Practice and patronage of traditional bonesetting in Ondo State, Nigeria
2022-10-10NafiuFatihudeenOKOROAdelekeAraoyeOJOOluwaseyiAbiodunAKPOROgheneroborBenjaminAKPOR
Nafiu Fatihudeen OKORO, Adeleke Araoye OJO, Oluwaseyi Abiodun AKPOR, Oghenerobor Benjamin AKPOR
1Department of Nursing Science, Afe Babalola University, Ado‑Ekiti, Ekiti State, Nigeria; 2Department of Nursing, Adeleke University, Ede Osun State, Nigeria; 3Department of Biological Sciences, Afe Babalola University, Ado‑Ekiti, Ekiti State, Nigeria
ABSTRACT Objective: This study was carried out to investigate the determinants of the practice and patronage of traditional bonesetting (TBS) in a Local Government Area of Ondo State, Nigeria.Materials and Methods: A descriptive research design approach with purposive sampling technique was used. Data collection was through the use of two set of self-developed structured questionnaire (for bonesetters and clients). The study obtained data from eight traditional bonesetters and fifty-six inpatients receiving treatments in the bonesetters’ homes across the study location.Results: Findings from the study showed that the major cause of fractures were road traffic accidents while low cost of treatment was the major influence for patronizing traditional bonesetters. The study also revealed that majority of the traditional bonesetters had little or no formal education. Among the sociodemographic characteristics of the participants, only occupation showed signification relationship with reasons for patronage of TBS homes (χ2 = 28.164, P = 0.036).Conclusion: The patronage of traditional bonesetters may be impossible to eradicate; thus, the study recommends the need for collaboration among traditional bonesetters and modern orthopedic practitioners through recognition and continuous training of the traditional bonesetters on appropriate management and referrals.
Keywords: Practice, traditional bonesetters, traditional bonesetting, treatment

Access this article online Quick Response Code Website:www.journalin.org DOI:10.4103/jin.jin_6_22images/BZ_44_966_2775_1202_3011.png
INTRODUCTION
Traditional bonesetting (TBS) is a specialization in the traditional medical treatment that is passed from one generation to the next. This is similar to other traditional practices that is maintained along the family lines in form of traineeship with rare admission of nonfamily members as trainees.[1-2]In most part of the developing world, traditional bonesetters have continued to receive high patronage of large proportion of fracture cases due to their availability and good local reputations.[2]The practice of TBS is extensive in Nigeria with enormous patronage by the populace. Mbadaetal.[3]and Thanni[4]asserted that people from all levels of socioeconomic status in society including the educated and the affluent patronize the services of traditional bonesetters.Cardetal.[5]and Agarwal and Agarwal[6]stated in their studies that globally, between 10% and 40% of patients who suffered from fractures and dislocations received the services of unorthodox practitioners. The mode of care delivery of TBS cannot be ignored in Nigeria as up to 85% of patients with fractures would first visit them before their presentation at the hospital. According to Dadaetal.,[7]many Nigerians still believe that the TBS are efficient in the management of bone disorders probably due to cultural beliefs, poverty, and ignorance. Onyemaechietal.[8]reported that traditional bonesetters managed about 70%-90% of primary fracture care in many rural communities in Nigeria.
Orthodox and traditional medicines coexist side by side and patients patronized both. It is indicated that traditional and orthodox fracture management have been in existence for several decades in Nigeria.[9,10]Nevertheless, sense of interference and rivalry has been the features of the relationship of the orthopedists and the traditional bonesetters. Even though many practitioners of traditional bonesetters assume that the generational informal training they receive from their forefathers is superior to the training received by orthodox medical practitioners while many orthopedic surgeons appositely insisted that traditional bonesetters are untrainable apart from being a menace to the Nigeria society.[8]
The practice of TBS has been passed on by the practitioners from one generation to another but it is still masked in mystery as the practitioners kept it as family secret yet, the patrons of this service cut across the rich and the poor.[11]One of the obvious faults of the practice of TBS in Nigeria is the process of training and skills acquisition by the practitioners, which is not only informal, undocumented and uncontrolled but coupled with attendant continuous reduction training and information hoarding. Moreover, the practice is usually passed to the next generation orally with no written document, regulation, review or the required peer evaluation. Thus, the quality of the services rendered is not certain and there is high possibility of complications. This is in contrast to orthodox training which is not only regulated and open but also subjected to constant review owing to new evidences.[7]
Despite the shortcoming in training and outcomes of fracture treatment by TBS, their services still command high patronage and confidence in their communities.[9,12]Thus, the study aimed at investigating the determinants of the practice and patronage of TBS in a Local Government Area of Ondo State, Nigeria.
