Decreased incidence of febrile neutropenia in Michigan following masking and social distancing orders for the COVlD-19 pandemic:A population based cohort study
2022-11-29MichaelGerardBaracyJrKarenHagglundSanjanaKulkarniFareezaAfzalKatherineArendsRobertMorrisLeighAnnSolomonMuhammadFaisalAslamLoganCorey
Michael Gerard Baracy Jr, Karen Hagglund, Sanjana Kulkarni, Fareeza Afzal, Katherine Arends, Robert T Morris, Leigh Ann Solomon, Muhammad Faisal Aslam, Logan Corey
Michael Gerard Baracy Jr, Sanjana Kulkarni, Fareeza Afzal, Leigh Ann Solomon, Department of Obstetrics and Gynecology, Ascension St. John Hospital, Detroit, MI 48236, United States
Karen Hagglund, Medical Research, Ascension St John Hospital and Medical Center, Detroit, MI 48236, United States
Katherine Arends, Surveillance and Infectious Disease Epidemiology Section, Michigan Department of Health and Human Services, Lansing, MI 48933, United States
Robert T Morris, Department of Obstetrics and Gynecology, Wayne State University School of Medicine, Karmanos Cancer Institute, Detroit, MI 48201, United States
Muhammad Faisal Aslam, Female Pelvic Medicine and Reconstructive Surgery, Ascension St. John Hospital, Detroit, MI 48236, United States
Logan Corey, Department of Gynecologic Oncology, Wayne State University, Detroit, MI 48202, United States
Abstract BACKGROUND It has been theorized that 75%-80% of febrile neutropenia (FN) is caused by endogenous pathogens, while up to 20% of cases are thought to be caused by a viral infection. It is unknown if precautions such as masking and social distancing reduce the risk of FN in susceptible populations.AIM To determine whether coronavirus disease 2019 (COVID-19) infection mitigation efforts, namely masking and social distancing, were associated with a reduction in the incidence of FN.METHODS This was a retrospective population based cohort study comparing the incidence of FN in the 13 mo prior to (Year 0) and 13 mo following (Year 1) the public health executive orders (PHEO) in Michigan. Data was queried for all emergency department (ED) visits from April 1, 2019 to March 31, 2021 from the National Syndromic Surveillance Program, a program which collects data that is voluntarily submitted by approximately 89% of Michigan EDs. The primary study outcome was the incidence of FN as a proportion of ED visits in the 13-mo before and 13-mo after COVID-19 mitigations efforts, namely masking and social distancing. We hypothesized that there would be a significant decrease in the incidence of FN in the period following the PHEO aimed at reducing the spread of the severe acute respiratory syndrome coronavirus 2 virus.RESULTS There was a total of 8979221 total ED visits captured during the study period. In Year 0 there were 5073081 recorded ED visits and 3906140 in Year 1. There was a significant reduction in the proportion of total ED visits with a diagnosis of FN, decreasing 13.3% across periods (0.15% vs 0.13%, P = 0.036). In patients with a hematologic malignancy a more impressive reduction in the incidence of FN was evident following PHEO (22% vs 17%, P = 0.02).CONCLUSION We found a significant association between social distancing and mask guidelines implemented on a large public scale with decreased rates of FN, particularly in those with a hematologic malignancy. These findings may be useful in the design of future research and recommendations regarding the prevention of FN.
Key Words: Febrile neutropenia; COVID-19; SARS-CoV-2; Malignancy; Hematology; Public health
lNTRODUCTlON
Febrile neutropenia (FN) is defined as neutropenia in the setting of a temperature greater than or equal to 100.4 degrees Fahrenheit and is one of the most common and costly complications associated with cancer treatment[1,2]. Granulocyte colony stimulating factor is the most effective prophylaxis against neutropenia and the progression to FN[3,4]. Yet, little is known about non-pharmacological strategies, such as masking, for the prevention of FN in at-risk populations.
Currently, FN prevention strategies include hand hygiene and the avoidance of sick contacts and crowds, however the impact of these efforts is uncertain[5]. Furthermore, the majority of FN with culture-proven bacteremia are thought to be the result of translocation of gut bacteria[6]. Although it has been theorized that 75%-80% of FN is caused by endogenous microorganisms, up to 20% of cases are thought to be caused by communicable pathogens, such as virions[7]. Accordingly, mitigating viral infection in at risks populations would theoretically reduce the incidence of FN. However, we are not aware of any population-based studies evaluating the impact of infection mitigation practices on the incidence of FN.
