Global prevalence, mortality, and main risk factors for COVID-19 associated pneumocystosis: A systematic review and meta-analysis
2022-12-28HosseinKhodadadiEhsanAhmadpourSanamNamiRasoulMohammadiHaniehHosseiniMahsaBehravanHamidMorovati
Hossein Khodadadi, Ehsan Ahmadpour, Sanam Nami, Rasoul Mohammadi, Hanieh Hosseini, Mahsa Behravan, Hamid Morovati
1Department of Parasitology and Mycology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran
2Drug Applied Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
3Department of Medical Mycology and Parasitology, School of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
4Department of Medical Parasitology and Mycology, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran
5Immunology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
6Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran
ABSTRACT
KEYWORDS: Coronavirus disease 19; COVID-19; SARS-CoV-2;Pneumocystis pneumonia (PcP); COVID-associated infections;Prevalence; Odds ratio; Risk factors
1. Introduction
Coronavirus disease 2019 (COVID-19) is an infection caused by the severe acute respiratory syndrome coronavirus-2 (SARSCoV-2). Since its emergence in December 2019, many other infections have been associated with this virus[1]. Fungal infections,alongside bacterial and other viral infections, occur as coinfections in COVID-19 patients[2,3]. Although aspergillosis, mucormycosis,and candidiasis are well-known COVID-19-associated fungal infections[4,5], coinfection with other opportunistic fungi, such as Pneumocystis (P.) jirovecii has also been found in COVID-19 patients[6]. P. jirovecii (formerly known as P. carinii) is an opportunistic fungal pathogen that can cause severe pneumonia in immunocompromised hosts[7]. It is more challenging to distinguish between SARS-CoV-2 and pneumocystis pneumonia (PcP)among COVID-19-associated pneumocystosis (CAP) patients due to the overall similarity of their clinical and radiological manifestations[8-13].
Although pneumocystis DNA has been detected in the air of hospital rooms, bronchoscopy suites, and clinics, no definite proof has supported this view that it has environmental reservoirs[7,14]. It is transmitted through the airborne transmission route from person to person[7,14]. However, a study indicated that up to one in five people might have pneumocystis DNA in their bronchoalveolar lavage fluid[15]. These findings suggest the reactivation of latent infection or de-novo person-to-person transmission, particularly during outbreaks[16]. Therefore, the presence of cysts in the lung may be asymptomatic (in immunocompetent patients) or lead to infection(especially in high-risk patients)[16,17].There are four major categories of susceptible hosts: (1) congenital with inborn immunodeficiencies in T- or B-cell profiles; (2)patients with immunosuppressive therapy or chemotherapy,especially corticosteroids; (3) HIV-positive patients who acquired other opportunistic pathogens; and (4) neonates and infants with malnutrition[7,14,18]. Prior respiratory viral infections, such as Cytomegalovirus (CMV) infection, and pre-existing lung diseases,such as chronic obstructive pulmonary diseases, may increase the incidence of PcP in these populations[19]. Since HIV is the most prevalent risk factor for PcP, T cells play a critical role in controlling the infection[20,21]. PcP can occur in patients with compromised innate immunity due to corticosteroids, CMV infection, or the lack of humoral or cellular immunity[22-24]. However, it has been detected in several groups of non-HIV immunocompromised hosts,e.g., hematopoietic malignancies (25%), organ transplant recipients(22.4%), and inflammatory disorders (12.9%). About 90.5% of these patients have been administered corticosteroids[7,14,22-24].

Figure 1. The flowchart of study identification and selection process.
Diagnosis of PcP is based on four principles: radiographic patterns,laboratory parameters, microbiological evaluation, and molecular investigation[7,14,25-30]. There is no pathognomonic radiographic pattern for pneumocystis infection[7,14]. The radiographic pattern is determined by any underlying conditions, immunosuppression level, and infection stage. Thus, several overlapping COVID-19 radiological patterns pose a major challenge to diagnosis[10,11,13].Trimethoprim-sulfamethoxazole is the first line of PcP control and management and the chief prophylactic agent for prevention.
Concerns about outbreaks of nosocomial infections during the COVID-19 era are becoming a world-wild problem because this may change these infection patterns. With this perspective, and due to diagnostic overlaps between the COVID-19 pandemic and PcP in target people, we designed this analysis to provide accurate statistics on this superinfection. The results of our analysis will be suitable for researchers worldwide to develop preventative policies for infection control.
