Application of 3D-printed prosthesis in revision surgery with large inflammatory pseudotumour and extensive bone defect: A case report
2023-01-04HongPingWangMingYouWangYuPingLanZhuoDongTangQiFengTaoChunYuChen
Hong-Ping Wang, Ming-You Wang, Yu-Ping Lan, Zhuo-Dong Tang, Qi-Feng Tao, Chun-Yu Chen
Hong-Ping Wang, Yu-Ping Lan, Zhuo-Dong Tang, Qi-Feng Tao, Chun-Yu Chen, Department of Orthopaedics, Panzhihua Municipal Central Hospital, Panzhihua 617000, Sichuan Province,China
Ming-You Wang, Department of Clinical Medicine, Dali University, Dali 671000, Yunnan Province, China
Abstract BACKGROUND Hip revision surgery is the final treatment option for the failure of artificial hip joints, but it is more difficult than the initial operation. For patients with hip joint loosening around the prosthesis combined with large inflammatory pseudotumours and large segment bone defects, hip revision is even more difficult, and clinical reports are rare.CASE SUMMARY Male, 59 years old. The patient underwent left hip replacement 35 years ago and was now admitted to hospital due to massive masses in the left thigh, shortening of the left lower extremity, and pain and lameness of the left hip joint. X-ray, computed tomography and magnetic resonance imaging revealed prosthesis loosening, left acetabular bone defect (Parprosky IIIB type), and a bone defect of the left proximal femur (Parprosky IIIA type). Inflammatory pseudotumours were seen in the left hip and left thigh. Hip revision surgery was performed using a 3Dprinted custom acetabular prosthesis was used for hip revision surgery, which was produced by Arcam Electron Beam Melting system with Electron Beam Melting technology. The operation was successful, and the patient was followed up regularly after the operation. The custom-made acetabular prosthesis was well matched, the inflammatory pseudotumour was completely removed, the postoperative hip prosthesis was stable, and the old greater trochanter fracture was well reduced and fixed. The patient was partially weight-bearing with crutches 3 mo after the operation and walked with full weight-bearing after 6 mo. The hip prosthesis was stable, and there was no recurrence of inflammatory pseudotumours at the last follow-up. The Visual Analogue Scale was 3, and the Harris hip score was 90.CONCLUSION The use of 3D-printed personalized custom prostheses for complex hip revision surgery has satisfactory surgical results and has great clinical application value.
Key Words: 3D printing; Inflammatory pseudotumour; Electron Beam Melting technology; Hip revision;Bone defect; Case report
INTRODUCTION
Prosthesis loosening is one of the main reasons for revision surgery, and the appearance of an inflammatory pseudotumor, especially one with accompanying symptoms, is another[1]. Inflammatory pseudotumor parenchyma is a granulomatous or destructive cystic lesion, also known as a pseudotumor, metal metaplasia or sterile lymphocyte-dominated vasculitis[2], which has adverse reactions to metal fragments[3,4]. It is neither an infection nor a tumor and is prone to occur around total prostheses of the hip, with a tumor-like shape and varying sizes[5]. It can cause progressive pain, swelling, joint subluxation, compression, periprosthetic fractures and soft tissue destruction in the affected extremity[2,6]. Hip revision surgery is the final treatment option for prosthesis failure and for patients with periprosthetic loosening of the hip joint combined with a large inflammatory pseudotumor, extensive bone defects and nonunion of the greater trochanter. However, such surgery is rare in clinical practice and extremely difficult to perform. At present, with the continuous progress of science and technology and the continuous improvement of medicine, the application of 3D printing technology in orthopedics has gradually expanded from initial bone tumor patients to other patients with complex bone diseases, especially those with large bone defects. Due to the continuously improving cooperation between medicine and industry, the accurate 3D printing of materials is gradually being applied. The individualized materials for repair and reconstruction are prepared according to the characteristics of patients' bone defects and combined with 3D printing technology, which can meet the complex needs of patients for bone defect repair and achieve personalized and precise treatment of diseases. Therefore, the treatment of complex diseases is simplified. The successful application of 3D printing technology in the case study presented here fully demonstrates the advantages of this technology and may serve as a reference for its future clinical application. Here, we implanted a 3D-printed personalized acetabular prosthesis, and the long-term follow-up results were satisfactory.