The public health crisis due to coronavirus disease 2019 (COVID-19) and its corresponding public health interventions provided a unique opportunity to evaluate the impact of social distancing and masking on the incidence of FN. In March of 2020, the state of Michigan issued an Executive Order that urged residents to remain at home and socially distance, which was amended shortly thereafter to include a mask mandate[8]. The aim of our study was to evaluate the association of these mitigation efforts and the incidence of FN in patients presenting to emergency departments (EDs) in the state of Michigan.
MATERlALS AND METHODS
This is a retrospective cohort study comparing the incidence of FN in the 13 mo prior to (Year 0, March 1, 2019-March 31, 2020) and the 13 mo following (Year 1, April 1, 2020-April 31, 2021) the public health executive orders (PHEO) in Michigan. Approximately 89% of EDs across Michigan voluntarily submit encounter data (patient’s chief complaint, associated diagnoses, age, sex, intake temperature, intake percent oxygen saturation, and blood pressure) to the National Syndromic Surveillance Program (NSSP). A query was made for all encounters with a diagnosis of Neutropenia (ICD-10-CM D70) from March 1, 2019-April 31, 2021. FN was defined as an intake temperature greater than or equal to 100.4 degrees Fahrenheit and an ICD-10-CM D70. The incidence of FN in Year 0 was compared to the incidence of FN in Year 1. To account for the impact of the COVID-19 pandemic on total ED visits, the incidence of each ICD code was analyzed as a proportion of ED visits for the corresponding year. Associated ICD-10-CM codes were grouped according to Clinically Relevant Groups (CRG) (Supplementary Table 1), modified from the Healthcare Cost and Utilization Project[9]. Analysis of the incidence of FN in each CRG was also performed. A visit containing multiple ICD-10-CM diagnostic codes was included in multiple CRGs, if applicable. This study was deemed exempt by the responsible institutional review board.
Statistical analysis
Descriptive statistics were generated to characterize the study cohorts. Continuous variables are described as the mean with standard deviation or median with range or interquartile range. Categorical variables are described as frequency distributions. Univariable analysis of factors associated with FN were assessed using Student’st-test, analysis of variance, and the chi-squared analysis. Multivariable analysis was done using logistic regression. Analyses were conducted using SPSS version 25.0 and aPvalue less than 0.05 was considered statistically significant.
RESULTS
From March 1, 2019 to April 31, 2021 there were 8979221 total ED visits in the state of Michigan with data submitted to the NSSP and at least one viable ICD-10 code. In Year 0, there were 5073081 recorded ED visits and 3906140 in Year 1, a decrease of 23% (Table 1). There was a total of 5717 encounters with a diagnosis consistent with neutropenia. There was a significant reduction in the proportion of total ED visits with a diagnosis of FN, decreasing 13.3% from Year 0 to Year 1 (0.15%vs0.13%,P= 0.036).
In a sub-analysis of all patients with FN, in patients with a concomitant diagnosis of hematologic malignancy, FN was significantly lower in the period following PHEO (22%vs17%,P= 0.02, Table 2). In Year 0 there was a 29.3% incidence of FN in neutropenic patients with a CRG of hematologic malignancy,vsa 21.2% incidence in neutropenic patients without a CRG of hematologic malignancy (P< 0.0001, Figure 1). This difference was not observed in Year 1 (23.8%vs20.2%,P= 0.12). Hematologic malignancy was the only CRG diagnosis to have a relatively higher rate of FN in Year 0 compared to Year 1.
DlSCUSSlON
The public health response to COVID-19 in the state of Michigan provided a unique opportunity to analyze the impact of social distancing and masking on the incidence of FN. Masking and social distancing designed to prevent the spread of COVID-19 have resulted in the decline of other non-covid viral illnesses[10,11]. Our study is the first to document an association between this phenomenon and a decline in the incidence of FN, both overall and in patients with an ICD-10-CM diagnosis consistent with hematologic malignancy.
In the majority of cases, the underlying cause of FN is unknown, and therefore little is known about the efficacy of non-pharmacological efforts to prevent development of FN in neutropenic patients[12]. We found a significant association between the implementation of public health measures to prevent the spread of communicable diseases and the incidence of FN associated with hematologic malignancies. This is an important finding as patients with hematologic cancers are particularly vulnerable to FN and its associated morbidity and mortality[13]. Our findings suggest that a significant proportion of FN in patients with malignancy may have a viral etiology. Accordingly, health measures, such as masking, may reduce the risk of FN in vulnerable patients.

Table 1 Baseline demographics

Table 2 Frequency of clinical relevant group diagnosis among patients with neutropenic and febrile neutropenia in Year 0 and Year 1
Strengths and limitation
The strengths of this study include a large number of encounters and associated accurate objective data points (ICD codes and temperature). Additionally, Michigan adopted the stay-at-home orders and mask mandates quickly and broadly, with one of the highest compliance rates of the country during Year 1 (Supplementary Figure 1)[14]. As a result, our results likely accurately reflect the effect of COVID-19 mitigation efforts on FN.