2. Materials and methods
2.1. Search strategy and selection criteria
The protocol is registered at PROSPERO (Register ID:CRD42022337867). The present study is conducted and reported according to PRISMA 2020 guideline[31]. We developed a broad search strategy to identify studies that reported CAP (Supplementary Table 1). In our systematic review, the search terms “Coronavirus disease”, “COVID-19”, “SARS-CoV-2 infection”, “Pneumocystis”,“Pneumocystis jirovecii”, “Coinfection”, and related terms and words for relevant studies published in PubMed, Web of Science, Scopus,Google Scholar, LitCovid, and ProQuest between December 2019 and May 2022 were used (Figure 1). No linguistic or geographical limits were applied. We hand-searched bibliographies of all recovered articles for potentially eligible studies and contacted corresponding authors for published or unpublished data if needed.December 2019 was chosen as the cut-off because it was the initiation date of the COVID-19 infection. Inclusion criteria were as follows: patients with SARS-CoV-2 and pneumocystis infection,all types of studies encompassing data about patients with SARSCoV-2 and pneumocystis infected simultaneously, including clinical trials, retrospective, prospective, and cohort studies, gray literature including conference reports, etc. Exclusion criteria were as follows:patients with SARS-CoV-2 and without pneumocystis pneumonia or patients who have other fungal infections than pneumocystis, all review-type studies (e.g., narrative, critical, systematic, and metaanalysis, and mini-reviews) case reports and case series, all studies including letters to the editor, and editorials, without patient data.Titles and abstracts of references were screened, and the full texts of potentially relevant articles were independently assessed using a standardized score sheet. Studies assessing a clearly defined population of CAP in any clinical setting were included if they had specific diagnostic criteria for PcP. These were predefined using clinical case definitions (based on CDC criteria) or confirmation with laboratory testing using molecular assays, such as PCR,sequencing, and matrix-assisted laser desorption-ionization time of flight mass spectrometry (MALDI-TOF MS)[9-12].
2.2. Data extraction
The authors independently extracted data and compared it for consistency after data extraction. Discussion and consensus resolved disagreements on final inclusions. The key variable was the proportion of PcP coinfection among COVID-19 patients. Our denominator was the population of patients with positive realtime PCR test results for the SARS-CoV-2 virus. Prevalence was defined as the number of PcP cases among patients with established SARS-CoV-2 who were inpatients in a hospital or clinic captured by included studies. The following information was captured where available: underlying risk factors, PcP treatment options (if available), site of isolation of pneumocystis (if available), age and sex of the target population, methods of pneumocystis diagnosis,body mass index, radiological findings, laboratory parameters (e.g.,levels of PO2, serum LDH, lymph count) (if available), the status of immunosuppression and HIV, intubation, and the health status of patients (death or survival).
2.3. Risk of bias (quality) assessment
This research involved studies concerning a minimum of three participants to minimize the small-study effect. Authors independently assessed the quality according to the Hoy et al.checklist previously described[32,33]. This checklist explored the various dimensions of empirical proof and methodological assumptions. If required, a consensus was voted by other coauthors to settle the disputes between the investigators. Moreover, the regression-based Egger, Begg’s-Mazumdar, and Harbord tests for small-study effects will apply to analyze publication bias for our search.
2.4. Data analysis
Meta-analysis was performed according to the DerSimonian and Laird method applying the random-effects model in caseof considerable heterogeneity, defined asI2>75%. We evaluated heterogeneity using the Chi-square (χ2-based Q statistic, significant for P<0.05) and theI2statistic. StatsDirect software version 2.7.9(StatsDirect Ltd, Wirral-UK) was used to perform calculations and the meta-analysis[34]. Odds ratio (OR) analysis was performed for related data if their case(s) and control(s) details were available.Point estimates and 95% confidence intervals (CI) were derived using prevalence data from included studies for all outcomes. Where standard errors (SE) were not provided, we incorporated confidence intervals into the formula, SE=(upper limit-lower limit)/3.92.Subgroup analysis and meta-regression were used to determine the source of heterogeneity based on certain putative moderator factors,and sensitivity analysis was used to assess the reliability of our pooling results.searches in the databases and removal of duplicate and irrelevant records (Figure 1). The results of risk of bias assessment were added to Table 1. In this analysis, 923 patients were hospitalized with SARS-CoV-2, and PcP was found in 92 patients. One study each was conducted in India[35] and Russia[36], and the remaining six studies were conducted in France[37-42]. Respiratory tract samples were targeted for the detection of PcP among COVID-19 patients.Conventional and real-time PCR methods targeting mithochondrial small and large subunits (mtSSU and mtLSU) alongside β-D-glucan were the main PcP diagnostic methods. Moreover, microscopical and fast-track diagnostic (FTD) methods were applied in two studies[35,41]. Furthermore, five studies reported the ICU stay duration of the patients (3-61 days)[35,37-40].

