Return to work following shoulder arthroplasty:A systematic review
2022-09-22SimonLalehzarianAvineshAgarwallaJosephLiu
lNTRODUCTlON
Over the last two decades,the number of shoulder arthroplasties,including total shoulder arthroplasty (TSA),reverse TSA (rTSA),and shoulder hemiarthroplasty (HA),has increased at exponential rates[1-4]. TSA has typically been indicated for end-stage shoulder conditions in individuals with intact rotator cuff and sufficient glenoid bone stock to allow for stable glenoid component implantation[1-4]. The TSA procedure involves replacing the humeral head and glenoid with similarly shaped prosthetic components. rTSA,on the other hand,was historically indicated for patients with massive rotator cuff tears and involves using a convex glenoid hemispheric ball and a concave humerus articulating cup to reconstruct the glenohumeral joint. HA has traditionally been indicated in patients with glenohumeral arthritis where the glenoid bone stock is inadequate for TSA[1-4]. This procedure involves removing the humeral articular surface and replacing it with a stemmed humeral component.
Due to satisfactory clinical and functional long-term outcomes,the number of shoulder replacements performed will continue to rise into this next decade,with models predicting between 174810 and 350558 procedures by 2025[2,5,6]. Historically,shoulder replacements have been performed in elderly patients for degenerative shoulder conditions; however,these procedures are becoming more prevalent in younger and more active populations[5-8]. Furthermore,individuals born between 1981 and 1996 make up the largest generation of workers in the U.S. Labor Force[9]. With younger individuals who compose a significant amount of the workforce receiving shoulder replacements,patients will begin to place a higher priority on their ability to return to work (RTW) following shoulder arthroplasty.
Bow-wow! That was the end of happiness! The Snow-man, however, was not listening to him any more; he was looking into the room where the housekeeper lived, where the stove stood on its four iron legs, and seemed to be just the same size as the Snow-man
Prior studies have shown varying levels of RTW after shoulder arthroplasty based on arthroplasty type,diagnosis,and work intensity[10-12]. While informative,a compilation comparing various demographics,arthroplasty types,diagnoses,and work intensities has not been performed in recent years. The purpose of this systematic literature review and analysis is to summarize outcomes of RTW following TSA,rTSA,and HA as well as analyze the effects of workers’ compensation (WC) status on rates and ability to RTW.
