Topological approach of liver segmentation based on 3D visualization technology in surgical planning for split liver transplantation
2022-11-30DongZhaoKangJunZhangTaiShiFangXuYanXinJinZiMingLiangJianXinTangLinJieXie
Dong Zhao,Kang-Jun Zhang,Tai-Shi Fang,Xu Yan,Xin Jin,Zi-Ming Liang,Jian-Xin Tang,Lin-Jie Xie
Dong Zhao,Kang-Jun Zhang,Tai-Shi Fang,Xu Yan,Xin Jin,Zi-Ming Liang,Jian-Xin Tang,Lin-Jie Xie,Department of Liver Surgery and Organ Transplantation Center,The Third People's Hospital of Shenzhen,The Second Affiliated Hospital of Southern University of Science and Technology,National Clinical Research Center for Ⅰnfectious Disease,Shenzhen 518000,Guangdong Province,China
Abstract BACKGROUND Split liver transplantation (SLT) is a complex procedure.The left-lateral and right tri-segment splits are the most common surgical approaches and are based on the Couinaud liver segmentation theory.Notably,the liver surface following right trisegment splits may exhibit different degrees of ischemic changes related to the destruction of the local portal vein blood flow topology.There is currently no consensus on preoperative evaluation and predictive strategy for hepatic segmental necrosis after SLT.AIM To investigate the application of the topological approach in liver segmentation based on 3D visualization technology in the surgical planning of SLT.METHODS Clinical data of 10 recipients and 5 donors who underwent SLT at Shenzhen Third People’s Hospital from January 2020 to January 2021 were retrospectively analyzed.Before surgery,all the donors were subjected to 3D modeling and evaluation.Based on the 3D-reconstructed models,the liver splitting procedure was simulated using the liver segmentation system described by Couinaud and a blood flow topology liver segmentation (BFTLS) method.In addition,the volume of the liver was also quantified.Statistical indexes mainly included the hepatic vasculature and expected volume of split grafts evaluated by 3D models,the actual liver volume,and the ischemia state of the hepatic segments during the actual surgery.RESULTS Among the 5 cases of split liver surgery,the liver was split into a left-lateral segment and right trisegment in 4 cases,while 1 case was split using the left and right half liver splitting.All operations were successfully implemented according to the preoperative plan.According to Couinaud liver segmentation system and BFTLS methods,the volume of the left lateral segment was 359.00 ± 101.57 mL and 367.75 ± 99.73 mL,respectively,while that measured during the actual surgery was 397.50 ± 37.97 mL.The volume of segment IV (the portion of ischemic liver lobes) allocated to the right tri-segment was 136.31 ± 86.10 mL,as determined using the topological approach to liver segmentation.However,during the actual surgical intervention,ischemia of the right tri-segment section was observed in 4 cases,including 1 case of necrosis and bile leakage,with an ischemic liver volume of 238.7 mL.CONCLUSION 3D visualization technology can guide the preoperative planning of SLT and improve accuracy during the intervention.The simulated operation based on 3D visualization of blood flow topology may be useful to predict the degree of ischemia in the liver segment and provide a reference for determining whether the ischemic liver tissue should be removed during the surgery.
Key Words: Three-dimensional visualization;Couinaud liver segmentation;Blood flow topology liver segmentation;Split liver transplantation;Surgical planning
INTRODUCTION
The Couinaud liver segmentation is based on the distribution of the Glisson system in the liver and the division of the hepatic vein system.Three hepatic veins are used as vertical planes to form the main longitudinal fissure,and the liver is divided into different liver segments by the left and right branches of the portal vein.This segmentation method provides an anatomical basis for the clinical imaging diagnosis of liver diseases and has been widely used in clinical practice[1-3].However,only 30%-50% of the segmented results are consistent with the actual anatomy of the liver as the segmented results are derived from the cast liver specimenex vivo,and the variation in hepatic blood vessels is not taken into account[4,5].The blood flow topology segmentation method is based on the blood flow topology of the hepatic portal vein[6,7].Therefore,this method can truly reflect the anatomical structure of the liver and is the theoretical basis of anatomical hepatectomyviaindocyanine green fluorescence imaging[8-10].