MATERIALS AND METHODS
Design and setting
The study area was one of the Local Government Areas in Ondo State, Nigeria. A descriptive, nonexperimental research design was used in the study.
Participants
The target population for the study were all traditional bonesetters and their patients in the research setting. At present, there are eight TBS homes located in the study area. Total sampling technique was used to recruit all available consented traditional bonesetters, while 56 patients were purposively selected.
Inclusion criteria for the study were all patients above the age of 19 years who had fracture within the last 12 months, treated by the bonesetters whether still on admission or has been discharged, and willingness to participate in the study. Exclusion criteria were aged <19 years; diagnosis not up to 12 months; and those who did not consent to participate in the study.
The sample size was determined by the degree of variability, whereby the minimum suggested sample was 30 and upper limit was 100. A total of 64 participants which include eight traditional bonesetters and 56 patients (current and old) participated in the study.
Data collection
Data collection was through the use of two set of structured questionnaires (one for the traditional bonesetters and the other for their patients). The researcher visited traditional bonesetting homes during visiting hours and obtained the desired information directly from the admitted patients and out patients (those who have completed their treatment). The interview scheduled for patients was organized into sections that included questions on respondents’ sociodemographic characteristics, knowledge of bonesetting belief about efficacy of the treatments, and factors responsible for preference for TBS homes over the modern hospital. The second questionnaire scheduled for practitioners include questions on practitioners’ sociodemographic characteristics, their training, skills and belief about practice, acquisition of knowledge and skill.
Statistical analysis
Information gathered from the respondents was analyzed using the Statistical Package for Social Sciences (SPSS) version 21.00 (IBM corp released 2012 Armonk, NY, USA: IBM Corp). Data were presented as descriptive and inferential statistics. Relationships were tested for using theChi-square test. All analysis were carried out at probability level of 0.05.
Ethical considerations
Before the commencement of the study, approval was obtained from the Ondo State Research and Ethics Committee of the Ministry of Health with protocol number OSHREC August 28, 2021/370 on September 22nd, 2021. Permission was also obtained from the Primary Health Care Board of the Local Government Area in Ondo State, Nigeria. Informed consent was obtained and participants’ anonymity was maintained. Participants were not coerced to be part of the study and their names or any form of identification were not required in the administered questionnaires.
RESULTS
Participants’ sociodemographic profile and cause of fracture
Sociodemographic profile of the participants with bone fracture revealed that the 42.9% of the participants were between age 31 and 40 years and 73.2% were married. A total of 48.2% were secondary school leavers while only 8.9% had tertiary education. In addition, 30.4% of the participants were civil servants. The participants’ fractures profile revealed that 92.9% of them had their fracture through road traffic accidents [Table 1].
Reasons for the patronage of traditional bonesetters
Generally, 62.5% attributed their reason for patronage of traditional bonesetters to low cost of treatment. Also, 14.3% of the participants patronized traditional bonesetters because of fear of amputation while 8.9% patronized traditional bonesetters due to their traditional belief. In addition, 7.1% and 5.4% of the participants indicated they patronized bonesetters based on the influence of others and advice of friends, respectively. Only 1.8% of the participants attributed their reason of patronage of traditional bonesetters to avoidance of protocol. Among the sociodemographic characteristics of the participants, only occupation (χ2= 28.614,P= 0.036) was observed to be significantly associated with reasons for the patronage of traditional bonesetters [Table 2].