During the following months I watched Rebekah struggle with the ravages9 of chemotherapy. Her hospital stays became frequent and she worried about her children. Meanwhile I continued to contend with raising my own kids. They always seemed either out or holed up in their rooms. I missed the days when they were as attached to me as Rebekah s little girls were to her.
MATERlALS AND METHODS
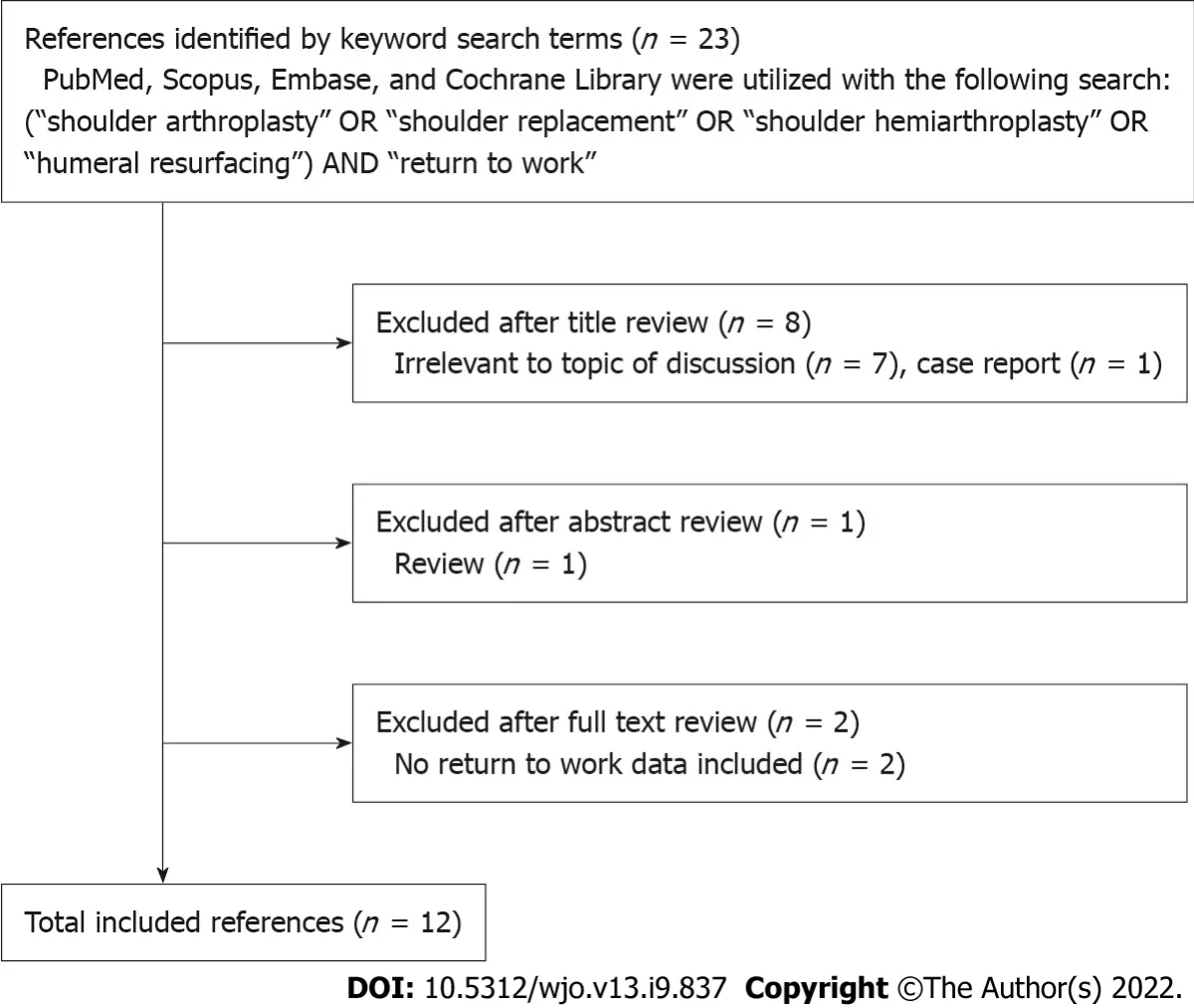
In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines,a systematic review and analysis was performed[13,14]. The PubMed,Scopus,Embase,and Cochrane Library databases was queried using the search terms “shoulder arthroplasty”,“shoulder replacement”,“shoulder hemiarthroplasty”,or “humeral resurfacing” combined with “return to work”. The(https://www.referencecitationanalysis.com/) software was also used to identify any additional studies. The final search was performed on January 8,2021. Additionally,the references of each study were manually assessed as well for potential inclusion in this investigation. The flow diagram summarizes the progression of the literature review with 12 total references meeting the inclusion criteria (Figure 1).
Clinical studies were evaluated and included if they were in English,had level of evidence I to IV,and reported on RTW after shoulder arthroplasty. Nonclinical studies,literature reviews,case reports,and those not reporting on RTW after shoulder arthroplasty were excluded. Title and abstract reviews were performed by two of the study authors (Lalehzarian SP and Liu JN). The full texts of articles meeting inclusion criteria based on title and abstract were then reviewed by two of the study authors (Lalehzarian SP and Agarwalla A) for final inclusion in the study. As referenced in Figure 1,23 references were initially identified by the keyword search terms described above. After the title review,8 references were excluded as 7 were irrelevant to the topic of discussion and 1 was a case report. One reference was excluded after abstract review as it was a review article and two references were excluded after full text review as they did not include RTW data. Following the review process,there were 12 references left and all were included in this review.