This case report was approved by the Ethics Committee of Panzhihua Central Hospital, and written informed consent was obtained from the patient and his family.
CASE PRESENTATION
Chief complaints
Eight months ago, the patient developed left thigh swelling without obvious reasons, and the swelling gradually extended from the back to the front, accompanied by pain when moving the leg.
History of present illness
Underwent herniorrhaphy 40+ years ago in the local hospital without other diseases or operations. Unfortunately, an intertrochanteric fracture of the left femur was caused by a fall 40 years ago and was treated conservatively, with the presence of ununited fractures later. The patient underwent left hip replacement 35 years ago due to a left intertrochanteric fracture combined with left femoral head necrosis. Eight months ago, the patient developed left thigh swelling without obvious reasons, and the swelling gradually extended from the back to the front, accompanied by pain when moving the leg. The claudication of the left lower limb was aggravated, so he was admitted to our department.
History of past illness
Underwent herniorrhaphy 40+ years ago in the local hospital without other diseases or operations. Unfortunately, an intertrochanteric fracture of the left femur was caused by a fall 40 years ago and was treated conservatively, with the presence of ununited fractures later. The patient underwent left hip replacement 35 years ago due to a left intertrochanteric fracture combined with left femoral head necrosis.
Personal and family history
The patient was born in the original place, without industrial poisons, radioactive substances, dust exposure history, no contact history with epidemic water in epidemic areas, smoking history of 40+years, with an average of 20 cigarettes/day, and denied drinking history. Divorce, having a child, healthy family. Deny the history of family hereditary diseases and infectious diseases.
Physical examination
The left lower limb was shortened by approximately 8 cm compared with the right side. A 15-cm-long surgical scar was seen on the left hip, where there was no redness, swelling or exudation. The middle and upper parts of the left thigh were obviously swollen, there were palpable fluctuations, the local skin temperature was normal, and there was no obvious tenderness (Figure 1).
Imaging examinations
X-ray: Left superior pubic branch - irregular pubic comb bone. Computed tomography (CT): Partial bone absorption of the upper part of the left femur; bone destruction of the left acetabulum; swelling and unclear layers of soft tissue shadows in the upper part of the left thigh and around the hip joint; multiple cystic lesions in the upper part of the left thigh, with multiple cystic necrosis areas in the lesions, of which the posterior subcutaneous necrosis area is a long strip from the subcutaneous buttock to the lower back. Magnetic resonance imaging (MRI): The left upper femur and left hip joint have abnormal bone, with multiple necrosis sites around the hip joint and soft tissue of the left thigh as the main cystic disease. Considering the inflammatory disease, the size of the larger cystic lesion is approximately 8.7 cm × 9.3 cm × 18 cm (Figure 2).
FINAL DIAGNOSIS
Prosthesis loosening after left hip replacement; Inflammatory pseudotumor of left thigh; Old fracture of left greater trochanter of femur; Shortening deformity of left lower limb.
TREATMENT
CT examination of the patient's hip joint was performed after admission. The 1:1-sized hip joint model was printed through 3D printing technology (supported by Akcome Medical Co., Ltd.), which we used for preoperative planning and disease communication. Revision surgery is routinely performed to reconstruct acetabular side bone defects, but it is extremely difficult and costly. After fully explaining the scenario to the patient and his family members, the personalized 3D-printed custom acetabular prosthesis was used for hip revision surgery, which was produced by the Arcam EBM system with electron beam melting technology (Figure 3).

