made to minimize potential response bias,as EH had a professional and hierarchical relationship with participants from the same institution.It is worth noting that NN and JG had no prior connection or significant relationship with the participants,as they were from different organizations,ensuring impartiality during the interviews.The interviews were conducted in Bahasa,or the Belitung language,to facilitate effective communication with the participants.
The interview questions can be seen in Table 1.There was no pilot testing of the interview guideline,as the questions were only for initial probing questions.In addition,the researchers also used chats,like WhatsApp,as an additional data collection method.However,this method was limited to clarifying the participants’responses if the recording was unclear during verbatim transcription.One participant sent her voice to answer the interviewer's questions through WhatsApp.The researchers' mobile phones automatically recorded the chats while the voices were transcribed verbatim and re-read.It should be noted that combining data collection from various sources in a single study yields reliable and trustworthy findings [18].
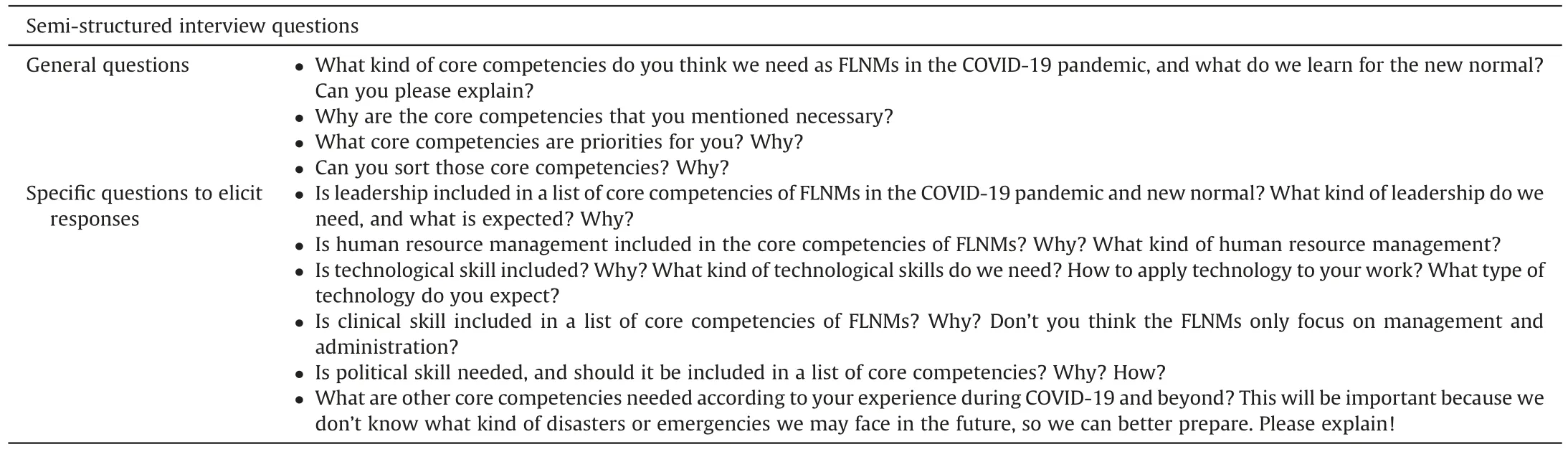
Table 1 Semi-structured interview questions.
The process was concluded when data were saturated occurred.It is noted that a content analysis of the interview data of each participant was done before the following interview.Therefore,the researchers/interviewers noticed if another participant provided the same responses.
The interview averaged about 50 min for each participant.In addition,there was one repeated interview (P3),and chats via WhatsApp were conducted several times to clarify the participants’answers.
2.5.Data analysis
A thematic analysis following Vaismoradi,Turunen,and Bondas[19] was employed.The process was comprised of 1) transcribing each interview,2) re-reading the transcripts several times and highlighting the codes that have meaning units,and 3)developing subthemes and themes by organizing,comparing,and contrasting the meaning units [19].This fundamental analysis relied on the explicit description with a lower interpretation level rather than the implicit meaning with a more profound interpretation[19,20].The findings were reported with no further theoretical analysis.Therefore,this thematic analysis was suitable for the qualitative descriptive study design.
Manual data analysis was done for this study.First,JG,NN,and EH performed initial transcription (verbatim),coding (144 codes),and developing categories,subthemes,and themes generated from the codes in the Indonesian language from August 10 to 30,2022.Next,all themes and participants’ quotes were translated into English,and the first drafts of the study report and manuscript were developed from August 30 to September 20,2022.A draft manuscript containing initial themes and all quotes was then shared with the research team on September 20,2022,and their feedback was used to refine the results.