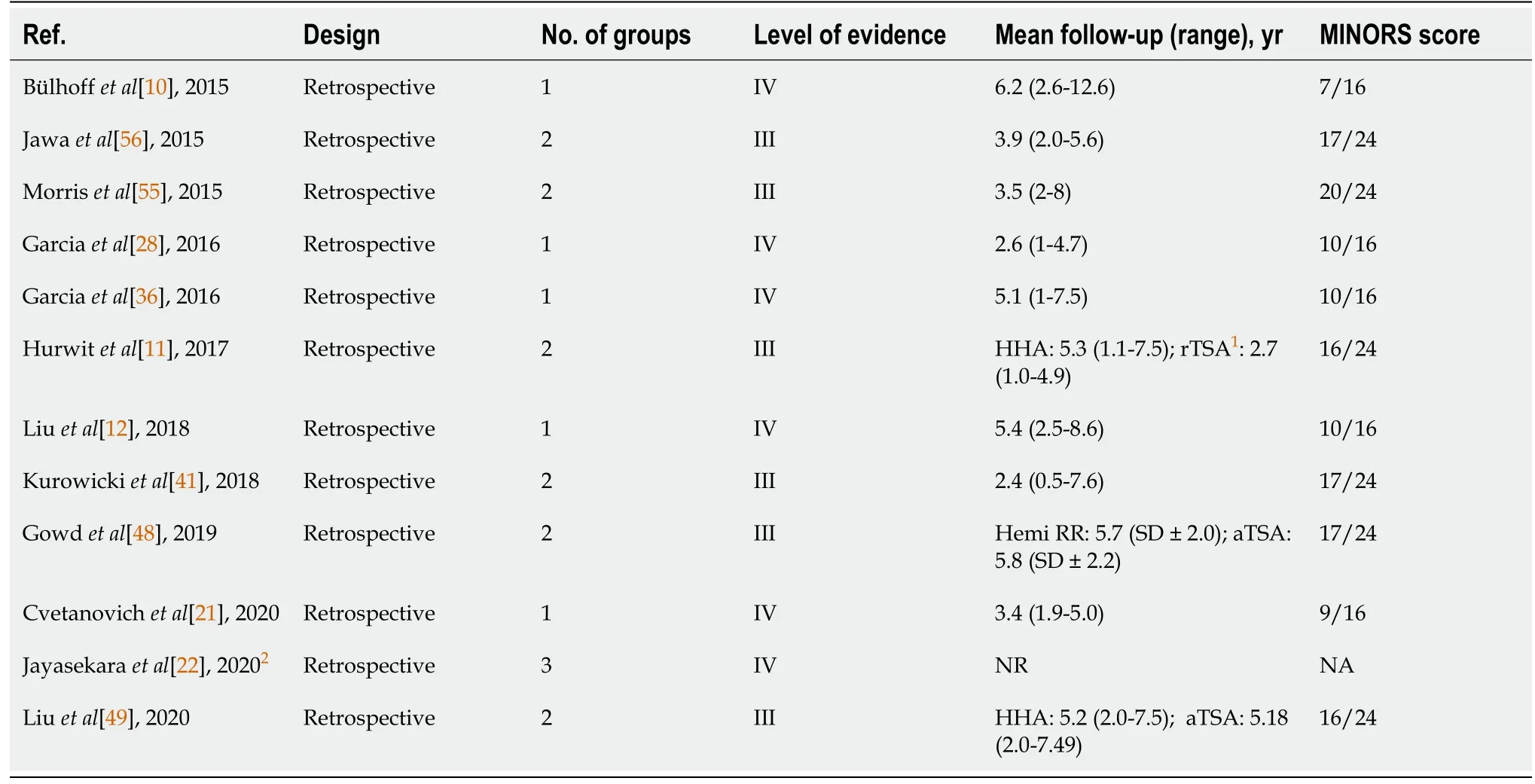
Included studies were evaluated using the Methodological Index for Non-Randomized Studies (MINORS) checklist[15]. Studies were evaluated on 8 items to 12 items,with each scored 0 (not reported),1 (reported but poorly or inadequately done),or 2 (reported,well done and adequate),with a maximum score of 16 and 24 for noncomparative and comparative studies,respectively. Articles were scored by one of the study authors (Lalehzarian SP) and confirmed by two of the study authors (Agarwalla A and Liu JN). An analysis of the 12 total articles is shown in Tables 1-3.
RESULTS
RTW after TSA
TSA has shown to be a highly effective treatment for degenerative shoulder disease with adequate longterm outcomes,low revision rates,and high implant survivorship[7,16]. The number of anatomic total shoulder arthroplasties has increased from 29414 in 2011 to 40750 in 2017 partly due to an increased demand from younger populations and expanded indications[2,17-20]. With this increase in demand and volume,RTW following anatomic TSA is an important metric for many employed patients.