Split liver transplantation (SLT) is complex,and the commonly used surgical technique is the leftlateral segment and right tri-segment splits,which are implemented based on the theory of Couinaud liver segmentation.Previous studies uncovered that the right tri-segment liver surface might show different degrees of ischemic changes related to the destruction of the local portal vein blood flow topology following the intervention[11-13].
However,opinions diverge on the management of ischemia found on the surface tissues of the liver segment following SLT,as well as liver tissue necrosis,infection,and bile leakage[11,14].Some experts postulate that the direct resection of segment IV of the ischemic liver tissue is necessary,while others believe no treatment is needed.This difference in opinion is due to a lack of preoperative evaluation and predictive strategy for hepatic segmental necrosis after SLT and a dearth of relevant publications worldwide.Therefore,this study aimed to investigate the application value of 3D visualization technology in the surgical planning of SLTs.
MATERIALS AND METHODS
General clinical data
A retrospective analysis was performed on 10 patients who underwent SLT in the Third People’s Hospital of Shenzhen from January 2020 to January 2021 and the corresponding data of 5 donors.All cases in this study were performed after the approval of the Hospital Ethics Committee.The livers were donated after the death of the donors.
Pre-operation evaluation
For each organ donor,preoperative blood routine,liver function,kidney function,coagulation function,tumor markers,and infection-related tests,as well as abdominal Doppler ultrasound and liver computed tomography (CT) angiography examination,were performed.A preoperative 3D visualization model of the liver was constructed for each case.The model was acquired by importing highquality THIN-layer enhanced CT DICOM data into the medical 3D reconstruction software: (1) For organ reconstruction: The region-growing method was used to perform a 3D reconstruction of the liver,tumor,pancreas and spleen;and (2) For vascular reconstruction: The segmentation based on threshold method was used to perform a 3D reconstruction of the portal vein,hepatic artery and hepatic vein[15].The model was utilized to evaluate the vascular pattern and hepatectomy simulation.
Simulated surgery
(1) The SLT procedure was simulated on a 3D visualization model and included a segment of the hepatic artery,portal vein,and hepatic vein and the disconnection of the liver parenchyma;and (2) The SLT procedure was simulated according to the Couinaud liver segmentation and blood flow topology liver segmentation (BFTLS) methods.The volume of the two liver segments and the ischemic volume were also quantified (Figure 1).
Actual operation
The combination ofin-situandex vivosplitting was used for liver splitting.The surgical methods included left-lateral and right tri-segment splits,and left and right hepatic splits.During the operation,Doppler ultrasound was employed to identify and mark the shape of the middle hepatic vein,and a cavitron ultrasonic surgical aspirator and an ultrasonic knife were used to separate the liver parenchyma.
Main statistical indicators
The classification of hepatic vasculatures was based on 3D visualization technology,the hepatic and ischemic volume was estimated using simulated surgery,and hepatic ischemia was measured during the actual surgery.
RESULTS
Preoperative hepatic vascular evaluation and simulated surgical results.The preoperative 3D visualization model revealed that all the donor hepatic portal veins were Chenget al’s type I[16],the hepatic arteries were Michels[17] type I,the middle hepatic vein and left hepatic vein shared trunk in 5 cases,and a single hepatic vein of segment IV directly flowed into the inferior vena cava in 1 case.Among the 5 simulated operations,4 cases were split into left-lateral segment and right tri-segment;1 case was split into left and right half liver,and the middle hepatic vein was split by median segmentation.
The results revealed that the resection plane simulated by the Couinaud liver segmentation method or BFTLS method was inconsistent,the former was flat,while the latter was irregularly shaped.4 cases were simulated using left-lateral and right tri-segment splits.As measured by the above two liver segmentation methods,the volumes of the left-lateral segments were 359.00 ± 101.57 mL and 367.75 ± 99.73 mL,respectively.According to the BFTLS method,the volume of segment IV (i.e.,the ischemic part of the liver) cleaving to the right tri-segment was 136.31 ± 86.10 mL.1 case of left and right liver splitting was simulated,and median segmentation of the middle hepatic vein was performed after strictly evaluating two adult recipients with low body weight.The operation was simulated according to the above two segmentation methods.99.95 mL of tissues in segment IV was assigned to the left half of the liver according to Couinaud classification;if splitting was carried out according to this method,99.95 mL of liver tissues might experience postoperative ischemia or even necrosis.