Our study has several limitations in addition to the inherent vulnerability to unmeasured biases found in retrospective studies: (1) There may be a small number of encounters of FN that are missed in this dataset; (2) Only the intake vital signs were available, and a temperature of 100.4°F was selected as the cutoff for diagnosing FN (rather than 101 F) in an effort to have a more inclusive cohort; (3) Each ED visit was treated as a separate encounter. Therefore, a patient with FN who presented to the ED on multiple occasions would be captured multiple times; (4) It is impossible to account for individual patient hesitancy on presenting to ED[14]; (5) Charts review was not possible, so the effect of active myelosuppressive therapy could not be assessed; and (6) The number and identify of facilities contributing data changes over time, and the use of diagnosis codes could be inconsistent across and within facilities.
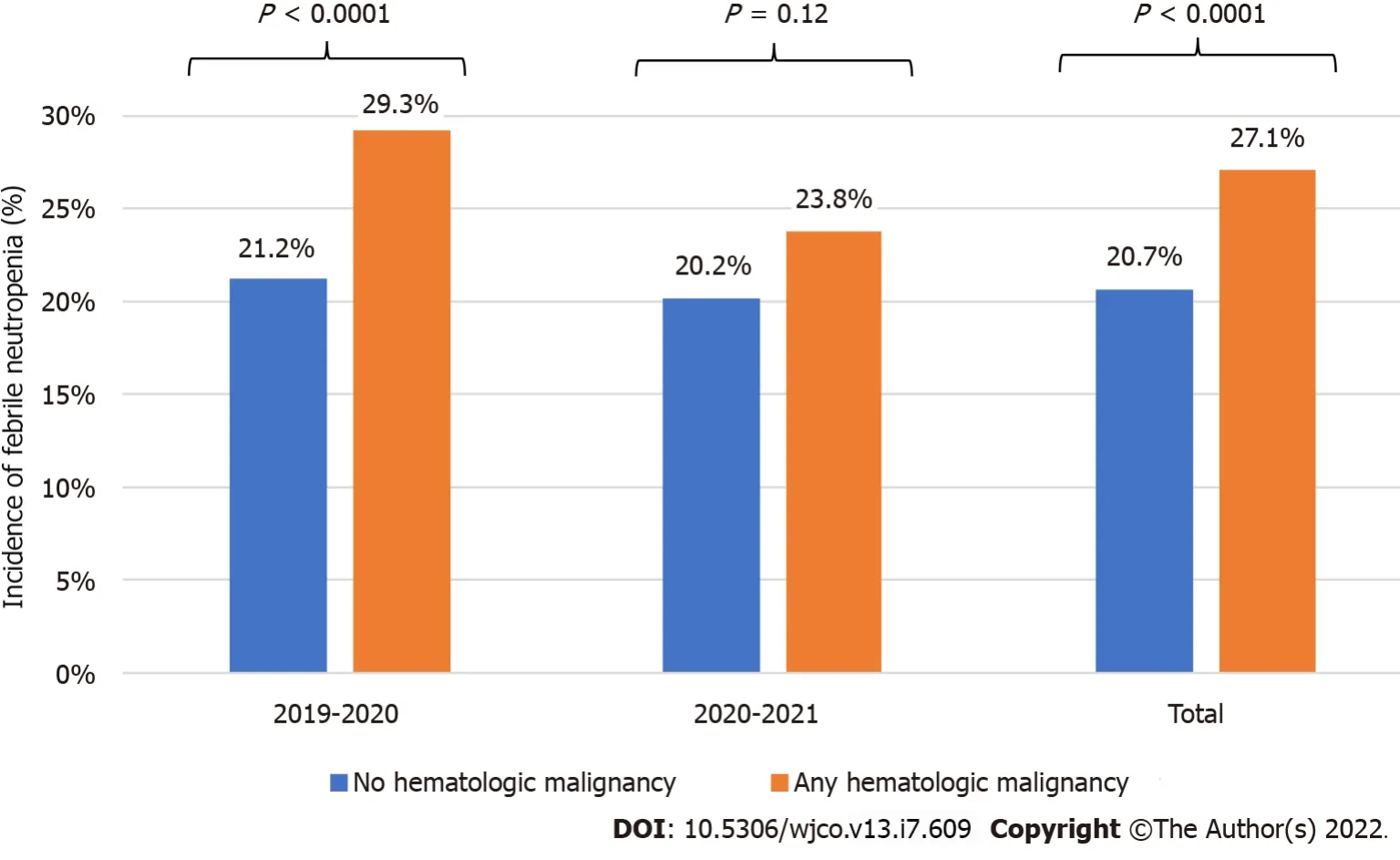
Figure 1 lncidence of febrile neutropenia in patients with an associated diagnosis of hematologic malignancy compared to those without a diagnosis of hematologic malignancy.