Table 1. Demographic data of the patients.

Table 2. Detailed results of the prevalence and OR tests of meta-analysis.

Table 3. Comparison of the epidemiological factors that affect PcP between the pre-COVID and COVID eras.
3.1. The pooled prevalence of CAP
3. Results
Our meta-analysis included eight eligible studies (Table 1) after

Figure 2. Forest plot (A) and funnel plot (B) of the pooled prevalence of coronavirus-associated pneumocystosis.
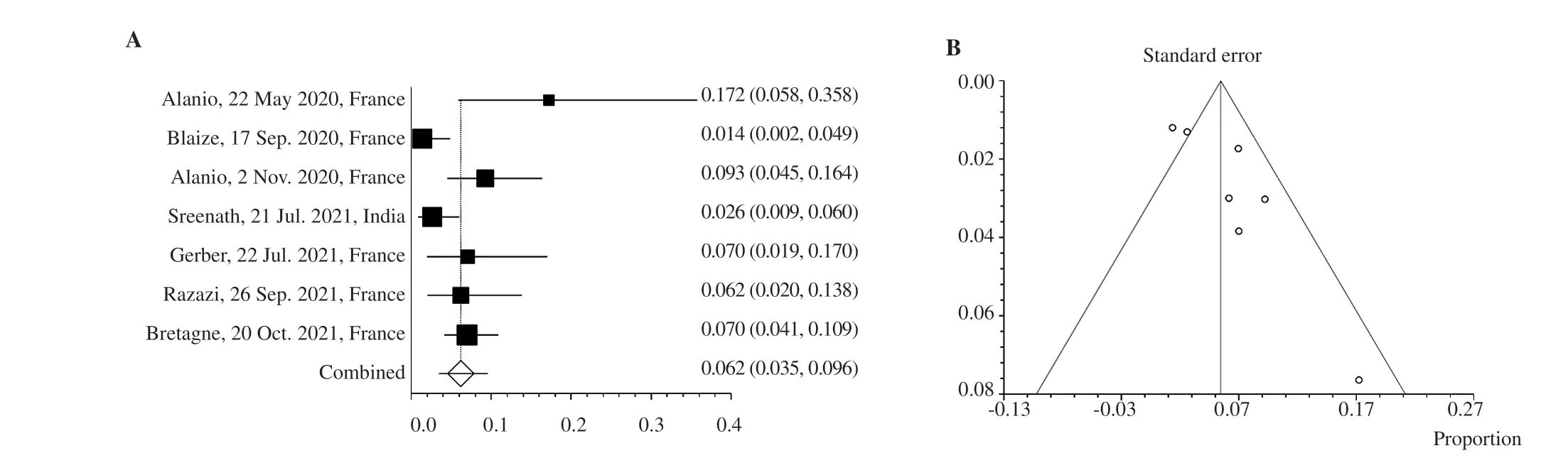
Figure 3. Forest plot (A) and funnel plot (B) of the pooled prevalence of coronavirus-associated pneumocystosis without Borodulina et al.’s study.
The percent rates of CAP cases (by country) in eight eligible studies were as follows: India 2.6% (5/191), Russia 64.7% (44/68),and France 6.5% (43/664) (Tables 1 and 2). Our random-effects model showed that the overall pooled prevalence of CAP was 11.5%(95% CI 3.8-22.7;I2=95.1%) (Table 2; Figures 2A and 2B). Also,we performed an analysis without the study by Borodulina et al.to control the effect of high heterogeneity, which resulted a 6.2%prevalence (95% CI 3.4-9.6) rate with a lower heterogeneity rate(69.3%) (Table 2; Figures 3A and 3B). As shown by funnel plots in Figures 2B and 3B and Table 2, there is a negligible publication bias between studies (intercept: 5.45; 95% CI 0.327-10.537; P=0.040 5).The analysis details of pooled prevalence were presented in Supplementary Tables 2 and 3.
