Acute liver failure: A systematic review and network meta-analysis of optimal type of stem cells in animal models
2023-03-15JunFengMaJianPingGaoZiWeiShao
Jun-Feng Ma, Jian-Ping Gao, Zi-Wei Shao
Jun-Feng Ma, Jian-Ping Gao, Zi-Wei Shao, Department of Surgical Oncology, Gansu Provincial Hospital, Lanzhou 730030, Gansu Province, China
Abstract BACKGROUND The therapeutic effects of various stem cells in acute liver failure (ALF) have been demonstrated in preclinical studies. However, the specific type of stem cells with the highest therapeutic potential has not been determined.AIM To validate the efficacy of stem cells in ALF model and to identify the most promising stem cells.METHODS A search was conducted on the PubMed, Web of Science, Embase, Scopus, and Cochrane databases from inception to May 3, 2022, and updated on November 16,2022 to identify relevant studies. Two independent reviewers performed the literature search, identification, screening, quality assessment, and data extraction.RESULTS A total of 89 animal studies were included in the analysis. The results of traditional meta-analysis showed that stem cell therapy could significantly reduce the serum levels of alanine aminotransferase [weighted mean difference (WMD) =-181.05 (-191.71, -170.39)], aspartate aminotransferase [WMD = -309.04 (-328.45, -289.63)], tumor necrosis factor-alpha [WMD = -8.75 (-9.93, -7.56)], and interleukin-6 [WMD = -10.43 (-12.11, -8.76)] in animal models of ALF. Further subgroup analysis and network meta-analysis showed that although mesenchymal stem cells are the current research hotspot, the effect of liver stem cells (LSCs) on improving liver function is significantly better than that of the other five types of stem cells. In addition, the ranking results showed that the possibility of LSCs improving liver function ranked first. This fully proves the great therapeutic potential of LSCs, which needs to be paid more attention in the future.CONCLUSION LSCs may have a higher therapeutic potential. Further high-quality animal experiments are needed to explore the most effective stem cells for ALF.
Key Words: Acute liver failure; Stem cells; Animal model; Systematic review; Network meta-analysis
INTRODUCTION
Acute liver failure (ALF) is a clinical syndrome in which a large number of hepatocytes undergo necrosis resulting in severe liver function damage within a short period time. This condition occurs in the absence of chronic liver disease and is associated with severe complications, such as hepatic encephalopathy and even death, with a mortality rate of about 40%-62.2%[1-3]. The etiologies of ALF include heat pain poisoning, liver ischemia, viral hepatitis and autoimmune hepatitis, as well as prescription drugs, herbs and dietary supplements[1]. Currently, patients with ALF mainly receive medical supportive treatment due to the lack of specific therapy. Although liver transplantation is the only proven treatment, it is limited by the unavailability of donor organs, high medical costs, and the need for lifelong immunosuppressive drugs. Therefore, there is a need to develop newer and more effective therapeutic strategies.
Advances in clinical application of stem cells have provided a new perspective for ALF treatment[4].Stem cells have many advantages, including self-renewal capacities, high proliferative activities, multidirectional differentiation, anti-inflammation, anti-apoptosis, and immunomodulatory activities. They can be obtained from various sources, such as the bone marrow, umbilical cord, adipose tissue, amniotic fluid and embryos among others[5,6]. After transplantation, naive stem cells or differentiated hepatocyte-like cells rapidly restore essential liver functions by replenishing functional hepatocytes and/or by stimulating endogenous liver regeneration processes through paracrine actions. Stem cell transplantation has been shown to increase the cumulative survival rate of ALF patients from 55.6% to 73.2%[7]. Stem cells improve damaged liver functions by increasing the activities of serum albumin,cholinesterase and prothrombin and reducing the levels of serum total bilirubin and alanine aminotransferase (ALT)[8].
Although the significance of stem cells in the treatment of ALF has been demonstrated in preclinical and clinical trials, there are still some controversies and obstacles that need to be resolved. For example,bone marrow mesenchymal stem cells (BMSCs) can be easily obtained without ethical problems and are considered the first-choice for autologous transplantation. However, their therapeutic effects are limited by easy aging and lack of vitality[9]. On the contrary, umbilical cord MSCs (UCMSCs) have become a new research hotspot because of their non-aging, low immunogenicity, and high proliferative activities[10]. Adipose MSCs (ADMSCs) can be prepared by minimally invasive methods, grow fasterin vitro,and secrete abundant cytokines as well as growth factors related to immune regulation. Dysregulation of ADMSCs in clinical applications is significantly lower than that of embryonic stem cells (ESCs) or induced pluripotent stem cells (IPSCs)[11,12]. Therefore, ADMSCs are good candidates for ALF treatment. The non-invasive stem cell population, menstrual blood-derived stem cells (MenSCs), has been recently studied[13-15]. It has been postulated that MenSCs can express markers for both MSCs and ESCs, and can differentiate into the three germ layers. Fathi-Kazerooniet al[16] found that compared with BMSCs, MenSCs significantly reduced serum ALT and aspartate aminotransferase(AST) levels in ALF mice models. Therefore, the therapeutic potential of MenSCs cannot be ignored.