CONCLUSlON
Our study found a significant association between the implementation of social distancing and mask guidelines and the incidence of FN in ED patients with neutropenia. This reduction was most pronounced in those with a hematologic malignancy. These findings may be useful in the design of clinical trials as well as informing future recommendations for the prevention of FN in vulnerable patients.
ARTlCLE HlGHLlGHTS
Research background
It has been theorized that 75%-80% of febrile neutropenia (FN) is caused by endogenous pathogens,while up to 20% of cases are thought to be caused by a viral infection. It is unknown if precautions such as masking and social distancing reduce the risk of FN in susceptible populations.
Research motivation
There has been a proven reduction in respiratory viruses (e.g., flu, common cold, etc.) with the implementation of social distancing and masking in the effort to prevent the spread of coronavirus disease 2019 (COVID-19). We sought to elucidate whether such public health measures would concomitantly reduce the incidence of FN in susceptible populations, namely those with malignancies.
Research objectives
To determine whether COVID-19 infection mitigation efforts, namely masking and social distancing,was associated with a reduction in the incidence of FN.
Research methods
This is a retrospective population based cohort study comparing the incidence of FN in the 13 mo prior to and 13 mo following the public health executive orders in Michigan. Data was queried for all emergency department visits from April 1, 2019 to March 31, 2021 from the National Syndromic Surveillance Program.
Research results
There was a significant reduction in the proportion of total ED visits with a diagnosis of FN, decreasing 13.3% across periods (0.15%vs0.13%,P= 0.036). In patients with a hematologic malignancy a more impressive reduction in the incidence of FN was evident following PHEO (22%vs17%,P= 0.02).
Research conclusions
Masking and social distancing appear to decrease the risk of FN in susceptible populations, especially among patients with hematologic malignancies.
Research perspectives
Masking and social distancing appear to decrease the risk of FN in patients with malignancies, supporting the theory that a proportion of FN may be secondary to communicable infectious particles. Well-designed studies and clinical trials are needed to guide recommendations regarding masking and social distancing for the prevention of FN in vulnerable patients.
ACKNOWLEDGEMENTS
We would like to acknowledge the staff from the MDHHS for their help in data collection and management, especially Henderson J.
FOOTNOTES
Author contributions:Corey L conceived of the idea; Baracy Jr MG and Corey L designed the protocol and wrote the manuscript; Baracy Jr MG and Corey L organized operative diagnoses, CPT codes, ICD-9 and ICD-10 codes and ensured the integrity of codification; Hagglund K verified the protocol was methodologically sound and analyzed the data; Arends K procured the data; Kulkarni S, Afzal F, Solomon LA, Morris RT and Aslam MF were integral in the design and execution of the project; all authors discussed the final results and contributed to the final manuscript.
lnstitutional review board statement:The study was reviewed and approved by the Ascension St. John Hospital Institutional Review Board (approval No. 1783486-1).
lnformed consent statement:Informed consent has been waived by the Ascension St. John Hospital Institutional Review Board.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:The dataset is available from the corresponding author at Michael.Baracy@ascension.org. Consent was not obtained but the presented data are identified and risk of identification is low.
STROBE statement:The authors have read the STROBE Statement-checklist of items, and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORClD number:Michael Gerard Baracy Jr 0000-0003-2437-3541; Karen Hagglund 0000-0003-2089-063X; Sanjana Kulkarni 0000-0001-8481-3831; Fareeza Afzal 0000-0002-0158-8999; Muhammad Faisal Aslam 0000-0002-4101-0382; Logan Corey 0000-0003-2880-7546.
S-Editor:Gao CC
L-Editor:A
P-Editor:Gao CC
杂志排行

World Journal of Clinical Oncology的其它文章
- Nanomedicine approaches for treatment of hematologic and oncologic malignancies
- Simple approach for the histomolecular diagnosis of central nervous system gliomas based on 2021 World Health Organization Classification
- Edmonton Symptom Assessment Scale may reduce medical visits in patients undergoing chemotherapy for breast cancer
- Awareness, knowledge, and attitudes towards sun protection among patients with melanoma and atypical mole syndrome
- Short term safety of coronavirus disease 2019 vaccines in patients with solid tumors receiving systemic therapy
- iCEMlGE: lntegration of CEll-morphometrics, Mlcrobiome, and GEne biomarker signatures for risk stratification in breast cancers