3.2. OR analysis for mortality among CAP patients
Three from eight eligible studies (161 from 281 patients) reported case & control data about mortality. The results of our OR analysis indicated that non-PcP patients had 1.928 times higher mortality rates than CAP patients. Therefore, death events among CAP patients were fewer than non-PcP patients (OR 1.928; 95% CI 0.863-4.305;I2=0.00%; χ2=2.56; P=0.109) (Table 2, Supplementary Figure 1).
3.3. OR analysis for CAP patient’s sex
The results of OR analysis for data captured from five studies indicated that among COVID-19 patients, women have 1.36 times more chance of catching PcP (OR 1.357; 95% CI 0.612-3.009;I2=0.00%; χ2=0.566; P=0.452) (Table 2, Supplementary Figure 2).
3.4. OR analyses for nine underlying conditions among CAP patients
The results of OR analyses indicated that COVID patients who have acute respiratory distress syndrome (ARDS), kidney diseases (KD),pulmonary diseases (PD), and long-term corticosteroid therapy(LTC) backgrounds are 1.22, 1.26, 1.46, and 28.22 times more prone to PcP (ORARDS1.22; 95% CI 0.051-29.281; χ2=0.015; P=0.901.ORKD1.26; 95% CI 0.212-7.494; χ2=0.064; P=0.8.ORPD1.46; 95%CI 0.432-4.976;I2=0.00%; χ2=0.378; P=0.538.ORLTC28.22; 95%CI 0.538-1 480.838; χ2=2.733; P=0.098) (Table 2, Supplementary Figures 3 to 6). Also, patients who have one of diabetes mellitus(DM), hypertension (HTN), obesity, transplantation, and malignancy backgrounds are 1.17, 1.47, 1.29, 1.44, and 2.92 times less prone to PcP (ORDM1.169; 95% CI 0.409-3.334;I2=12.1%; χ2=0.085;P=0.77.ORHTN1.474; 95% CI 0.378-5.742;I2=39.9%;I2=0.312;P=0.576.ORobesity1.293; 95% CI 0.365-4.576; χ2=0.159; P=0.689.ORransplantation1.444; 95% CI 0.167-12.529; χ2=0.112; P=0.737.ORmalignancy2.924; 95% CI 0.324-26.378; χ2=0.914; P=0.34) (Table 2,Supplementary Figures 7 to 11).
4. Discussion
PcP is a life-threatening opportunistic fungal infection. Since T-cell immunodepression is usually considered the main risk factor for PcP[43], less attention has been paid to PcP in nonimmunocompromised ICU patients. However, it accounts for 7% of the co-infections with influenza patients[44]. Recently, COVID-19 patients may develop lymphocytopenia and acute respiratory distress syndrome (ARDS), requiring adjunctive steroids and/or immunomodulatory therapies, well-known susceptibility factors for developing PcP[44]. The concomitant occurrence of opportunistic fungal infections alongside the COVID-19 super-infection leads to uncontrollable situations[12,45,46]. These coinfections are needed to be more considered among health systems to reduce mortality rates and treatment costs[12,45,46].