In conclusion, stem cells can improve liver failure. However, it is not clear which kind of stem cells has the best therapeutic effect. Solving this problem will improve the therapeutic effect and accelerate the clinical translation of stem cells. To date, few studies have directly compared the therapeutic effects of different types of stem cells. In the absence of direct comparisons, systematic reviews and network meta-analyses can be used to perform direct and indirect comparisons between different interventions and estimate the ranking probabilities[17]. Therefore, we intend to compare the therapeutic potential of different types of stem cells through subgroup analysis of traditional meta-analysis and network metaanalysis. Our findings inform on optimal types of stem cells and provide a reference for animal experiments and clinical research.
MATERIALS AND METHODS
Inclusion and Exclusion Criteria
Patients and diseases (P): Animal models of ALF. Interventions (I): Stem cells. Control (C): (1) Positive control: Comparisons between different stem cells; and (2) Negative control: Blank, DMEM, PBS, saline.Outcomes (O): (1) Primary outcomes: ALT and AST levels; and (2) Secondary outcomes: Expression levels of genes or proteins of tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6). Type of studies(S): Controlled studies.
Data sources and searches
Candidate studies were identifiedviasearching PubMed, Web of Science, Embase, Scopus,Reference Citation Analysis, and Cochrane databases from their inceptions until February 3, 2022, and updated on November 16, 2022. Search terms were: “stem cell” OR “stem cells” OR “stromal cells” OR “stromal cell” OR “mesenchymal cell” OR “mesenchymal cells” OR “cell therapy” OR “cellular therapy” OR“progenitor cell” OR “progenitor cells” OR “cytotherapy” AND “liver failure” OR “hepatic failure”. The retrieval processes for each database are shown in Supplementary Table 1.
Literature screening, data extraction, and quality assessment
Two independent reviewers performed the literature search, identification, screening, quality assessment and data extraction. Literature screening was based on the inclusion and exclusion criteria,and data extraction was based the pre-established information (including basic information, outcome indicators, and key elements of quality evaluation) shown in Supplementary Table 2. Based on SYRCLE’s risk of bias tool for animal studies[18], 10 items in 6 aspects including selection bias,performance bias, detection bias, attrition bias, reporting bias, and other biases were used to evaluate the quality of included studies.
Statistical analysis
Traditional meta-analysis was performed using the Stata16.0 software. Odds ratios were used for count data, while weighted mean differences (WMD) rather than standardized mean differences (SMD) were used as effect indicators for measured data. In fact, when performing meta-analysis, WMD eliminates the influence of the absolute value on the results, so that the original weight and measure can truly reflect the experimental effect, and it is easy to understand when applied. However, SMD not only eliminates the influence of the absolute value, but also eliminates the influence of weights and measures on the results, which makes the results difficult to interpret and requires caution when interpreting the results. Therefore, it is a better practice to choose WMD in our study. Confidence intervals were also reported. Heterogeneity was analyzed by theχ2test whileI2was used to determine the degree of heterogeneity. If the findings were not statistically different, the fixed effects model was used for metaanalysis. Conversely, the source of heterogeneity was further analyzed, and the random-effects model used for meta-analysis. Reliability of the traditional meta-analysis results were determinedviasensitivity analyses.
Network meta-analysis was performed using the Winbugs1.4.3 software. The evidence network diagram of the comparisons for each treatment was drawn to show the current research status in the field. Then, a comparison-correction funnel chart was established to evaluate the possibility of publication bias and small sample effects in the included studies. The Bayesian network meta-analysis was performed using the Markov Chain Monte Carlo method, and ranking probability for each intervention calculated[19]. In addition, potential false positive factor (PSRF) was used to evaluate the convergence of the results. A PSRF value is between 1-1.05 indicated complete convergence, good model stability, and reliable analysis[20].
Traditional meta-analysis was performed by subgroups to explore the therapeutic effects of different types of stem cells. Only ADMSCs, amniotic fluid MSCs (AFMSCs), BMSCs, liver stem cells (LSCs),MenSCs, and UCMSCs were subjected to the network meta-analysis because studies using these six stem cells reported all the primary and secondary outcomes. In this case, the results of network metaanalysis based on different outcome indicators are comparable.
RESULTS
Literature search results
A total of 5436 articles were obtained from the preliminary search. After excluding repetitive articles and those that did not meet the inclusion criteria, 89 articles were finally included (Figure 1).

Figure 1 Flow diagram for study selection. A total of 5436 articles were obtained from 5 databases. After removing repetitive articles and those that did not meet the inclusion criteria by reading the title, abstract, and full text, 89 articles were finally included.