The framework of Abfalter,Mueller-Seeger,and Raich [21] was utilized for the translation decisions,comprising seven elements.The first question consisted of why.The why was to develop scientific value among researchers and for dissemination to advance FLNM core competencies.The second question consisted of when.The when was from the initial draft development through the end of the study.The translation in the initial findings allowed all researchers to look at the data and identify if additional interviews were needed.The third question is what.The what consisted of interview data and all reports.The fourth question is who.The who consisted of the interview data and drafts that were translated by JG,NN,and EH.The fifth question is how.The how is JG did the translation from Bahasa to English,and NN and EH compared both versions for clarity.The sixth question is where.The where is within the English-speaking research team environment.The seventh question is by what means.The by what means is that language proficiency was ensured and no IT applications were used.
2.6.Rigor and trustworthiness
Multiple strategies were implemented to ensure rigor and trustworthiness in this study.Firstly,a peer review process involving nursing experts from the research team and an external researcher was conducted within two weeks to assess authenticity,objectivity,and credibility while ensuring the absence of bias or preconceived notions during the analysis and theme development stages.Secondly,member checking was performed on August 30,2022,allowing participants to review and confirm the thematic findings.Thirdly,the emerging codes,categories,and themes were checked and validated by all researchers through consensus.Fourthly,the research design,implementation,and data collection process were thoroughly described to ensure dependability.Finally,the researchers acknowledged their own positionality and potential biases,with one researcher (EH) minimizing her involvement in most interview sessions and participating in only one interview to mitigate bias.
3.Results
The participants in this study consisted of five females and two males aged 34-46 years.They have an average of four years’experience as an FLNM with a maximum of six years’ experience.Their experience with COVID-19 as an FLNM included working in isolation units,emergency units,ICUs,internal medicine,airborne and pulmonology,and perinatology care areas.In addition,the participants’ education levels comprised bachelor’s and diplomas in nursing,with clinical experience between six to 14 years.The detailed information can be seen in Table 2.

Table 2 Demographic characteristics of participants.
Four main themes of the core competencies developed: 1)managerial core competencies,2) clinical core competencies,3)technological core competencies,and 4)personality traits.Notably,researchers did not anticipate the emerging themes before the study.The themes are presented with exemplary quotes from the participants,with Participant No.(P1-P7)and Codes (C).
When he tried to follow her through aisles25 dense17 with racks of slips and brassieres and panties, all glimmering softly, a sales clerk in a navy blue dress with a white collar stopped him, smiling, to ask if she could help
3.1.Theme 1: managerial core competencies
Managerial core competencies refer to the primary set of skills,abilities,attributes,and behaviors required for FLNMs to implement particular managerial responsibilities.Seven subthemes were developed in this theme: 1) human resource management (with four categories: staffing,rewards,training,and performance evaluation),2) self-management,3) supply and equipment management,4)patient care management,5)knowledge management,6)leadership,and 7)unit budgeting.The detail of each subtheme and exemplar quotes can be seen in Table 3.
3.2.Theme 2: clinical core competencies
Clinical core competencies are the sets of skills,abilities,attributes,and behaviors for FLNMs to provide safe care and achieve patient outcomes under particular circumstances within a clinical context.Learning from the pandemic,most participants agreed that they needed to have additional clinical skills.These skills must be advanced to accurately access and critically think about the best options for patient care.Six core competencies were identified: 1)emergency and critical care,2) hospital disaster/crisis management,3)case management,4)infection control and prevention,5)basic clinical skills,and 6)medication management.The exemplars of participants’ quotes can be seen in Table 4.

Table 4 Dimensions of clinical core competencies and exemplar quotes.
3.3.Theme 3: technological core competencies
Technological core competencies refer to the skill sets of FLNMs in understanding,using,and developing technology.Understandably,the daily management and clinical tasks the FLNMs perform rely on different tools and processes.In other words,technology is a mediating and essential variable in nursing management and practice;thus,enhancing technological skills is a necessity.The participants’ quotes can be viewed in Table 5.