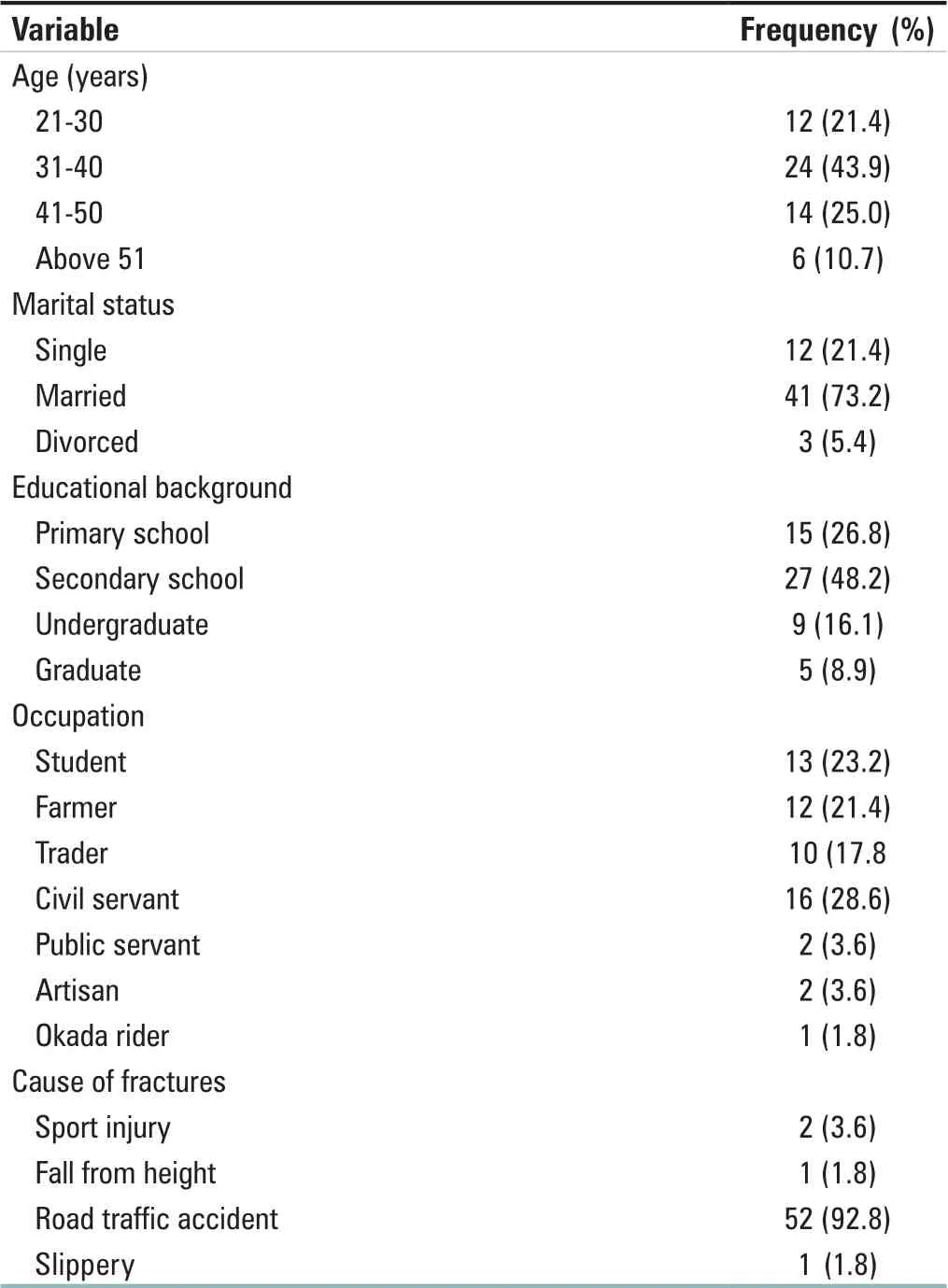
Table 1: Sociodemographic profile of the participants (n=56)
Procedures and methods of practice of traditional bonesetters
Generally, all the traditional bonesetters have been in the practice of bonesetting for over 5 years and 75.0% were trained in the practice of bonesetting by their parents. On how they diagnose patient with fracture(s), all participants were observed to follow a similar pattern of diagnosis. On their treatment method and how they know if a fracture has healed, 87.5% indicated they observed the absence of gap between the broken fragment and ensure there is no deformity at the affected part while 12.5% indicated they observed return of painless easy movement of affected part. In the case of how they treat complications, 62.5% reported that they refer the patient to orthodox medical setting/hospital [Table 3].