Basic information of the included studies
Among the 89 studies, there were 74 randomized controlled trials and 15 controlled studies. The animal species involved in the studies included Sprague-Dawley rats (22 studies), Wistar rats (6 studies),Albino rats (2 study), BALB/c mice (16 studies), C57BL/6 mice (29 studies), ICR mice (3 studies), NODSCID mice (2 studies), Swiss albino mice (1 study), dogs (1 study), pigs (6 studies), and F344-Fischer rats(1 study). In terms of gender, 66 studies included male animals, 10 studies included female animals while 13 studies did not report the gender of the animals. The animals weighed between 18 g-18 kg,were aged between 4 wk and 1.5 years, and the sample sizes were between 6-94. Modeling methods for ALF included partial hepatectomy (7 studies), carbon tetrachloride (25 studies), Concanavalin A (6 studies), D-galactosamine (D-GalN, 10 studies), D-GalN/lipopolysaccharide (27 studies),acetaminophen (9 studies), thioacetamide (4 studies), and ischemia-reperfusion injury (1 study). The types of stem cells that were assessed included ADMSCs (21 studies), UCMSCs (21 studies), AFMSCs (2 studies), BMSCs (39 studies), ESCs (1 study), IPSCs (2 studies), LSCs (2 studies), MenSCs (4 studies), and placental stem cells (PMSCs, 1 study). The transplantation routes for the stem cells included intraperitoneal injection (4 studies), liver parenchyma (3 studies), portal vein (6 studies), splenic vein (2 studies),tail vein (71 studies) and stent loading (3 studies). The transplantation timing for the stem cells was within 4 d after modeling, while the transplantation dose was between (1 × 105)-(1 × 108). The negative control groups were treated with normal saline (32 studies), PBS (35 studies), Blank (16 studies) and DMEM (6 studies). The basic information of the included studies is shown in Supplementary Table 2.

Table 1 League table of network meta-analysis estimations
Risk of bias assessment results
Although there were 74 randomized controlled trials among the included studies, there were no reports on specific randomized grouping methods or whether covert grouping was implemented. Eighty-one studies reported that the baseline characteristics of experimental animals, such as age, sex and weight were balanced. Stem cell transplantation before modeling was performed in 4 studies. Seventy-eight studies reported randomized placement of animals during the experiments. Due to limited information provided by the included studies, it was difficult to determine whether animal breeders and/or researchers had been blinded. Only eight studies reported randomly selecting animals in measurement of the results. Thirty-one studies had blinded outcome evaluators. There was no study that reported on the loss or follow-up of animals. Although protocols were not available for all studies, all expected results were clearly reported. Findings from the risk of bias assessment are shown in Figure 2.

Figure 2 Risk of bias assessment results. 10 items in 6 aspects including selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases were used to evaluate the quality of included studies. The risk of bias of all studies about a certain item is expressed as a percentage.
Meta-analysis results
Serum ALT levels:A total of 78 studies reported on serum ALT levels. Meta-analysis of the random effects model showed that ALT levels in the stem cell group were significantly suppressed, relative to those of the negative control group [WMD = -181.05 (-191.71, -170.39)]. Subgroup analysis revealed that the trend of improving liver functions was: IPSCs, LSCs, UCMSCs, ADMSCs, PMSCs, MenSCs, BMSCs.Notably, the treatment effects of AFMSCs and ESCs were not markedly different from those of the control group (Supplementary Figure 1). The evidence network diagram showed that BMSCs and ADMSCs are the current research hotspots (Figure 3A). Network meta-analysis revealed that the effects of LSCs in reducing ALT levels were significantly better than those of the other five stem cells (Table 1).The asymmetrical comparative correction funnel chart suggested that there was publication bias and small sample effects (Figure 4A). The ranking results showed that LSCs had the best effects in reducing ALT levels (Figure 5A).
Serum AST levels:Seventy-one studies reported serum AST levels. The meta-analysis of the random effects model showed that serum AST levels in the stem cell group were significantly lower than those of the negative control group [WMD = -309.04 (-328.45, -289.63)]. Subgroup analysis showed that the trend for effects of improving liver functions was: LSCs, IPSCs, UCMSCs, AFMSCs, ADMSCs, MenSCs,BMSCs (Supplementary Figure 2). The evidence network diagram showed that BMSCs and ADMSCs are the current research hotspots (Figure 3B). Network meta-analysis showed that the effects of LSCs in reducing AST levels were significantly better than those of the other five stem cells (Table 1). The asymmetrical comparative correction funnel chart revealed the possibility of publication bias and small sample effects (Figure 4B). The rank ranking results showed that LSCs have the best effects in reducing AST levels (Figure 5B).