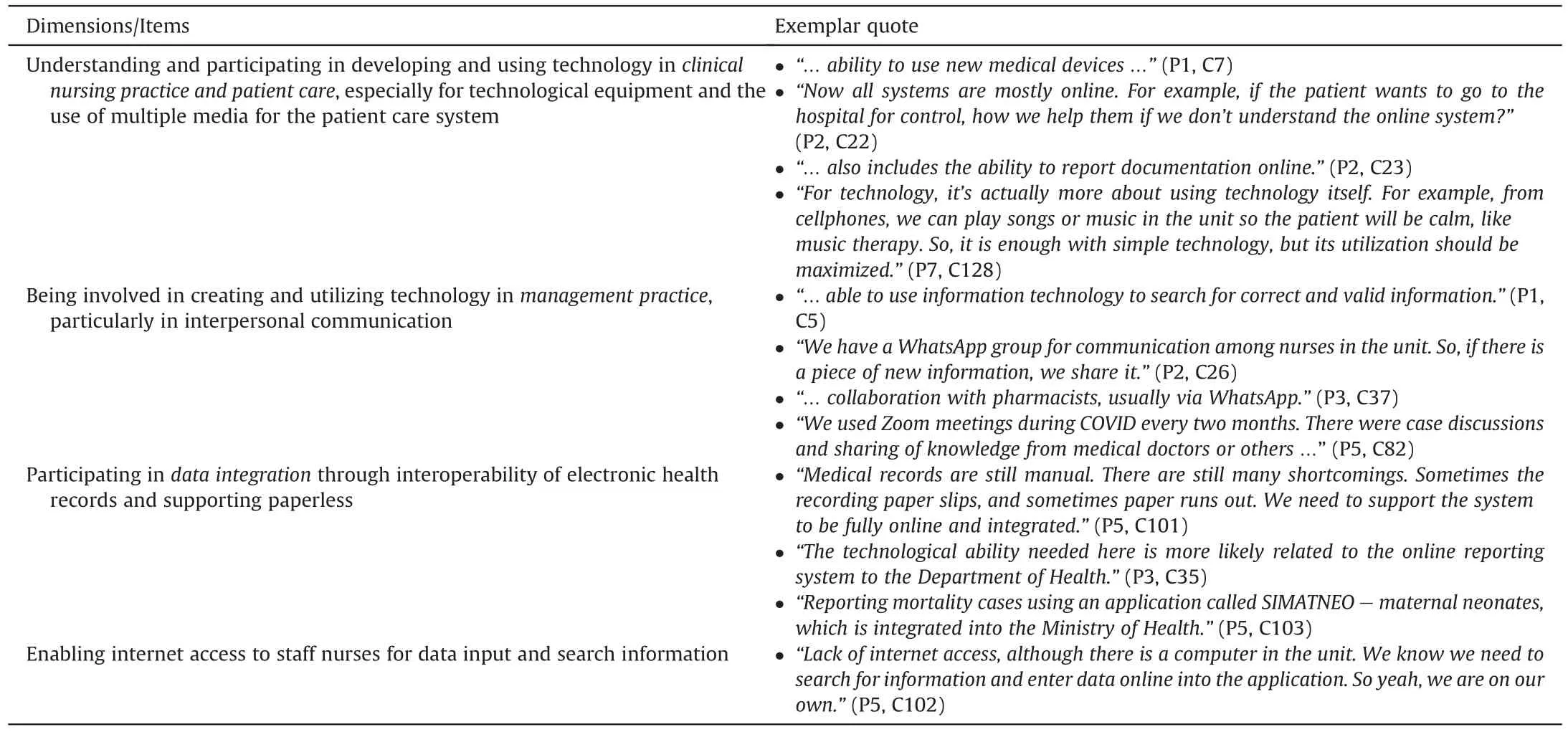
Table 5 Dimensions of technological core competencies and exemplar quotes.
3.4.Theme 4: personal traits
Learning from the pandemic,personal traits are needed to deal with complex environments and emergencies.Personality traits refer to FLNMs’ characteristic patterns of thoughts,feelings,and behaviors.These include being brave,fast,patient,optimistic,consistent,and responsible.These personal traits must be included in the managerial or leadership competencies,but we havedifferentiated between managerial core competencies and personality traits for clarity.The participants’ quotes are displayed in Table 6.