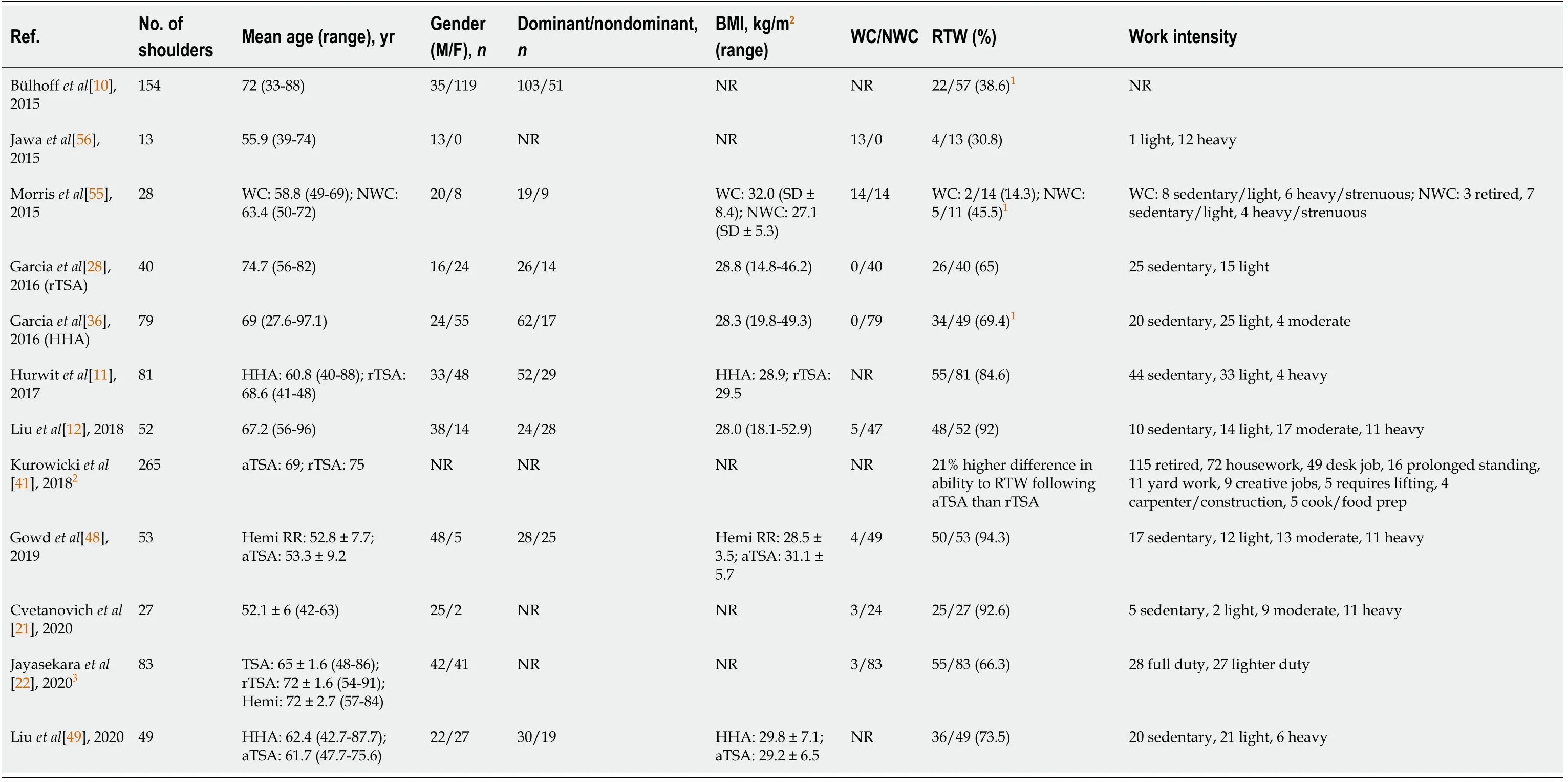
In a study by Bülhoff[10],57 TSA patients were analyzed after meeting inclusion criteria. At the most recent follow-up,22 total patients (39%) returned to work. It is important to note that 6 patients (11%) cited their inability to pursue work at the time of most recent follow-up due to shoulder problems. While the authors concluded that approximately 61% of their patients did not retire or cease their vocation because of TSA,a large number of patients who were not working at final follow-up had retired from work[10]. This major limitation could be responsible for a low rate of RTW.