Serum TNF-α levels:Twenty-six studies reported the expression of TNF-α at gene or protein levels. The meta-analysis of random effects model showed that TNF-α levels in the stem cell group were significantly suppressed, relative to those of the negative control group [WMD = -8.75 (-9.93, -7.56)].Subgroup analysis showed that the reduction trend in TNF-α levels was UCMSCs, LSCs, ADMSCs,MenSCs, BMSCs. The treatment effects of AFMSCs were not significantly different from those of the negative control group (Supplementary Figure 3). The evidence network diagram showed that BMSCs and ADMSCs are the current research hotspots (Figure 3C). Network meta-analysis showed that differences in the effects of all stem cells on reducing TNF-α levels were insignificant (Table 1). The asymmetrical comparative correction funnel chart suggested the existence of publication bias and small sample effects (Figure 4C). The rank ranking results showed that LSCs was most effective in reducing TNF-α levels (Figure 5C).

Figure 3 Evidence network diagram. Circle size represents sample size involved, thickness of the line segment represents the number of studies involving both interventions. A: Alanine aminotransferase; B: Aspartate aminotransferase; C: Tumor necrosis factor-α; D: Interleukin-6. BMSCs: Bone marrow mesenchymal stem cells; LSCs: Liver stem cells; MenSCs: Menstrual blood-derived stem cells; AFMSCs: Amniotic fluid mesenchymal stem cells; ADMSCs: Adipose mesenchymal stem cells; UCMSCs: Umbilical cord mesenchymal stem cells.

Figure 4 The comparison-correction funnel plot. The dotted lines on both sides of the funnel plot represent 95% confidence intervals, and each point represents a study. If each point falls within the dotted line and is symmetrically distributed on both sides of the vertical line, there is no publication bias. On the contrary, it indicates the possibility of publication bias. A: Alanine aminotransferase; B: Aspartate aminotransferase; C: Tumor necrosis factor-α; D: Interleukin-6.BMSCs: Bone marrow mesenchymal stem cells; LSCs: Liver stem cells; MenSCs: Menstrual blood-derived stem cells; AFMSCs: Amniotic fluid mesenchymal stem cells; ADMSCs: Adipose mesenchymal stem cells; UCMSCs: Umbilical cord mesenchymal stem cells.
Serum IL-6 levels:A total of 20 studies reported the expression of IL-6 at gene or proteins levels. A meta-analysis of the random effects model showed that that IL-6 levels in the stem cell group were significantly lower than those of the negative control group [WMD = -10.43 (-12.11, -8.76)]. Subgroup analysis showed that the trend in reduction of IL-6 was LSCs, ADMSCs, UCMSCs, BMSCs, MenSCs. The treatment effects of AFMSCs were not markedly different from those of the negative control group(Supplementary Figure 4). The evidence network diagram showed that BMSCs and ADMSCs are the current research hotspots (Figure 3D). Network meta-analysis did not reveal significant differences in the effects of all stem cells in reducing IL-6 levels (Table 1). The asymmetrical comparative correction funnel chart showed the possibility of publication bias and small sample effects (Figure 4D). The rank ranking results revealed that LSCs have the best effects in reducing IL-6 levels (Figure 5D).