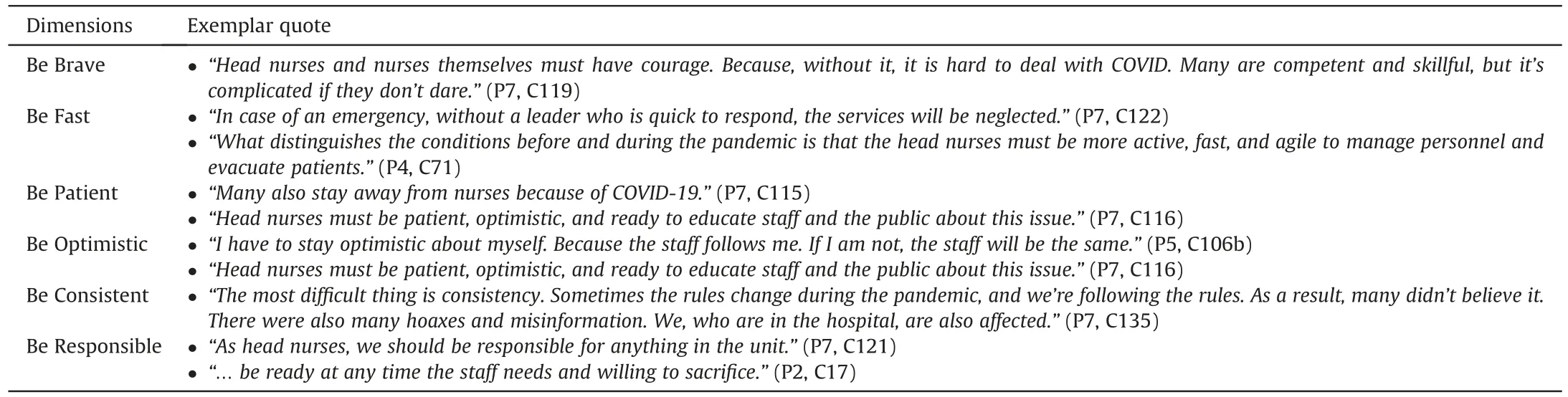
Table 6 Dimensions of personality traits and exemplar quotes.
4.Discussion
The study findings provided additional insights into the core competencies of FLNMs.The authors are aware that the main themes may not be novel,but the new dimensions may help refine the lists of FLNMs’ core competencies for the new normal.
4.1.Managerial core competencies
Out of the seven subthemes of the managerial core competencies,we highlight the dimensions that might be different from the existing research: 1) FLNMs should be able to establish their own reward system within their unit using their allocated budget as hospital incentives for nurses are often delayed,missed,or insufficiently implemented.However,incentives are essential for recognizing nurses’ efforts and supporting their wellness [5];2)FLNMs should be prepared to provide training for their staff(training of trainers),particularly during emergencies when finding external trainers becomes challenging [8];3) The study highlights the importance of FLNMs seeking performance assessment from middle and top nurse managers.Often,the focus is predominantly on evaluating staff nurses,making this aspect overlooked;4)FLNMs must prioritize self-care and embrace a healthy lifestyle,a factor often disregarded but emphasized in prior research [22];5)FLNMs play a central role in care coordination and collaboration to improve patient outcomes,particularly in situations involving overlapping responsibilities between nurses and other professions[23];6)FLNMs require the scientific ability to assess and apply the evidence-based practice,staying update to address misleading information accessed by patients and families online [24];7) FLNMs should serve as role models,employing adaptable leadership styles and political skills.This competency is considered universal as they must lead,empower,and solve conflict [24].However,leadership education is necessary for FLNMs[25];8)FLNMS are responsible for maintaining records,conducting inventory,and communicating supplies and equipment.Although this is traditionally an equipment manager’s role but identified in our study;9) FLNMS are encouraged to be more involved in the hospital budget process,even though they lack direct decision-making authority regarding financial matters in their units consistent with prior research[26].However,finance is considered one of the most-cited core competencies required by nurse managers [12].
4.2.Clinical core competencies
This study highlights the significant emphasis placed on clinical core competencies as managerial core competencies among FLNMs.The essential competencies include emergency skills,critical care,case management,infection control,and prevention.The rationale behind incorporating these core competencies is that FLNMs often provide direct patient care during nursing staff shortages.Furthermore,these core competencies are crucial for training and coaching nurses within the unit.
Hospital disaster or crisis management is an imperative skill set for FLNMs to enhance preparedness,as corroborated by prior research studies [5,9].Additionally,lessons from the pandemic emphasize the need for a comprehensive preparedness plan to respond to future disasters effectively.However,successful disaster management requires a multidisciplinary approach [27] and emphasizes the importance of interpersonal communication competence among FLNMs [8].
4.3.Technological core competencies
The technological core competencies can be seen as a mediated factor in delivering the roles and functions in management and clinical practice.The participants emphasized using WhatsApp for communication and Zoom meetings for virtual collaboration.These findings highlight the importance of FLNMs’ understanding and proficiency in utilizing these tools to support their work.This aligns with a previous study [30] that stated that technologies,such as instant messaging,document sharing,video conferencing,social media,and other technologies,mediated performance and social influence in healthcare settings.Additionally,integrating hospital data through electronic health records interoperability is crucial for enhancing care quality [31].