Figure 1 Preoperative swelling of both lower extremities and the left thigh. A: The unequal appearance of the lower limbs; B and C: The inflammatory pseudotumor of the left thigh.
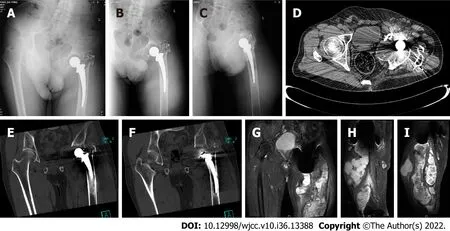
Figure 2 Preoperative imaging examination. A: X-ray; A-C: Left superior pubic branch - irregular pubic comb bone; D: CT; D-F: Partial bone absorption of the upper part of the left femur; bone destruction of the left acetabulum; swelling and unclear layers of soft tissue shadows in the upper part of the left thigh and around the hip joint; multiple cystic lesions in the upper part of the left thigh, with multiple cystic necrosis areas in the lesions, of which the posterior subcutaneous necrosis area is a long strip from the subcutaneous buttock to the lower back; G: MRI; G-I: The left upper femur and left hip joint have abnormal bone, with multiple necrosis sites around the hip joint and soft tissue of the left thigh as the main cystic disease. Considering the inflammatory disease, the size of the larger cystic lesion is approximately 8.7cm × 9.3 cm × 18 cm.
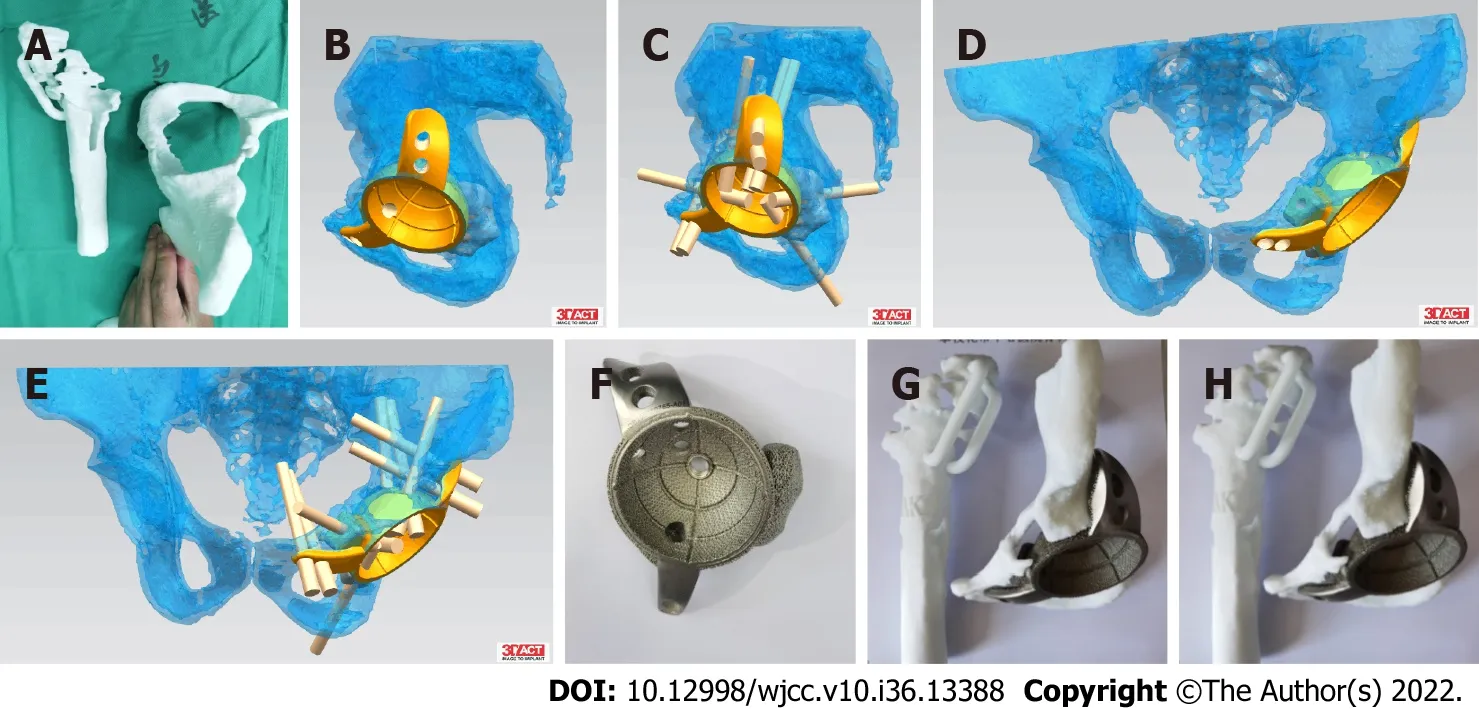
Figure 3 Design process of personalized prosthesis. A: 1:1 printed model; B-E: Preoperative planning; F: Cup making; G-H: Preoperative surgery simulation.