Actual surgical results
In practice,in-situandex vivosplits were performed successfully according to the preoperative plan.According to the Couinaud liver segmentation method,left-lateral and right tri-segment splitting was performed in 4 cases.The left branch of the portal vein,the main trunk of the left hepatic artery,and the left branch of the hepatic vein were distributed to the left-lateral segment.The hepatic artery and portal vein branches entering segment IV of the liver were severed.The actual volume of the left-lateral segment was 397.50 ± 37.97 mL.The liver sections of the 4 cases exhibited ischemic changes after the operation (Figure 2).1 case experienced necrosis of the liver section and bile leakage and underwent reoperation to remove the necrotic tissues.The volume of the ischemic liver calculated before the operation was 238.7 mL.
In the other case,the operation was performed by left and right half liver splitting based on the portal vein BFTLS method.The middle hepatic vein was segmented in the middle,and the donor’s external iliac vein was used to reconstruct the middle hepatic vein of the left and right halves of the liver.No apparent changes in hepatic sectional ischemia were detected post-surgery (Figure 3).
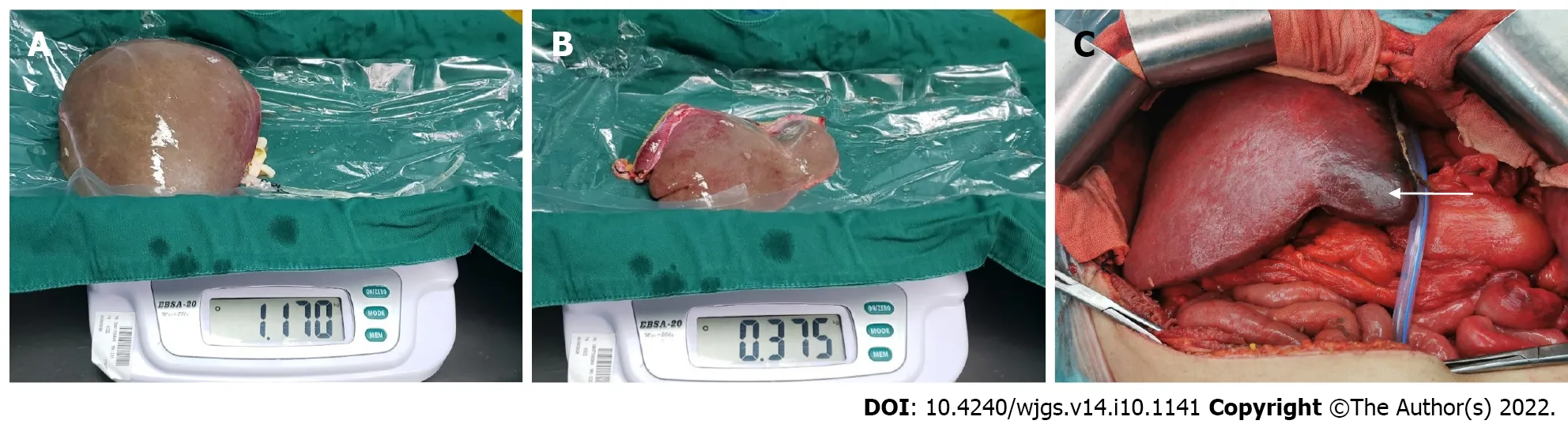
Figure 2 Based on the Couinaud liver segmentation method,left-lateral segment and right tri-segment splits were performed.
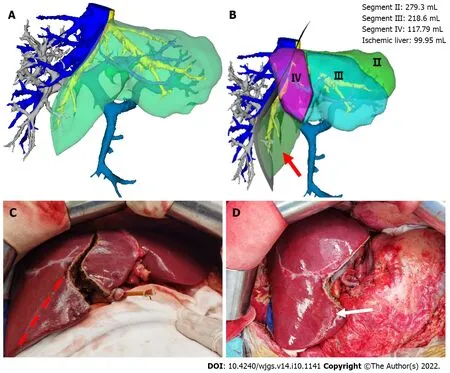
Figure 3 Left and right half-split liver transplantation was performed according to the portal vein blood flow topology liver segmentation method.