4.4.Personality traits
Personality traits are a subset of socio-emotional skills that seem to explain why people in leadership positions act the way they do[32].This study identified six personality traits for FLNMs:bravery,speed,patience,optimism,consistency,and responsibility.First,FLNMs must be brave in critical situations,prioritizing principles and fostering a safer environment.They inspire and enable others through professional behaviors and values [33].Second,FLNMs must possess speed,respond quickly,be proactive,and execute tasks efficiently.Referred to as“speed leadership,”this emphasizes completing tasks within a limited timeframe and delivering optimal results[34].Third,patience is essential,particularly in the face of challenges and societal issues related to the pandemic.Fourth,optimism is vital,enabling FLNMs to navigate challenges,find opportunities,and persevere in nursing practice.While not everyone may naturally possess optimism,it can be nurtured and developed [35].Fifth,consistency plays a critical role in FLNMs’work,providing clear and consistent messages to foster trust and stability among staff [36].Finally,responsibility emerges as a vital trait for FLNMs for managing and evaluating staff performance,teaching,coaching,empowering their team[37],and being present and creating a support network [5].
4.5.Implications of the study
First,the identified core competencies can serve as a valuable guideline for updating FLNMs’ core competencies,allowing organizations to align their management training programs accordingly.Second,the findings can contribute to developing an objective tool for assessing FLNMs’ core competencies.Third,the identified core competencies highlight areas for hospitals to provide training programs,including leadership,disaster/crisis management,medication management,technology,and professional/personal development,to equip FLNMs with the necessary tools for success.Fourth,implementing performance assessments designed for FLNMs is recommended to ensure and maintain quality in their roles.Fifth,hospital managers are encouraged to involve FLNMs in financial management for their respective units,enabling them to contribute expertise,promote ownership and accountability,and make informed resource allocation and budgeting decisions.
4.6.Limitations of the study and recommendations for future research
The study findings were limited to a single hospital setting,which may not represent all FLNMs in Indonesia.Further research is needed to validate the core competencies across multiple hospitals or healthcare settings.Future studies should evaluate the core competencies’construct validity and psychometric properties to enhance their reliability using a larger sample of FLNMs.Comparative studies between FLNMs in different regions or countries can also provide insights into potential cultural or contextual variations in core competencies.
5.Conclusion
As the world transitions to an endemic phase of COVID-19,the recovery process is expected to be prolonged,spanning several years.New challenges will arise throughout this period,prompting the development and implementation of innovative solutions.While this study may not discover a flawless approach to identifying all fundamental skills,it does propose a novel model of core competencies,providing a starting point for FLNMs.FLNMs have self-development goals,and this new competency model offers a standard for hospital managers to select competent nurse managers.Ultimately,this has a positive impact on healthcare organizations in the new normal era.The core competencies identified in this study encompass managerial,clinical,and technological skills and personal traits,all of which are crucial for FLNMs in this evolving landscape.It is important to note that further research is necessary to validate and confirm these core competencies in future studies.
Funding
This study was supported by Second Century Fund (C2F),Chulalongkorn University,Bangkok,Thailand.Funder has no role of study design,data analysis,interpretation,and drafting the manuscript.
Data availability statement
The data generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
CRediT authorship contribution statement
Joko Gunawan:Conceptualization,Methodology,Validation,Formal analysis,Investigation,Data curation,Writing -original draft,Writing -review &editing,Project administration,Funding acquisition.Yupin Aungsuroch:Conceptualization,Methodology,Validation,Formal analysis,Investigation,Data curation,Writingoriginal draft,Writing -review &editing,Project administration,Supervision,Funding acquisition.Mary L.Fisher:Conceptualization,Methodology,Validation,Formal analysis,Data curation,Writing -review &editing,Supervision.Colleen Marzilli:Conceptualization,Methodology,Validation,Formal analysis,Data curation,Writing -review &editing.Nazliansyah:Methodology,Validation,Formal analysis,Investigation,Writing -review &editing.Ety Hastuti:Methodology,Validation,Formal analysis,Investigation,Writing-review&editing.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgements
The authors acknowledge all nurse managers in this study for participation in this study.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.08.001.
杂志排行

International Journal of Nursing Sciences的其它文章
- The associations among nurse work engagement,job satisfaction,quality of care,and intent to leave: A national survey in the United States
- 《国际护理科学(英文)》2024年征稿
- Meaning of community activity participation for older adults in couple households
- The implementation and impacts of national standards forcomprehensive care in acute care hospitals: An integrative review
- Nurse-coordinated home-based cardiac rehabilitation for patients with heart failure: A scoping review
- Effectiveness of a family-based program for post-stroke patients and families: A cluster randomized controlled trial