Table 2: Relationship of sociodemographic characteristics of the participants with reasons for the patronage of traditional bonesetting (n=56)
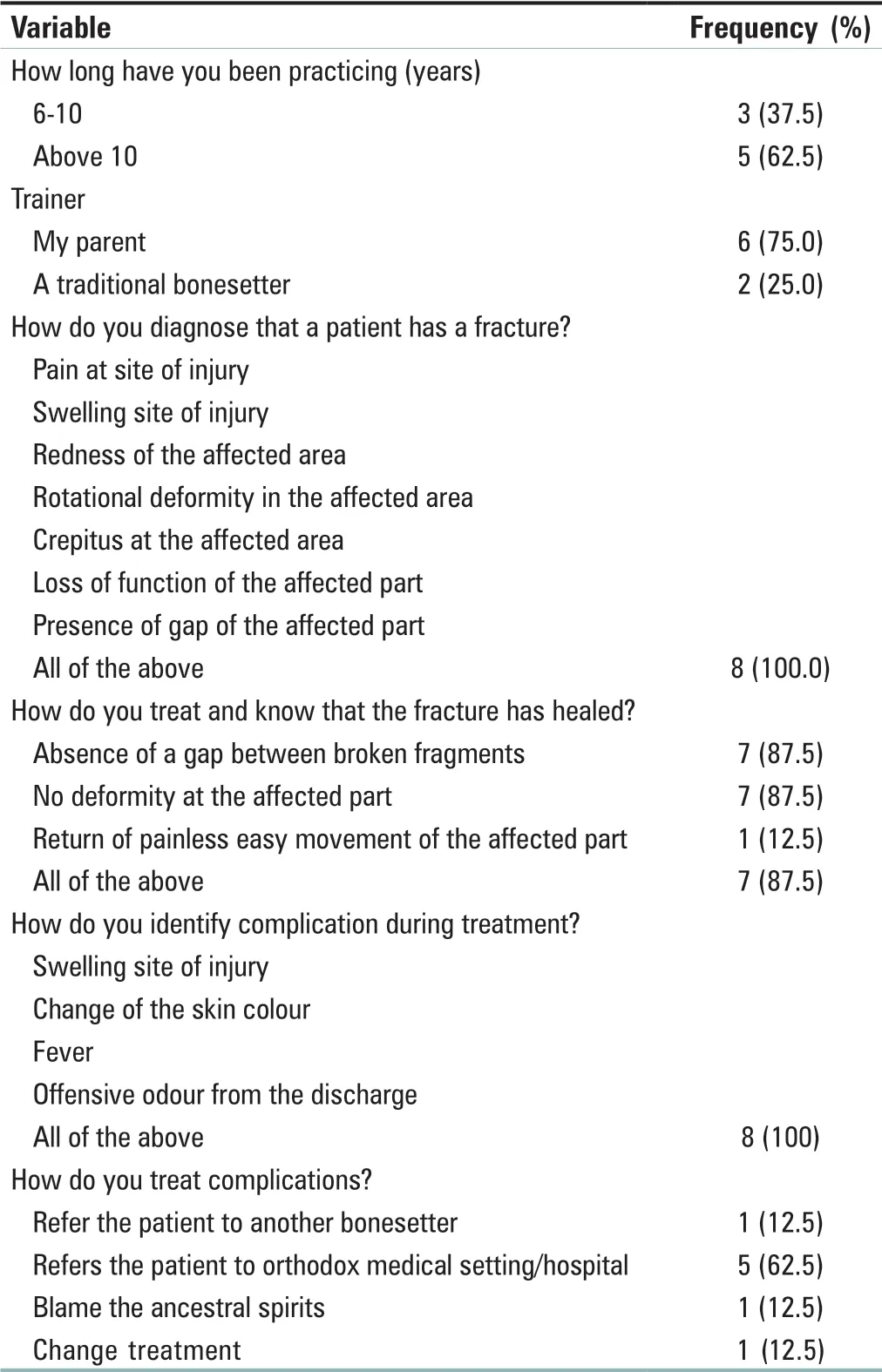
Table 3: Procedures and methods of practice of the traditional bonesetters
DISCUSSION
From the findings of the study, the major cause of fracture among the study participants was road traffic accidents. The observation was similar to an earlier study conducted by Owumietal.,[1]A similar study on the effect of gender on the rate of fracture by Sawetal.,[13]indicated that the overall rate of fracture was higher in men (75.3%) as against women (24.7%). The reasons for the difference in occurrence may be due to the nature of both gender daily activities, the relative amount of travel and the traditional role of women as house wives.[13]As shown in a related study conducted in Nigeria, 76.0% of the study participants had open fractures of the lower limbs that were indicated to have occurred due to motorcycle accidents.[12]
On the effect of socioeconomic status on patronage of traditional bonesetters, the study revealed that people who patronized traditional bonesetter cut across all groups of socioeconomic status.[1,7,14]Some of the reasons alluded to for the patronage of traditional bonesetters were low cost, easy accessibility, quick services, cultural belief, influence from families and friends and fear of amputation in the orthodox setting. This observation was in agreement with the findings of previous investigators.[1,7,14]Abangetal.,[14]argued that cultural beliefs, ignorance, and suggestion from family and friends, short supply of trained orthodox workers in rural areas, faster and cheaper services as well as the fear of amputation in the hospitals are some of the possible reasons for high demand of TBS services. As stated by Ruhinda,[15]rehabilitation of patients is not a usual part of TBS services as not all patients treated by TBS are readmitted to conventional hospitals, except those with hitches. It can then be presumed that many patients especially those with minimal displaced fractures would have been successfully treated by the TBS. Findings from a study on the reasons for the patronage of TBS conducted by Abangetal.,[14]and Mbadaetal.,[3]showed that 29% of patients seen at the orthopedic outpatient clinics have patronized TBS centres, and majority of the patients were males. Treatment duration can be as long as 18 months for a patient with closed femoral shaft fracture who despite the long duration of treatment may still end up with a nonunion fracture. It was revealed that a total of 79.3% of the patients in the study were admitted immediately after their injuries with some having multiple fractures. A related study on the behaviour of patients with long bone fractures that are treated by traditional bonesetters in Nigeria highlighted factors, such as cheaper fees, pressure from friends, incantations and concoction utilization, quick service, cultural belief and ease of accessibility as reasons for the patronage of traditional bonesetters.[16]In addition, Nwadiaroetal.,[17]reported reasons adduced for patronage of traditional bonesetters to be inconsistent but could broadly be based on fixated cultural outlook.