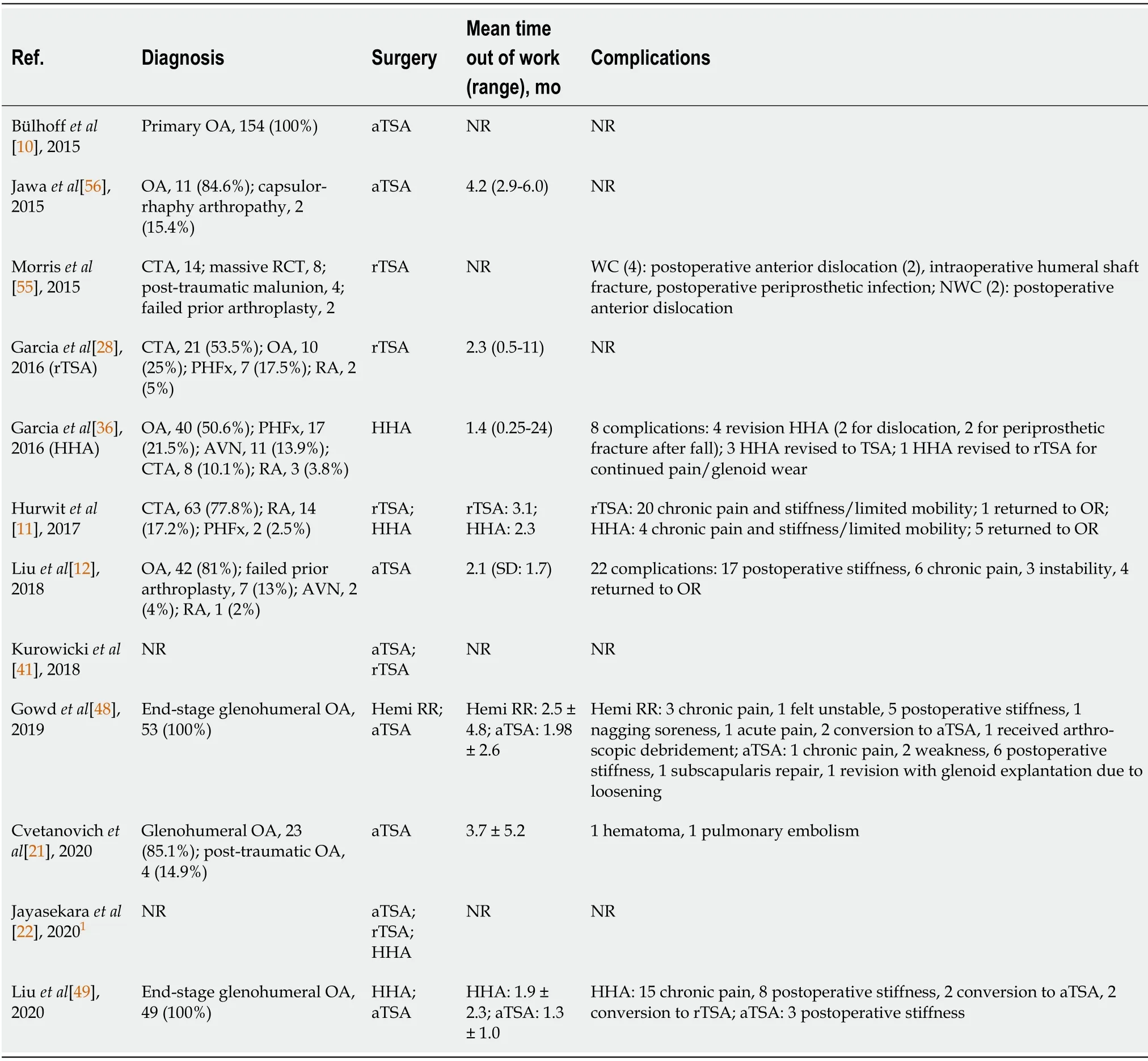
Gowd[48] analyzed 53 total patients with glenohumeral arthritis. Twenty five patients (average age of 52.8 years) received HA with ream-and-run resurfacing and 28 patients (average age of 53.3 years) received TSA. Of the 25 patients undergoing HA,all 25 (100%) were able to RTW at an average duration of 1.98 mo. On the other hand,25 (89%) of 28 patients receiving TSA were able to RTW with an average time of 2.5 mo following surgery. When HA patients were stratified preoperatively into work demand level,7 patients were categorized as sedentary,7 were light,4 were moderate,and 7 were heavy. For TSA,10 patients were categorized as sedentary,5 were light,9 were moderate,and 4 were heavy. Postoperatively,all HA patients (100%) in sedentary,light,and moderate were able to RTW. For TSA,9 (90%) of 10 returned to sedentary work,while all (100%) light and moderate duty patients returned to work. For the heavy category,7 (100%) of 7 HA patients were able to return compared to 2 (50%) of 4 TSA patients demonstrating that heavy duty workers undergoing HA had a significantly higher rate of RTW[48]. Of the 2 TSA heavy duty patients who were unable to RTW,only one reported permanent restriction with overhead lifting. Despite this difference,authors concluded near equivalent rates of RTW between HA and TSA.
The majority of patients were able to return to work following TSA,rTSA,or HA. Understanding outcomes for rates of return to work following shoulder arthroplasty should assist surgeons and patients in managing expectations in clinical practice.
The available data suggests that the majority of patients who undergo rTSA are able to RTW at rates between 56% and 65%. Despite this low percentage,the volume of rTSA continues to rise due to expanding indications[2].