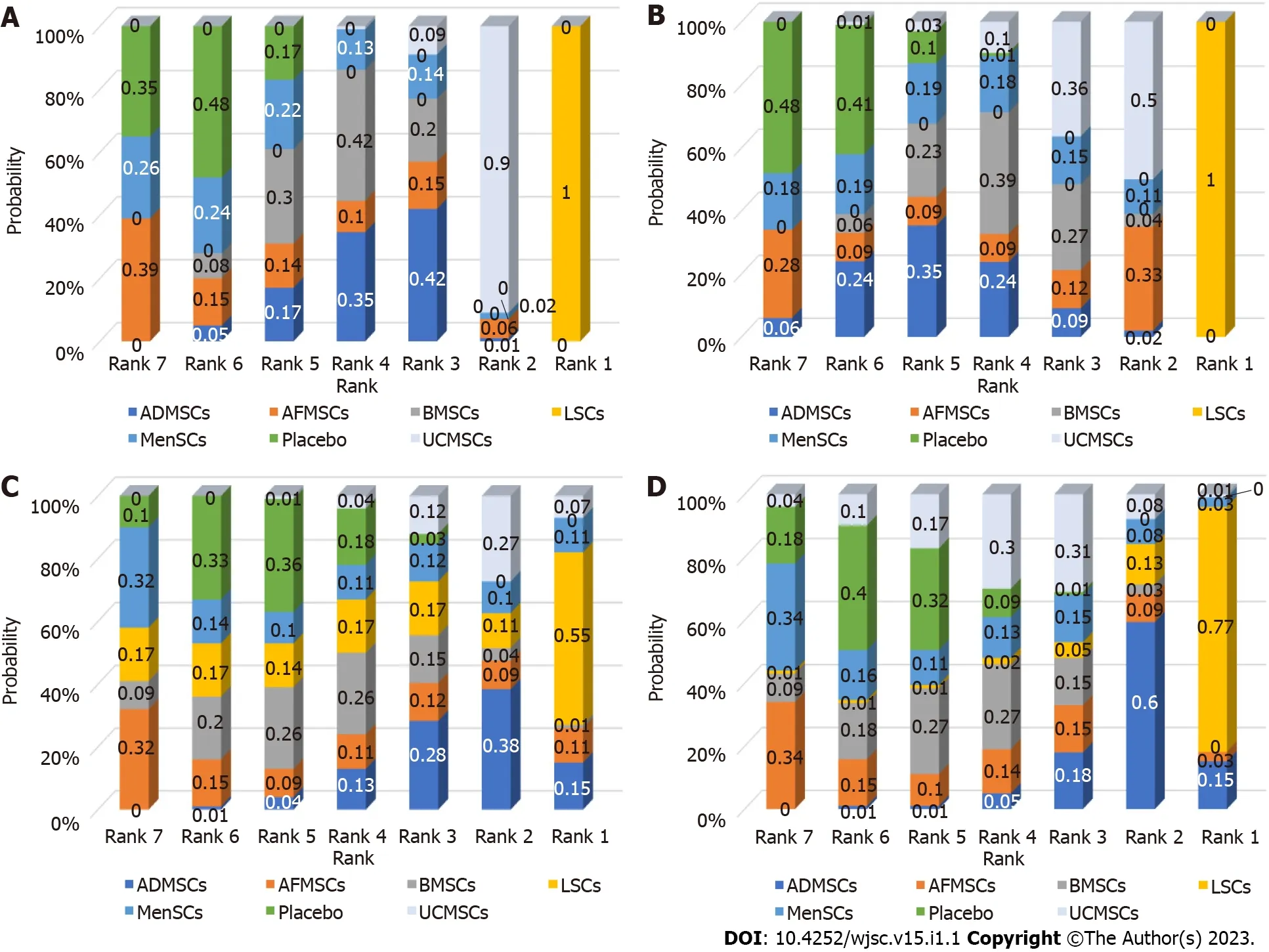
Figure 5 Ranking results. The higher the probability of being ranked first, the better the treatment effect of that intervention. A: Alanine aminotransferase; B:Aspartate aminotransferase; C: Tumor necrosis factor-α; D: Interleukin-6. BMSCs: Bone marrow mesenchymal stem cells; LSCs: Liver stem cells; MenSCs:Menstrual blood-derived stem cells; AFMSCs: Amniotic fluid mesenchymal stem cells; ADMSCs: Adipose mesenchymal stem cells; UCMSCs: Umbilical cord mesenchymal stem cells.
Reliability test of meta-analysis results:Sensitivity analysis was performed to test the reliability of the results from the traditional meta-analysis. The four outcome indicators showed that after one by one exclusion of certain studies, directions of the confidence intervals of the combined results of the remaining studies did not change, indicating that findings from the meta-analysis were robust and reliable (Figure 6).
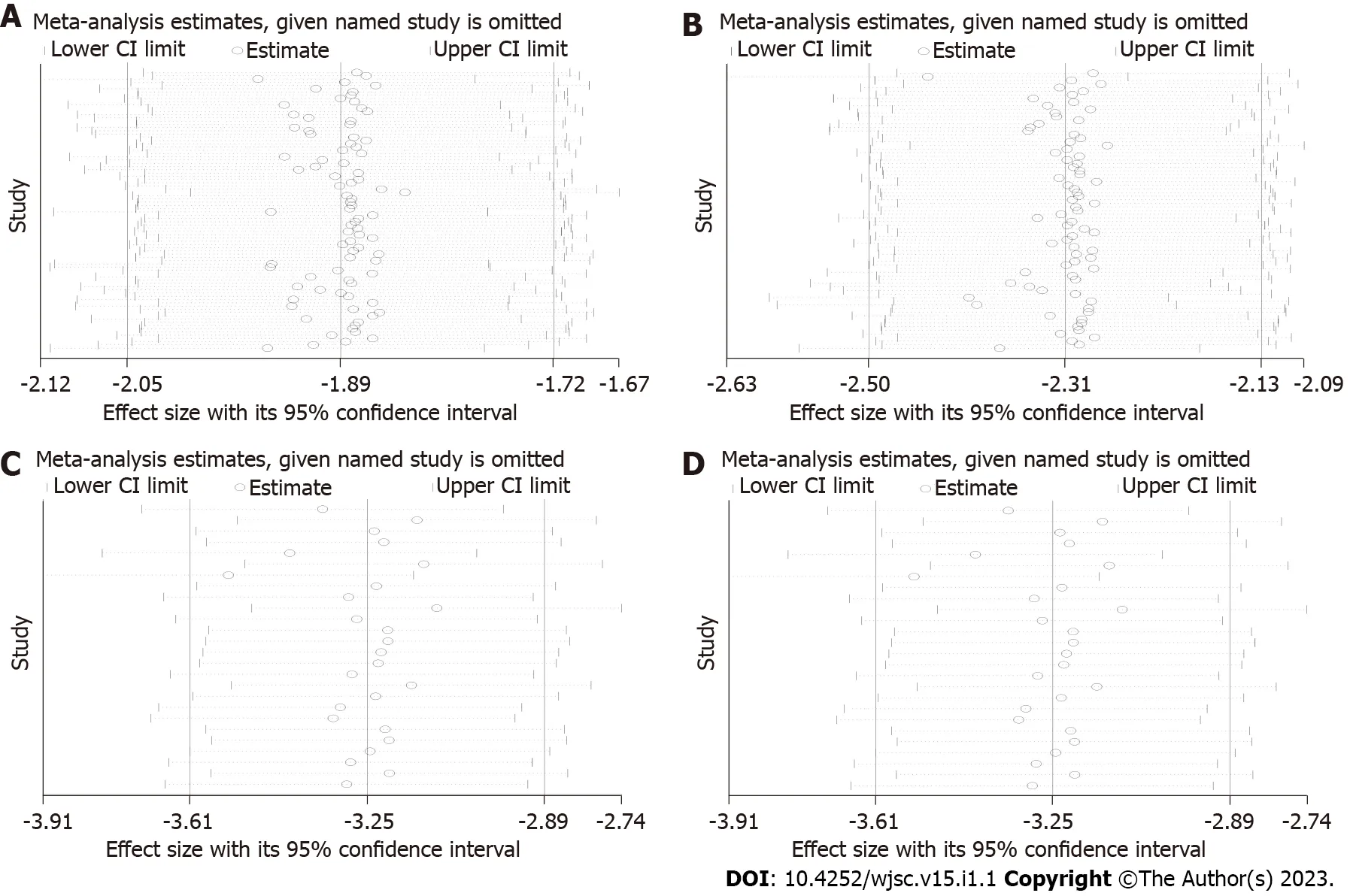
Figure 6 Results of sensitivity analysis. After excluding a certain study, the remaining studies were combined for analysis to see if there were any changes in the effect sizes. If the results of the remaining studies were basically the same as the previous total combined results (the range of the confidence interval did not change significantly), the results of the meta-analysis were considered to be reliable. Conversely, the results of the meta-analysis were considered unreliable. A:Alanine aminotransferase; B: Aspartate aminotransferase; C: Tumor necrosis factor-α; D: Interleukin-6. CI: Confidence interval.
Then, PSRF was used to evaluate the fitting effects of the model, after which the reliability of the network meta-analysis results was determined. The four outcome indicators showed that PSRF converged to 1 after a certain number of iterations, indicating that robustness and reliability of the network meta-analysis results were good (Figure 7).

Figure 7 Results of potential false positive factor. After a certain number of iterations, the curve finally approaches 1, which indicates that the results of the network meta-analysis have good robustness and reliability. A: Alanine aminotransferase; B: Aspartate aminotransferase; C: Tumor necrosis factor-α; D: Interleukin-6. PSRF: Potential false positive factor.
DISCUSSION