In this study, a good number of the participants were satisfied with the treatment provided by the traditional bonesetters. A similar observation was reported by Owosenietal.,[18]in a related study that was conducted in Nigeria. In the study, 49.8% of respondents were reported to have indicated that the treatment outcome of traditional bonesetters was excellent. This finding is however at variance with the observation of Cardetal.,[5]who in their study on patient patronage and perspectives of TBS at an outpatient orthopedic clinic in Northern Tanzania, reported a higher negative perception regarding bonesetters, with the main reason for patients not utilizing traditional bonesetters’ services as concern for competency. While a similar study reported patients’ preference for TBS due to sociocultural beliefs and affordability.[19]Furthermore, another related study on knowledge, attitude, and practice of bonesetters in rural areas in Nigeria indicated that the services of traditional bonesetters are vital in the maintenance of healthy life. The subjects also indicated healing of fractures treated by traditional bonesetters were more effective than orthodox medicine.[3]
In this study, only occupation was observed to be significantly associated with reasons for patronage of traditional bonesetters. In a related study on factors influencing patronage and continuing popularity of traditional bonesetters, it was indicated that educational level of the study’s respondents did not seem to influence their patronage of TBS.[4,19,20]Their services are cheaper and patients also believed their healing methods are quicker.[19,21]Factors influencing the patronage of TBS include the use of plaster of Paris, extended period of immobilization with lower risk of amputation. Also, indifferent attitudes of conventional hospitals or wheedling by families, neighbors, and their supporters may influence patronage of potential clients. Similarly, traditional bonesetters are regarded as ‘specialists’ for minor fractures, that can be easily accessible, with reassuring services that include home treatment and thus they enjoy strong regional influence and popularity.[4,14,21,22]
Most of the traditional bonesetters investigated in this study had more than 10 years’ experience in bonesetting, two-thirds indicating they were trained by their parents. This is in line with the assertion of Owumietal.,[1]that the practice of TBS is an age long practice that is shrouded in mystery and often passed from father to child from one generation to another.[7,11]A similar observation on the source of their knowledge in bonesetting has been reported.[18]In the study of Owosenietal.,[18]it was reported that majority of traditional bonesetters got into the art of bonesetting through either self-education or training from parents and relatives.