Operation method
Under general anesthesia, the skin, subcutaneous tissue and scar were incised layer by layer through the posterolateral incision of the left hip, the hip joint was released, and the large inflammatory pseudotumor around the hip joint and thigh was removed. The artificial prosthesis was removed, rinsed with a large amount of normal saline and soaked with iodophor solution. Allograft cancellous bone was implanted into the bone defect of the posterior wall of the acetabulum and pressed tightly. The abduction angle was kept at 45° after the acetabulum was worn down, and the customized 3D-printed Accurate Constructive Technology acetabular prosthesis was installed with an anterior tilt of 20°. The inner lining was installed, the appropriate femoral stem and femoral head were selected and implanted, and the hip joint was reset. The hip joint in all directions was relatively stable, and the tightness was appropriate. The fractured greater trochanter was reduced and fixed with a trochanteric plate after satisfactory reduction. C-arm fluoroscopy showed that the prosthesis was in a good position (Figure 4). Complete hemostasis was performed, and an indwelling drainage tube was placed after repeated rinsing. A peripheral nerve block cocktail was given, tranexamic acid was perfused intraarticularly, and the incision was sutured.
OUTCOME AND FOLLOW-UP
We strove for a fast recovery in the perioperative period. Postoperatively, to prevent thrombosis, cefuroxime sodium was given for anti-inflammation and rivaroxaban was given for anticoagulation. Postoperative bacterial culture was negative, and the pathology showed a small amount of neutrophil and lymphocyte infiltration and no obvious tumor cells. X-ray imaging showed the following: The swelling of the thigh had subsided, the acetabular prosthesis was stable, the greater trochanter fracture was well reduced and fixed, the femoral stem and the greater trochanter were stably held in place, the fixation was effective, and the hip joint position was satisfactory. The patient was kept to strict bed rest after surgery, hip joint activities were performed on the 2ndday after surgery, and the drainage tube was removed on the 3rdday. The patient underwent debridement due to poor incision healing 3 wk after the operation. During the operation, it was found that the residual inflammatory pseudotumor recurred, but the wound recovered well after the residual inflammatory pseudotumor was completely removed. The patient regularly returned to the hospital for follow-up at 1.5 mo, 3 mo, and 6 mo. Partial weightbearing with crutches was started 3 mo after the operation, and full weight-bearing was started at 6 mo. During the follow-up period, the wound healing was good, the greater trochanter plate and the hip prosthesis were well positioned, and no obvious osteolytic changes or inflammatory tumor recurrence were found around the prosthesis (Figure 5). There was no obvious pain or discomfort in the hip at the last follow-up, the Visual Analogue Scale was 3 points, and the Harris hip joint score was 90 points.