The mechanism for occurrence of ALF begins with hepatocyte necrosis[21], followed by damage to the membrane structure of hepatocytes and the release of AST and glutamic pyruvic transaminase (ALT)from hepatocytes into the bloodstream. Therefore, the serum levels of AST and ALT are the most reliable markers of liver injury[22]. Stem cells can protect the damaged liver by promoting hepatocyte regeneration and inhibiting hepatocyte apoptosis[23]. Consistent with findings from current animal studies, our meta-analysis showed that different types of stem cell transplantation can significantly suppress serum ALT and AST levels. This indicates the great therapeutic potential of stem cells in ALF.By confirming that stem cells can improve liver functions, there is a need to elucidate on their therapeutic potential to accelerate their clinical translation. About 10 different types of stem cells have been studied in ALF, however, a limited number of studies have compared the therapeutic effects of different types of stem cells. We found that only four studies compared the therapeutic potentials of different types of stem cells in ALF. Among them, three studies compared ADMSCs with BMSCs. They showed that the effects of the two kinds of stem cells on improving liver functions were comparable[24-26]. In another study, MenSCs were found to be significantly better than BMSCs in reducing ALT and AST levels[16]. Studies have reported that MSCs have the advantages of easy access, multipotential,anti-apoptosis, immunosuppression, and paracrine characteristics[27]. Therefore, MSCs are the most studied stem cells in the field of ALF. This is consistent with results shown in the evidence map of our network meta-analysis, that is, MSCs derived from the bone marrow, fat and umbilical cord are the current research focus. However, further subgroup analysis and network meta-analysis showed that they are not the best in improving liver functions. Besides, LSCs are more effective in reducing serum ALT and AST levels. LSCs are MSC-like cells in the liver. In addition to having the same surface markers as MSCs, such as CD29, CD73, CD44, CD105 and CD146, they also express specific hepatocyte markers (albumin, cytokeratin8, and cytokeratin-18) and embryonic markers (Nanog, Oct3/4, Sox2,Musashi, SSEA4, and Pax2)[28,29]. Studies have shown that LSCs improve liver functions by directly differentiating into hepatocytes and secreting cytokines that inhibit injury progression[29]. A possible reason why LSCs showed a better ability to repair liver functions is their greater ability to migrate to the damaged liver. For example, after intravenous transplantation, LSCs preferentially aggregate and play a role in the damaged liver, while MSCs are mainly trapped in the lungs and do not migrate to the damaged liver[29,30]. In addition, human LSCs do not express human leukocyte antigen II molecules and costimulatory molecules (CD40, CD80 and CD86), which reduces the severity of immune responses[31].