Our meta-analysis included eight eligible studies[35-42], including 923 patients hospitalized with COVID-19. Ninety-two of them were reported as PcP cases. Here we found the pooled prevalence of 6.2%to 11.5% for CAP patients. Also, our results showed that mortality among CAP patients was 1.928 times fewer than non-CAP patients;therefore, the mortality of PcP was reduced during the COVID-19 era. We concluded that women with COVID-19 were 1.36 times more susceptible to PcP than men with COVID-19. Our findings show that ARDS (OR 1.22; 95% CI 0.051-29.281), KD (OR 1.26;95% CI 0.212-7.494), PD (OR 1.46; 95% CI 0.432-4.976), and LTC (OR 28.22; 95% CI 0.538-1 480.838) elevated the risk of PcP among COVID-19 patients. While, COVID-19 patients with DM(OR 1.169; 95% CI 0.409-3.334), HTN (OR 1.474; 95% CI 0.378-5.742), obesity (OR 1.293; 95% CI 0.365-4.576), transplantation(OR 1.444; 95% CI 0.167-2.529), and malignancy (OR 2.924; 95%CI 0.324-26.378) were less prone to PcP. During the analysis of the pooled prevalence (11.5%), we faced a high level of heterogeneity(95.1%) between included studies. As we didn’t apply any subgroup analysis or other methods to reduce the effect of high heterogeneity,we excluded the study by Borodulina et al.[36] and finally reached an acceptable heterogeneity (69.3%) with the prevalence rate of 6.2%.There is a sufficient volume of data about the prevalence of PcP during the pre-COVID era. However, there are several descriptive studies among them[47-50]; we selected five systematic reviews and meta-analyses (SR&MA) related to the pre-COVID era[46,51-55] and three SR&MA during the COVID-19 era about PcP in non-COVID patients[24,56,57] for comparison of their key findings with data of PcP among COVID-19 patients (present study) (Table 3). The pooled prevalence of PcP during the pre-COVID era ranged from 4.79% in the study of Sonego et al.[51] to 22.4% in the study of Wasserman et al.[53]. During the COVID-19 era prevalence of PcP among HIVinfected non-COVID patients ranged from 9% to 19% in the study of Wills et al.[57]. Compared to our findings, we resulted that the prevalence of PcP was not changed between pre-and post-COVID eras (Table 3). But this rate was higher in non-COVID-19 patients compared to COVID-19 patients.
During the COVID-19 epidemic, Wang et al.[24] resulted that sex was not a risk factor for mortality among non-COVID PcP patients(Table 3). However, our findings show that among COVID-19 patients, women were 1.357 times more susceptible to PcP than men.During the pre-COVID era, Wasserman et al.[53] reported a 6.5%mortality rate for PcP. Fujikura et al.[54] indicated that adjunctive corticosteroid therapy increased the mortality rate of PcP patients with an OR of 1.26. Our findings show that mortality decreased among CAP patients with an OR of 1.928 (Table 3). Compared to our findings, we concluded that PcP-related mortality was reduced by the emergence of the COVID-19 pandemic. Although misdiagnosis of PcP among COVID-19 patients can be a reason for the reduction in CAP patients’ mortality rate, interactions between immune responses in this population may lead to this reduction.
The immune response against SARS-CoV-2 is an unbridled process usually accompanied by uncontrolled inflammation and cytokine storm or cytokine release syndrome. Following the activity of cytokine release syndrome, the profile of cytokines such as TNF,which are not antigen-specific, increases and triggers an immune response against all antigens present in the microbial environment of the disease, especially in the lung. Considering that the nature of this response is systemic, it can affect the type of immune response to other infectious agents. The reduction in CAP patients’ mortality rate seems to be due to this strong and efficient innate immune response that prevents the rapid course of superinfection. Previous studies have shown the antigenic similarity between SARS-CoV-2 and other viruses, e.g., influenza, increases the immune response in co-infected patients. As we saw at the beginning of the COVID pandemic,the people who received the B.C.G vaccine were more resistant to COVID infection and its complications. The acquired immune response is supplied with memory, and the innate immune response is supplied with training. It has been shown that innate immunity training increases memory efficiency in acquired immunity, which seems to reduce mortality in CAP patients[58,59].