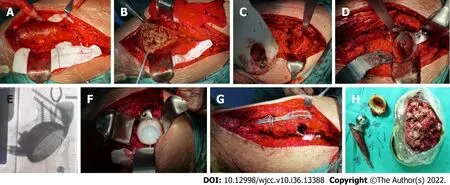
Figure 4 Surgical steps. A: The inflammatory pseudotumor was freed; B: The pseudotumor was excised; C. Acetabular defect; D. Implanted acetabular cup; E.Intraoperative fluoroscopy; F. Uchimura implant; G. Steel plate-fixed rotor; H. Removal of prosthesis and inflammatory pseudotumor.
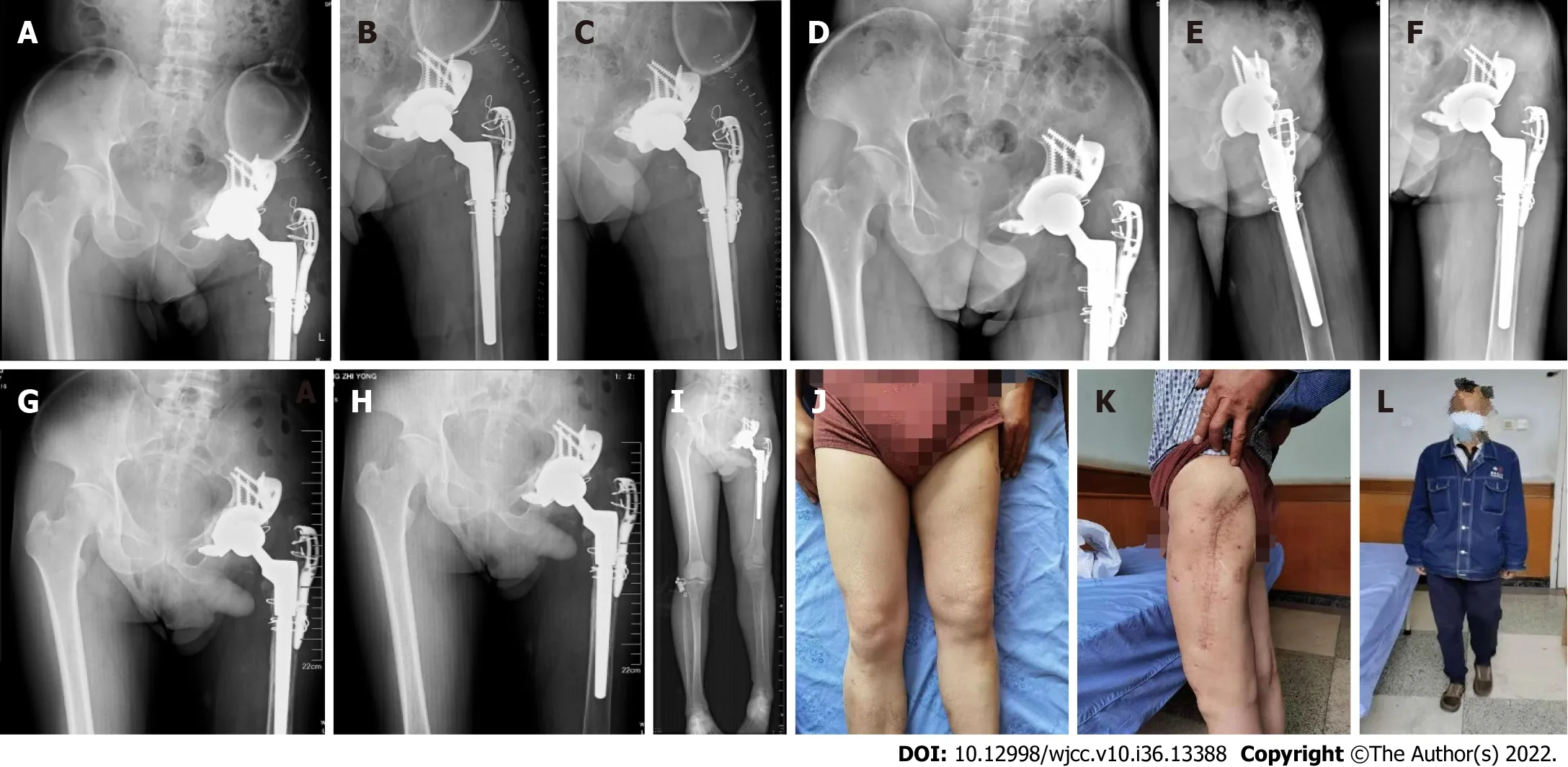
Figure 5 Postoperative follow-up. A: X-ray in two days after surgery; B and C: Different view; D-F: Ninety days after surgery; G-L: Six months after surgery (a 30-cm surgical scar on the outside of the left thigh, without redness, swelling or exudation).