The most common causes of death in ALF patients is systemic complications with release of proinflammatory cytokines and impairment of associated molecular patterns of the necrotic hepatocytes, endothelial cells, and leukocytes[32,33]. Regardless of the cause, uncontrolled inflammation is crucial in ALF occurrence and development[34]. Reduction of pro-inflammatory cytokines and hepatocyte dysfunction is key in ALF treatment. Hepatocyte apoptosis is associated with excess activations of immune responses, usually mediated by TNF-α and IL-6[35]. TNF-α is a pro-inflammatory factor that regulates the expressions of pro-inflammatory genes, tissue factors and leukocyte antigen class I[36,37]. The TNF-α interacts with its receptor (TNF receptor I) to activate signal transduction pathways[38]. IL-6 is produced by Th2 cells, monocytes, and vascular endothelial cells, and is one of the core cytokines involved in liver injury development[39]. Excess secretion of IL-6 delays cell cycle progression and inhibits hepatocyte regeneration[40]. Therefore, plasma levels of TNF-α and IL-6 in ALF patients were significantly increased. Although previous studies have confirmed that MSCs from human cord blood can differentiate into hepatocyte-like cellsin vivoand partially repair Dgalactose/lipopolysaccharide-induced liver injury in mice models[41]. Menstrual fluid-derived stem cells showed the potential to restore liver functions in mice that had been subjected to 2/3 partial hepatectomy, and menstrual stem cell-derived hepatocyte-like cells were detected in the recipient liver[42]. However, transplanted stem cells are less likely to differentiate into functional hepatocytes and regenerate liver tissues within a short period of time. In early stages, stem cells protect against ALFviaexerting their immunomodulatory and anti-inflammatory properties[43]. Consistent with the results of animal experiments, our meta-analysis found that stem cell transplantation significantly reduces TNF-α and IL-6 levels. In addition, consistent with ALT and AST levels, LSCs are the most potential stem cells for reducing serum TNF-α and IL-6 levels. The consistent results from four different outcome indicators prove that LSCs have the greatest therapeutic potential in ALF treatment. Our results are also in line with current research evidence, which has confirmed that serum IL-6 levels are positively correlated with ALT and AST levels. However, studies on LSCs are few, and the mechanisms by which they exert their repair effects have yet to be conclusively determined. There is also a lack of evidence for direct comparisons of LSCs with other stem cell types. Therefore, studies should elucidate on the roles of LSCs. In addition, due to differences in outcome reporting, AFMSCs, ESCs, and IPSCs were not analyzed in our network meta-analysis. This does not mean that other types of stem cells have limited therapeutic potential. On the contrary, studies should also focus on therapeutic effects of different types of stem cells, carefully compare their advantages and disadvantages, and construct stem cells with more potential through genetic modification and other means.
Evidence quality
Considerable heterogeneity among the included studies:The included studies involved 11 different animal species, 8 modeling methods, and there were wide variations in baseline characteristics of animals, such as body weight and age. In addition, there were differences in stem cell types,transplantation doses and routes, as well as in measurement and reporting of outcome indicators (such as protein levels, gene levels,etc.), resulting in greater heterogeneity among the included studies, which reduced the reliability of meta-analysis results. There is a need to standardize ALF animal models,experimental implementation and outcome measurements to improve the authenticity of experimental results and the reliability of systematic review results.
Insufficient internal authenticity of animal experiments:(1) Selection bias: Randomization and covert grouping of animals while ensuring the balance of their baseline characteristics is an important measure to avoid selection bias[18]. Although about 90% of the studies were randomized controlled trials and the baseline characteristics of the animals were balanced, no study reported the specific randomization method and whether they implemented concealed grouping, resulting in a certain selection bias; (2)Performance bias: Placement of animals, such as different light and temperature conditions, has an important impact on experimental results[18]. Although 87.64% of the studies randomized the placement of animals, no study had blinded animal breeders and researchers, resulting in a certain implementation bias; (3) Detection bias: Failure to blind the outcome assessors in animal experiments may lead to exaggeration of effects and produce false positive results[44,45]. Only 34.83% of the studies reported blinding the outcome assessors, and no study reported a specific blinding process. Therefore,studies should pay more attention to applications of blinding in experimental designs, and should provide more experimental details to improve the reporting quality; (4) Reporting bias: Selective reporting of results can lead to publication bias, which affects the reliability of experimental results[46].Moreover, protocols were not available for all studies. Therefore, we suggest that animal experimental researchers prospectively register protocols to improve transparency; and (5) Publication bias: Negative results from animal experiments are difficult to publish[47]. If negative results are not included in systematic reviews, the effects of intervention will be overestimated. The corrected funnel chart revealed a certain publication bias in this field.