In summary,the majority of studies cited a rate of RTW between 71% and 93% with an average duration of 1 mo to 4 mo following TSA[12,21]. Furthermore,most patients who undergo TSA are able to RTW at the same preoperative intensity level with the exception of those patients in heavy intensity jobs who are less likely to RTW after TSA.
RTW after rTSA
Mom, the kids asked, who was that? Why did you give her our flowers? Is she somebody s mother? The mother said she didn t know the old woman. But it was Mother s Day, and she seemed so alone, and who wouldn t be cheered by flowers? Besides, she added, I have all of you, and I still have my mother, even if she is far away. That woman needed those flowers more than I did.
Garcia[28] conducted a study on 40 patients who had undergone rTSA. Of the 40 patients analyzed,26 (65%) of them were able to RTW with an average time of 2.3 mo. From the 14 patients who did not RTW,only two of them retired due to shoulder reasons while the other 12 retired due to nonorthopedic causes. When stratified into intensity level,rates were comparable to the overall rate of RTW with 17 (68%) of 25 patients returning in the sedentary class and 9 (60%) of 15 returning in the light class. Additionally,patients with sedentary jobs returned to work more quickly than those with light work (1.4 mo4.0 mo).
Jayasekara[22] evaluated 34 rTSA patients,with 19 (56%) of them able to return to some type of work at the 6 mo follow-up. Eight of the 19 patients who returned to work were able to RTW with full duties and the other eleven returned to work with lighter duties. From the twelve surgeries included in the study,rTSA was associated with the lowest rate of RTW at 56%. Jayasekara[22] concluded that this percentage is consistent with prior studies which cited a 65% rate of RTW[11,28].
In a large clinical series by Jayasekara[22],1773 patients were examined. TSA was one of the twelve surgeries analyzed with a total number of 38 patients. At the six month follow-up,27 (71%) patients were able to return to some type of work:14 (37%) patients returned with full duty,13 (34%) patients returned with lighter duty,and 11 (29%) patients were unable to RTW. Of the twelve surgeries analyzed,TSA at 71% was shown to have a lower rate of RTW compared to surgeries such as HA and rTSA which had 82% and 56%,respectively[22]. This lower rate of RTW may have been due to a higher average age of patients who underwent TSA compared to those in previous studies; therefore,the age of the patients may have negatively influenced their desire and ability to RTW[22].
RTW after HA
Traditionally,HA was considered a safer option compared to TSA or rTSA for patients who wished to remain active following surgery due to its low failure rate and utilization of an intact glenoid[29]. Despite exponential rises in TSA and RTSA,the rate of HA procedures has steadily declined from 15860 in 2011 to 6150 in 2017[2]. This is in part due to the increase in rTSA for shoulder replacement. Since the indications for rTSA have been expanded to include fractures,the rate of HA for fracture use has decreased by nearly 30%[30-32]. Additionally,recent studies have shown that clinical outcomes from HA are significantly inferior to that of TSA and that patients undergoing HA had statistically significantly worse functional scores[11,33-35]. With this steady decline over the last decade,there is much necessity for a clinical review that examines all available literature regarding the rates of RTW for HA.
Garcia[36] examined 49 patients who worked preoperatively and underwent HA. Thirty-four (69.4%) patients were able to return to previous employment at an average duration of 1.4 mo. Preoperatively,20 (41%) patients classified their jobs as sedentary,25 (51%) patients as light physical work,and 4 (8%) patients as moderate physical work. Following HA,15 of 20 (75%) patients returned as sedentary,17 of 25 (68%) patients as light physical work,and 2 of 4 (50%) patients as moderate physical work. While no patients changed job demand level postoperatively,the average time to return to employment varied:1.9 mo for sedentary,2.6 mo for light,and 13.1 mo for moderate. As one of the first studies to analyze the rates of RTW following HA,Garcia[36] was able to quantify evidence that aided physicians in managing expectations of patients undergoing shoulder HA.
Jayasekara[22] included 11 patients who underwent shoulder HA. Nine (82%) patients were able to return to some type of work at 6 mo follow-up with 6 (55%) patients able to return to full duties,3 (27%) able to return to lighter duties,and 2 (18%) unable to RTW. While the reason for not returning to work was not cited,it may be due to the fact that the average age of patients undergoing HA in this cohort was 72 years of age. Although a limitation of this study was a smaller size,Jayasekara[22] found higher rates of RTW despite an average age much higher than previous studies[11,36].
Recent literature has shown rates of RTW for shoulder HA between 69% and 82% compared to both TSA and rTSA[22,36]. Despite higher rates of RTW for HA compared to rTSA,the number of HA cases continues to decline with poor functional outcomes at long-term follow-up[11,37].