Bonesetting practitioners often keep their knowledge as a family secret although some non-family members do received training via apprenticeship.[1]Equally, Owosenietal.[18]in their study on traditional bonesetters and fracture care in Ekiti State, Nigeria stated that the source of the knowledge in bonesetting is from self-education, parents or from relatives. As revealed in this study, the usual method of identifying fracture in a patient as mentioned by the TBS were the presence of pain at the site, swelling of the affected area, redness, rotational deformity, crepitus, loss of function and presence of a gap on the affected bone. This is similar to the findings of Odatawa-Omagbemietal.,[2]in a study conducted in Delta State Nigeria, which revealed that TBS have similar methods of fracture diagnoses and treatment. A study on the role of TBS in the care of primary fracture in Nigeria by Onuminya[16]indicated that the practice of bonesetting is a well-preserved family practice, with training majorly by apprenticeship. The study further reported that bonesetting records are preserved and kept by oral tradition. It is also reported that diagnosis of fracture is mainly by physical assessment and experience.
Limitations of the study were that the study was be conducted within a setting, hence it will be difficult to generalize the findings without some form of bias. In addition, the study population was restricted to a limited number of the traditional bonesetters and its attendant’s population of patients that patronize the TBS homes.
CONCLUSION
From the findings of this study, it is concluded that road traffic accidents are major cause of fractures. Patients patronize traditional bonesetting homes over modern orthopedic services due to low cost of treatment, majority of these patients are not educated. Similarly, majority of the practitioners have no knowledge of the importance of the orthodox fracture treatment. Notwithstanding, it may be difficult to stop their activities taking into consideration the level of trust and assurance they enjoyed from their clients. Modern orthopedic services are more effective than traditional bonesetting procedures, as a result of complications and longer duration of treatment involved in traditional bonesetting procedures. The patronage of traditional bonesetters may be impossible to eradicate thus, the study recommends the need for collaboration among traditional bonesetters and modern orthopedic practitioners through recognition and continuous training of the traditional bonesetters on appropriate management and referrals for the benefit of both parties. Higher complication rate occurred among TBS; thus, it will also be beneficial if affordable and accessible hospital services especially orthopedic care can be provided in public health facilities as this could reduce clients’ patronage as well as the likely complications that may arise from TBS services.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
杂志排行

Journal of Integrative Nursing的其它文章
- Nursing perspective of expert consensus on the diagnosis and treatment of cerebral infarction with integrated traditional Chinese and Western medicine
- Does educational intervention change knowledge, attitude, and practice regarding pharmacovigilance among nursing officers in Central lndia? An interventional study
- Research capacity and training needs of nurses’ in Shanghai, China: A multicenter, cross-sectional survey
- Referral and counter-referral practices in obstetric emergencies among health-care providers in selected health facilities in Plateau state, Nigeria
- Nurses and nursing students’ knowledge regarding blood transfusion: A comparative cross-sectional study
- Faculty of health sciences students’ knowledge and attitudes toward coronavirus disease 2019 during the first wave of the pandemic: A cross-sectional survey