Limited external authenticity of included studies:External authenticity in animal experiments refers to reproducibility of results and feasibility of their translation to clinical research[48]. The lack of external authenticity in this study is reflected in the following aspects: (1) Although this study has preliminarily determined the best type of stem cells, the routes, dose, and timing of stem cell transplantation are also key factors for achieving desirable outcomes[49,50]. Until these experimental conditions are clearly explored, clinical translation of stem cells will remain immature; (2) In animal experiments, stem cells are often transplanted in early stages. However, clinical practice must be to recruit patients a few days or weeks after ALF; (3) Clinically, factors such as medical histories and physical conditions of patients may affect the efficacies of stem cells. For example, aging and diabetes can lead to impaired stem cell proliferation, decreased angiogenesis, and reduced wound healing. Animal experiments are difficult to simulate[51]; (4) The clinically used stem cells are all human stem cells, but in animal experiments, stem cells are obtained from various sources, which may lead to strong immune responses, affecting the authenticity of animal experimental results[50]; and (5) Stem cells have a potential risk of developing tumors because of their multi-directional differentiation ability, but no research has focused on the potential side effects of stem cells[49]. Therefore, studies should pay attention to effectiveness and safety of stem cell therapy.
Strengths and limitations
Strengths of this study: (1) As the first study in the ALF field, we systematically evaluated and analyzed the effects of different types of stem cells by subgroups, and pointed out the challenges and directions for improvement; (2) After testing the robustness and reliability of the results of traditional metaanalysis and network meta-analysis, we found that our results are very reliable; (3) In the absence of evidence for direct comparisons, the therapeutic potential of different stem cells was comprehensively compared through subgroup analyses of traditional meta-analyses and network meta-analyses; and (4)Based on the SYRCLE bias risk assessment tool, the internal authenticity of animal experiments was evaluated. At the same time, external authenticity was also evaluated.
Limitations of this study: (1) Due to the small number of studies and the large differences in treatment strategies of stem cells in different studies, subgroup analysis of transplantation doses and route of stem cell administration were not performed; (2) Searches were only performed in English databases, which may have led to a certain linguistic bias; and (3) Failure to search grey literature and conference abstracts may have led to a publication bias.
CONCLUSION
This analysis showed that stem cell therapy can significantly reduce ALT, AST, TNF-α and IL-6 levels in ALF animal models through a comprehensive analysis of 89 studies. Importantly, although MSCs are the current research hotspot, we found that LSCs have superior therapeutic effects in ALF. However,because of the low quality of evidence from internal and external authenticity of animal studies, future high-quality animal studies should aim at identifying the best stem cells for therapeutic purposes.
ARTICLE HIGHLIGHTS
Research background
The therapeutic effects of various stem cells in acute liver failure (ALF) have been demonstrated in preclinical studies, however, it has not been determined which stem cells have the best therapeutic implications.
Research motivation
The efficacy of stem cells in ALF has been demonstrated in preclinical and clinical trials. However, it remains unclear which stem cells have the most therapeutic potential. Addressing this issue is critical to improve the efficacy of stem cells and to accelerate the progress of basic and clinical research of stem cells.
Research objectives
To explore the best type of stem cells for ALF treatment and to promote the clinical translation of stem cell therapy.
Research methods
A systematic review and meta-analysis of stem cell therapy for ALF. A search was conducted on the PubMed, Web of Science, Embase, Scopus, and Cochrane databases. Two independent reviewers performed the literature search, identification, screening, quality assessment, and data extraction. The data was analyzed by STATA 16 and Winbugs1.4.3 software.
Research results
Stem cell therapy can significantly reduce serum levels of alanine aminotransferase, aspartate aminotransferase, tumor necrosis factor-alpha, and interleukin-6 in animals with ALF. Although mesenchymal stem cells are the current research focus, among the six types of stem cells included in the analysis, liver stem cells (LSCs) have the greatest therapeutic potential.
Research conclusions
LSCs have the best effects in treating ALF.
Research perspectives
In ALF treatment, stem cell therapy, especially LSCs should be paid more attention to. In addition, to improve on the quality of research, future animal studies should be carefully designed and reported.
FOOTNOTES
Author contributions:Ma JF undertook the design, guidance and writing of the paper; Gao JP and Shao ZW completed the literature retrieval, information extraction and data analysis.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
PRISMA 2009 Checklist statement:The authors have read the PRISMA 2009 Checklist, and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Jun-Feng Ma 0000-0002-6472-9031.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Wang JJ