Comparison of RTW between TSA and rTSA
In patients with end-stage glenohumeral arthritis and an intact rotator cuff,TSA has shown to be a highly effective treatment with high rates of functional recovery[5]. While the original indication for rTSA was rotator cuff arthropathy,the indications for rTSA have expanded to include conditions such as TSA and HA implant failures,complex proximal humerus fractures,asymmetric glenoid wear,posterior humeral head subluxation in patients with intact rotator cuffs,and irreparable rotator cuff tears in the absence of arthritis[38-40]. Similarly,the indications for TSA have also expanded to now include a more diverse and active patient population[41]. As younger patients undergo shoulder replacements,many patients cite their ability to work as instrumental in their decision to have surgery. With increased indications for both surgeries,assessing the ability of patients to RTW following TSA and rTSA is imperative to educate future patients and manage expectations.
In one recent study,Kurowicki[41],evaluated 159 patients undergoing TSA (average age 69) and 106 patients undergoing rTSA (average age 75). Authors used the American Shoulder and Elbow Surgeons (ASES) Assessment Form as a way to track patients’ ability to RTW. Among usually reported work,it is important to note that 43% of patients cited retirement as their work,with housework (27%) and desk jobs (18%) as the second and third most cited,respectively. Kurowicki[41] reported a 21% higher difference in overall ability to work for patients following TSA compared to those patients who underwent rTSA. In particular,statistically significant differences were found between TSA and rTSA amongst patients who cited their work as housework or gardening.
Kurowicki[41] is the only study that compares the ability of TSA patients to RTW to rTSA patients. Based on this study,authors concluded that returning to work after TSA is more favorable than rTSA in fields of work that require low-demand activities such as housework and gardening[41]. This study was limited by its reporting bias from survey-based studies,small sample size within work subgroups,and population representation differences particularly in age. Regardless,comparisons among these groups hold importance in defining patient and surgeon expectations after surgery.
Comparison of RTW between TSA and HA
If non-operative treatment for glenohumeral osteoarthritis with intact rotator cuff integrity fails,patients are often told to consider HA or TSA. While the optimal surgical treatment remains controversial,there are benefits to both procedures. Multiple studies have shown that patients with glenohumeral arthritis who undergo TSA have improved pain relief,higher functional scores,and more range of motion compared to those who undergo HA[35,36,42-44]. However,TSA also has an increased operative time,more blood loss,more technical difficulty,and incurs the risk of glenoid loosening[45]. On the other hand,while HA has the benefits of decreased operative time,decreased blood loss,and less technical difficulty,there is some concern regarding the progression of arthritic changes especially with bone loss and the need for future revision surgeries such as conversion to TSA[45,46]. Furthermore,many patients have lifting restrictions after TSA,which may limit their ability to RTW[47].
Liu[12] reported on 52 patients (54 shoulders),who were 55 years or younger at the time of surgery,worked in the 3 years leading up to surgery,and were available for a minimum follow-up of 2 years. Forty-eight patients (92%) were able to RTW postoperatively at an average of 2.1 mo after surgery. In addition to calculating the rate of RTW,the authors stratified patients by intensity of work:sedentary,light,moderate,or heavy. Forty one of 41 (100%) patients who had sedentary,light,or moderate work preoperatively were able to return to the same level of work. However,only 7 of 11 (64%) patients who had heavy-intensity work preoperatively were able to RTW. Of the 4 patients who did not RTW,only one patient cited shoulder pain and limited range of motion as the reason[12]. Additionally,the intensity of work was positively correlated with time to RTW. The authors found a statistically greater time to RTW when comparing heavy intensity (4.2 mo) to sedentary,light,and moderate intensity,respectively.
He fell very ill, sent for doctors of every kind, even bonesetters, but they, none of them, could find out what was the matter with him, or even give him any relief
Liu[49] evaluated 49 total patients with end-stage glenohumeral osteoarthritis. Twenty-six patients underwent HA (average age of 62.4 years) and 23 patients underwent TSA (average age 61.7). Sixteen (62%) of 26 HA patients were able to RTW at an average duration of 1.88 mo following surgery. Of the patients undergoing TSA,20 (87%) were able to RTW at an average time of 1.29 mo following surgery. From the 10 HA patients who did not RTW,only one had retired postoperatively due to shoulder issues. The other nine patients retired preoperatively due to the shoulder,other medical reasons,or postoperatively due to non-specified reasons. Of the three TSA patients who did not RTW,zero had retired postoperatively due to the shoulder. Patients either retired preoperatively due to the shoulder,other medical concerns,or non-specified reasons. For patients who underwent TSA,7 (100%) of 7 returned to a sedentary work demand level,9 (82%) of 11 returned to a light work demand level,and 3 (100%) of 3 returned to a heavy work demand level (Table 4). For patients who underwent HA,8 (62%) of 13 returned to a sedentary work demand level,7 (70%) of 10 returned to a light work demand level,and 1 (33%) of 3 returned to a heavy work demand level (Table 4). (68%) of 25 returned to a sedentary work level and 9 (60%) of 15 returned to a light work demand level (Table 4). Liu[49] concluded that patients with osteoarthritis undergoing TSA have higher rates of RTW and function compared to those undergoing HA.