Sonego et al.[51] reported that underlying diseases among PcP patients were 4.76% during the pre-COVID era. Yiannakis et al.[52] showed that solid organ transplantation and primarily renal transplantation were the main risk factors for PcP outbreaks.Hosseini-Moghaddam et al.[55] indicated that CMV (OR 3.3; 95%CI 2.07-5.26) and allograft rejection (OR 2.36; CI 95% 1.54-3.62)increased the risk of PcP during the pre-COVID era. Wang et al.[24]reported that PD (OR 3.42; 95% CI 1.96-5.96), solid tumors (OR 2.06; 95% CI 1.32-3.21), lung disease (OR 3.59; 95% CI 1.91-6.75),pneumothorax (OR 2.55; 95% CI 1.13-5.77), and ventilation during hospitalization (OR 29.24; 95% CI 13.09-65.33) were the main risk factors for PcP among non-COVID patients during the COVID era.Also, Permpalung et al.[56] indicated that acute rejection [pooled odds ratio (pOR)] 2.35; 95% CI 1.69-3.26), CMV-related illnesses(pOR 3.14; 95% CI 2.30-4.29), lymphocyte count <500 cells/mm3(pOR 6.29; 95% CI 3.56-11.13), BK polyomavirus-related diseases(pOR 2.59; 95% CI 1.22-5.49), HLA mismatch 3 (pOR 1.83; 95%CI 1.06-3.17), Rituximab use (pOR 3.03; 95% CI: 1.82-5.04), and Polyclonal antibodies use for rejection (pOR 3.92; 95% CI 1.87-8.19) were the main risk factor for PcP among non-COVID patients(Table 3). We resulted that ARDS (OR 1.22; 95% CI 0.051-29.281),KD (OR 1.26; 95% CI 0.212-7.494), PD (OR 1.46; 95% CI 0.432-4.976), and LTC (OR 28.22; 95% CI 0.538-1 480.838) increased the risk of PcP among COVID-19 patients. This suggests that ARDS,PD, and LTC remained the major risk factors for PcP during the pre-and post-COVID eras. Although, we previously reported that HTN, DM, and obesity were the leading risk factors for COVID-19-associated Candida auris infections[60]. Here, we resulted that DM,HTN, obesity, transplantation, and malignancy had an adverse effect on the PcP status among COVID-19 patients (Table 3). This can be a disputable finding. Immunosuppression, especially CD4+T cell dysfunction, is one of the main risk factors for opportunistic fungal infections, especially PcP[20]. While here, PcP was decreased by transplantation and malignancy among COVID-19 patients.
One limitation of this study is that pneumocystosis is considered one of the COVID-19 mimics. There are several overlaps in the diagnosis of PcP and COVID-19 superinfection. Therefore, CAP's prevalence and mortality rates may be affected and under-evaluated by the misdiagnosis of PcP cases as COVID-19 cases. Another limitation is that many CAP cases were presented by case report studies. According to guidelines in the prevalence meta-analysis,case reports and case series studies report a 100% prevalence rate and give false effects on the elevation of pooled prevalence rate,reporting biases, and heterogeneity[61-64].
The prevalence of PcP among the COVID-19 population is almost similar to the pre-COVID era. PcP-related mortality was decreased by the emergence of the COVID-19 pandemic. Women with COVID-19 are more susceptible to PcP than men. ARDS, KD,PD, and LTC increased the risk of PcP; surprisingly, transplantation and malignancy decreased the risk for PcP among COVID-19 patients. Unfortunately, there are many descriptive studies with duplicate content in the field of epidemiology of PcP, which are increasing every day. We suggest further retrospective, case-control,and prospective studies in this field. Avoiding the designing and publishing of descriptive studies without adding novel data to the field is recommended. Finally, more precisely systematic review and meta-analysis studies with lower heterogeneity rates are needed to add to the field and accurately establish the cause-and-effect relationships between PcP and COVID-19 infections.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Data availability
All data generated or analyzed during this study are included in this published article (and its Supplementary Information files).
FundingThis study has received financial support from the Vice Chancellor for Research & Technology Affairs, Shiraz University of Medical Sciences (Grant number: 26817).
AcknowledgmentsThe authors are grateful to the Vice Chancellor for Research &Technology Affairs of Shiraz University of Medical Sciences for the great support of this project.
Authors’contributionsHM, HK, HH, MB and SN performed initial searches, screened,and selected eligible studies. HM, RM, HK and EA evaluated the risk of bias assessment and quality control of included studies.HM, HK, SN, EA, HH, MB and RM extracted the data. HM and EA analyzed and interpreted the data. HM and HK drafted the manuscript. EA, HM, HH, MB performed revision.
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- Monkeypox awareness, knowledge, and attitude among undergraduate preclinical and clinical students at a Malaysian dental school: An emerging outbreak during the COVID-19 era
- Posttraumatic stress symptom trajectories of Chinese university students during the first eight months of the COVID-19 pandemic and their association with cognitive reappraisal, expressive suppression, and posttraumatic growth
- Long-term experience with debulking surgery in extensive hepatic alveolar echinococcosis: A case series and literature review
- Neurological paradox during treatment in a non-HIV patient with pulmonary tuberculosis: A case report
- Diversity of coronaviruses in wild and domestic birds in Vietnam
- Imminence: Cryptocurrency addiction and public health