Post-transplant outcomes
The operation was successfully completed in all 10 patients corresponding to the split livers,and postoperative biliary leakage occurred in 1 case without small-for-size syndrome.During the perioperative period,1 patient who underwent a right tri-segment split suffered from a sudden intracerebral hemorrhage on the 7thpostoperative day and died on the 18thpostoperative day.
DISCUSSION
Couinaud liver segmentation is an artificial segmentation method based on anatomical markers of the liver.Moreover,its segmentation plane limits the drainage area of the hepatic vein and does not consider the topology of portal vein branches in the liver[6,7,18].For instance,when a vascular variation occurs in the liver,multiple portal or hepatic vein branches may co-exist within the same Couinaud liver segment.However,the BFTLS approach used herein was based on the topological structural relationship of the hepatic portal vein,which can truly display anatomical structural relationships in the liver[6,7].Indeed,this concept is also widely used in clinical practice[19-21].
The initial aim of SLT is to save two lives with a single liver.However,inappropriate preoperative evaluation of the liver donor or splitting method may bring a well-functional liver into 2 marginal donors,which may delay the recovery of graft function and even lead to graft failure or recipient death[22,23].Therefore,compared with other hepatobiliary surgeries,adequate preoperative evaluation of SLT is monumental.At the time of preoperative donor evaluation,enhanced CT of the liver must be performed,with initial vascular and biliary evaluation followed by re-evaluation based on the 3D visual model.If the donor has significant portal vein variation,SLT is not recommended to ensure the safety of both recipients.Herein,only donors with good liver function and no significant anatomical variation were included in the SLT cohort.All the patients undergoing SLT in our center underwent an initial simulation using the 3D visualization model,and the portal vein,hepatic vein,and hepatic artery were segmented accordingly.Furthermore,the liver volume was also calculated so that a detailed preoperative plan could be drawn up.
In this study,all patients underwent simulated surgeries using the Couinaud liver segmentation method and BFTLS method,and the measured volumes of the left-lateral segment were 359.00 ± 101.57 mL and 367.75 ± 99.73 mL,respectively.Moreover,according to the above two methods,the volume of the segment IV (the portion of the ischemic liver lobe) allocated to the right tri-segment was 136.31 ± 86.10 mL,obtained by adding the volume of segments Ⅱ/Ⅲ/Ⅳ minus the volume of the left-lateral segment.Based on these data,we can obtain a detailed evaluation of the surgery,predict the degree of ischemic tissue changes and necrosis in the liver segments,as well as assess the need to remove ischemic segments during liver transplantation.
Hepatic segmental ischemic necrosis is extremely common following SLT,mainly because the branches of the portal vein[13] and hepatic artery[14,24,25] entering this part of the liver are not connected,and the corresponding hepatic vein[26-28] may also be cut off in some cases.Therefore,this part of the liver may undergo pathological changes such as hepatocyte ischemia,necrosis,fibrosis,and atrophy,and in some cases,tissue necrosis and bile leakage.Indeed,one of the 5 cases in this study suffered from ischemic tissue necrosis and bile leakage on the surface of the right tri-segment.The necrotic tissue was eventually resected by reoperation in that particular case,with a preoperative ischemic liver volume of 238.7 mL.The ischemic areas of the right tri-segment in the other 3 cases,calculated preoperatively,were 76.9 mL,54.4 mL,and 175.3 mL,respectively.Therefore,we postulate that if the scope of hepatic segmental ischemia can be accurately determined before the operation,hepatic segmental tissue necrosis can be predicted in advance,avoiding reoperation and alleviating the pain and economic burden of patients.
CONCLUSION
In conclusion,in the case of the left-lateral segment and right tri-segment splits,preoperative evaluation based on three-dimensional visualization technology could calculate the ischemic range of the right trisegment.Judging by the results,the operator could predict the postoperative ischemic range and make clinical judgments accordingly.For instance,when the branches of the hepatic artery and portal vein of segment IV supplying the right tri-segment are disconnected,and the calculated ischemic range is large,the operator can directly remove this section during the operation to avoid further damage to the body due to tissue necrosis,infection or bile leakage.Nevertheless,due to the small number of cases,it was not possible to determine a specific cut-off value to predict the likelihood of postoperative hepatic ischemic necrosis.Therefore,it is imperative to include a large number of cases for future clinical or multi-center research.