DISCUSSION
3D printing technology, which is a kind of additive manufacturing, emerged in 1984. It is based on the principle of discrete/accumulation of different 2D cross-sectional shapes. It is a new additive manufacturing technique that builds up materials layer by layer into 3D shapes based on digital models[7]. In recent years, with the development of 3D printing techniques in the medical industry and based on patient CT and MRI image data, reverse molding has been performed to achieve 3D model reconstruction of patient tissues and organs and medical implants, which helps optimize the surgical plan and procedure. Medical planning and surgical implementation methods have become very fastgrowing innovations in clinical medicine[8,9]. At present, the application of 3D printing technology in the hip joint can be divided into four categories: (1) Establishment of an anatomical model based on patient images to promote a better understanding of the corresponding anatomy, and at the same time, to facilitate the simulations of surgery and improve the controllability of surgery in each sex; (2) Establishment of patient-specific instruments to improve surgical accuracy[10]; (3) Customizing and producing artificial joint replacement implants; and (4) Customizing the specific implanted prosthesis according to the patient's condition to increase the degree of matching with the specific anatomy of the patient[11,12,15]. How to preserve more bone mass in hip revision surgery is the key to the success of the surgery, especially for revision surgery with large bone defects. Preserving bone mass helps to achieve early full weight-bearing postoperatively, to retain as much range of joint movement as possible, and to maintain long-term prosthesis stabilization[13].
This patient had previously undergone left hip arthroplasty due to intertrochanteric fracture combined with left femoral head necrosis. During the operation, a cement prosthesis (stem and acetabulum) was used, and the intertrochanteric fracture was fixed with wire bundles after reduction. At the time of admission, the patient's left upper thigh was swollen, a local large mass bulged, and the left hip joint was painful when moving, but there were no chills, fever, skin sinus formation or exudation at the local site. White blood cells and inflammatory indicators were normal. No bacteria were found with arthrocentesis. X-ray, CT and MRI examinations showed osteolysis around the prosthesis, bone defects of the left acetabulum and proximal femur, and multiple cystic lesions in the soft tissue of the middle and upper left thigh. It was also found that the femoral trochanteric fixation wire was broken and the fracture was displaced again. The clinical manifestations of this patient are consistent with the diagnosis of an inflammatory pseudotumor, so it is highly likely that it was an inflammatory pseudotumor. According to related reports, the incidence of inflammatory pseudotumor is 40%-60% at the metal-metal interface and 20% at the metal-polyethylene interface. They are less common at ceramic-polyethylene and ceramic-ceramic interfaces[14,15], which is related to the low wear rate and the biological inertness of ceramics. Due to the long medical history of this patient, the friction between the metal femoral head and polyethylene, the micromovement of the bone cement and the bone surface, and the loosened wire continued to produce grinding. Metal ions in the synovial fluid produced by corrosion lead to the formation of inflammatory pseudotumor[14,16-18] and progressively create large defects in the femur and acetabulum.
For this patient, we made a 3D-printed 1:1-sized hip joint model. Along with the difficulty of the imaging examination, the difficulty of the operation was mainly due to the following: (1) The acetabular bone defect was very large, and it was difficult to reconstruct the acetabulum; (2) The inflammatory pseudotumor had spread far, so it was difficult to completely remove it; (3) The greater trochanter of the femur had an old fracture that had not healed, and it was difficult to effectively reduce and fix the greater trochanter; (4) The proximal femoral bone defect made it difficult to maintain the effective fixation of the greater trochanter; and (5) The patient's lower limbs were not equal in length, and it was difficult to restore their length. Based on the above difficulties, we used 3D printing to create a personalized prosthesis. The acetabular cup was fixed on the ilium and pubis by screws. It was stable and ensured effective bone ingrowth later on. A high-molecular-weight polyethylene inner village and ceramic femoral head were used to reduce the recurrence rate of inflammatory pseudotumor induced by metal ions and prolong the service life of the prosthesis. The advantages of this scheme are as follows: (1) It fully preserved the patient’s acetabular bone mass and greatly increased the contact area of the acetabular prosthesis; (2) The 3D printing module was used to repeatedly perform surgical simulation and refine the surgical plan before surgery; and (3) The design of the integrated 3D-printed prosthesis was more conducive to performing the operation and saved operation time. The greater trochanter needs to be effectively fixed to ensure the normal function of the abductor muscles, and it is also important to the future stability of the hip joint. The greater trochanter provides conditions for late healing. There is controversy over whether the inflammatory pseudotumor needs to be completely removed. According to a study, in the natural history of an inflammatory pseudotumor without intervention, 60% of the lesions will increase in volume but can be reduced or regressed in 80% of patients undergoing hip revision surgery. Sassoonet al[4] reported on 5 patients who underwent revision surgery; the inflammatory pseudotumor was partially removed in 2 patients and retained in 3 patients, and the pseudotumor was significantly reduced or regressed in all patients at the 17-mo follow-up. Therefore, in the initial operation, we focused mostly on pseudotumor with large cystic cavities that were associated with the joint and did not give special treatment to the relatively closed and hidden pseudotumor. However, the wound returned due to the recurrence of inflammatory pseudotumor in the early postoperative period. Second-stage surgery was performed for complete debridement. This shows that large inflammatory pseudotumor need to be completely removed during the operation to avoid the adverse effects of repeated inflammatory pseudotumor.
CONCLUSION
We report a case of complex hip joint loosening around a prosthesis combined with a large inflammatory pseudotumor, extensive bone defect and an old fracture of the greater trochanter. A 3D-printed personalized prosthesis for artificial hip revision can be effectively installed. Preoperative planning and successful completion of the complex hip revision surgery yielded good results. This case provides a reference for the surgical treatment of similar diseases.
FOOTNOTES
Author contributions:Wang HP and Wang MY participated in the perioperative management, surgical process, and postoperative follow-up and wrote the main manuscript; Lan YP was in charge of the whole preoperative planning, operation scheme design and operation process and helped draft the manuscript and revise the article; Tao QF, Tang ZD and Chen CY were in charge of the follow-up of the patients and the collection and collation of the patients' pictures; All authors read and approved the final draft.
Informed consent statement:Written informed consent was obtained from the patient for the publication of this case report.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Yu-Ping Lan 0000-0001-8058-9414.
S-Editor:Liu GL
L-Editor:A
P-Editor:Liu GL
杂志排行

World Journal of Clinical Cases的其它文章
- Liver injury in COVID-19: Holds ferritinophagy-mediated ferroptosis accountable
- Amebic liver abscess by Entamoeba histolytica
- Living with liver disease in the era of COVID-19-the impact of the epidemic and the threat to high-risk populations
- Cortical bone trajectory screws in the treatment of lumbar degenerative disc disease in patients with osteoporosis
- Probiotics for preventing gestational diabetes in overweight or obese pregnant women: A review
- Effectiveness of microwave endometrial ablation combined with hysteroscopic transcervical resection in treating submucous uterine myomas