ARTICLE HIGHLIGHTS
Research background
Split liver transplantation (SLT) is complex,and the commonly used surgical technique is the left-lateral segment and right tri-segment splits,which is implemented based on Couinaud liver segmentation.The right tri-segment liver surface may have different degrees of ischemic changes after SLT,which was related to the destruction of the local portal vein blood flow topology.
Research motivation
To our best knowledge,opinions diverge on the management of ischemia in surface tissues of the liver segment following SLT and there was no a consensus of pre-operative evaluation and predictive strategy for hepatic segmental necrosis after SLT worldwide.
Research objectives
Herein,we sought to investigate the application of the topological approach of liver segmentation based on 3D visualization technology in the surgical planning of SLT.
Research methods
A retrospective analysis was performed on 10 recipients and 5 donors who underwent SLT from January 2020 to January 2021.All the donor livers were subjected to 3D modeling and evaluation before surgery,based on which the liver splitting procedure was simulated by the Couinaud liver segmentation and blood flow topology liver segmentation (BFTLS) methods respectively,and the volume of the liver was calculated.Clinical data were analyzed,including the hepatic vasculature and expected volume of split grafts evaluated by 3D models,the actual liver volume,and the ischemia state of hepatic section in actual surgery.
Research results
The donor liver was split into a left-lateral segment and right tri-segment in 4 cases,while 1 case was split by left and right half liver splitting.According to Couinaud liver segmentation and BFTLS methods,the volume of the left lateral segment was 359.00 ± 101.57 mL and 367.75 ± 99.73 mL,respectively.The volume of segment IV (the portion of ischemic liver lobes) allocated to the right trisegment was 136.31 ± 86.10 mL as determined using the topological approach to liver segmentation.Yet,during the actual operations,ischemia of the right tri-segment section was observed in 4 cases,including 1 case of necrosis of the surfaces cut and bile leakage.
Research conclusions
The application of the topological approach of liver segmentation based on 3D visualization technology may be useful to predict the range of ischemia in the liver section and provide a basis for determining whether the ischemic liver tissue should be removed during the surgery.
Research perspectives
However,the follow-up studies with large samples are still warranted due to the relatively small number of cases.
ACKNOWLEDGEMENTS
We thank all the liver donors and patients.
FOOTNOTES
Author contributions:Zhao D conceived and designed,and made contributions to administrative support;Zhang KJ,Fang TS and Tang JX made contributions to providing research materials or patients;Liang ZM,Yan X,Jin X and Xie LJ collected and compiled data;Zhao D,Zhang KJ and Fang TS conducted data analysis and interpretation;All authors wrote the manuscript and contributed to the final approval of manuscript.
Supported byThe Third People's Hospital of Shenzhen Scientific Research Project,No.G2021008 and No.G2022008;Shenzhen Key Medical Discipline Construction Fund,No.SZXK079;Shenzhen Science and Technology Research and Development Fund,No.JCYJ20190809165813331 and No.JCYJ20210324131809027.
Institutional review board statement:The study was reviewed and approved by the Third People's Hospital of Shenzhen Institutional Review Board (Approval No.2022-133).
Informed consent statement:All study participants or their legal guardian provided informed written consent about personal and medical data collection prior to study enrolment.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Dong Zhao 0000-0003-3773-721X;Jian-Xin Tang 0000-0003-4416-5336.
S-Editor:Fan JR
L-Editor: A
P-Editor: Fan JR
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- Immunoglobulin G4-related disease in the sigmoid colon in patient with severe colonic fibrosis and obstruction: A case report
- Cecocutaneous fistula diagnosed by computed tomography fistulography: A case report
- Can DKI-MRI predict recurrence and invasion of peritumoral zone of hepatocellular carcinoma after transcatheter arterial chemoembolization?
- Reconstructing the portal vein through a posterior pancreatic tunnel:New choice for portal vein thrombosis during liver transplantation
- Long-term efficacy and safety of cap-assisted endoscopic sclerotherapy with long injection needle for internal hemorrhoids
- Performing robot-assisted pylorus and vagus nerve-preserving gastrectomy for early gastric cancer: A case series of initial experience