Morris[55] compared 14 WC patients who underwent rTSA to a matched cohort of 14 patients without WC status who also underwent rTSA. From the patients with WC claims,only 2 (14%) of 14 were able to RTW. Of the 12 patients who were not able to RTW,one was unemployed and seeking employment at the time of follow-up,five were disabled,and six had retired following rTSA. In the matched cohort of non-WC patients,only 11 patients had worked prior to the surgery. From these 11 patients,5 (46%) were able to RTW,one was disabled,and five had retired after rTSA. No patients,WC or non-WC,were able to return to heavy/strenuous work demands after rTSA. Despite significant improvement from preoperative to final follow-up outcomes,WC patients had significantly worse Constant scores,ASES scores,Western Ontario Osteoarthritis of the Shoulder Index scores,and less external rotation compared with the matched cohort group. Morris[55] reported that while WC patients had significant improvements following rTSA,they achieved significantly worse outcomes compared to non-WC patients after rTSA.

From these two studies,there is still a discrepancy in terms of ability to RTW between HA and TSA. The mixed results could potentially be due to the limitations of each study. For example,in Gowd[48],surgeons counseled their TSA patients that they would have permanent overhead lifting restrictions,whereas those who underwent HA would not receive these restrictions. Comparatively,in Liu[49],surgeons placed no postoperative work restrictions on either group. Furthermore,the average age of individuals in Gowd[48] (52.8 and 53.3 years of age) was significantly lower than the average of individuals in Liu[49] (62.4 and 61.7 years of age) possibly indicating that older patients either hold more sedentary,less demanding occupations or may benefit more in their ability to RTW following TSA compared to HA[48,49].
In 2003,the United States Food and Drug Administration approved the use of rTSA for rotator cuff arthropathy[1,23]. Since that time,the volume of rTSA has drastically increased,from 21916 in 2011 to 63845 in 2017,in part due to its encouraging results and expanded indications to cover proximal humerus fracture and previous failures of arthroplasty[24-27]. When comparing the number of rTSA to the total number of shoulder replacements from 2011 and 2017,the percentage has increased from 33% to 58%[2]. Due to the exponential increase in rTSA use,a clinical review outlining the rate of RTW after rTSA will assist orthopedic surgeons in treating future patients with shoulder conditions.
Comparison of RTW between HA and rTSA
When TSA is contraindicated,in cases such as rotator cuff or deltoid dysfunction,deficiencies in glenoid bone stock,or proximal humerus fractures,patients must be educated on the benefits and drawbacks of HArTSA[50]. Many studies over the last decade have shown more predictable and superior outcomes for rTSA compared to HA[51-53]. Yet,in the younger population,especially those who want to remain employed following surgery,surgeons often feel more comfortable recommending HA given the theoretical risk of glenoid component loosening or failure in rTSA[54]. Furthermore,surgeons tend to place more activity restrictions on patients who undergo rTSA,which could significantly limit their ability to RTW.
Take gold and silver with you, and a large retinue2 of servants, as beseems two noble princes, and go through the world till you find out who it is that steals my golden apples, and, if possible, bring the thief to me that I may punish him as he deserves
Hurwit[11] compared 40 rTSA patients (average age of 68.6 years) to 41 HA patients (average age of 60.8 years) all of whom had end-stage glenohumeral arthritis with rotator cuff dysfunction,deficiencies in glenoid bone stock that prohibited the insertion of an anatomic glenoid component,or proximal humerus fracture. Of the patients who underwent rTSA,26 (65%) of them were able to RTW at an average duration of 2.3 mo following surgery. Only two patients who were unable to RTW cited their main reason as issues with the shoulder following surgery,while the other twelve either retired preoperatively due to medical reasons or non-specified reasons. Twenty-nine (71%) of the 41 HA patients were able to RTW at an average time of 3.1 mo after surgery. In this cohort,only one patient retired postoperatively due to shoulder issues. The other eleven had retired preoperatively due to the shoulder,medical reasons,or non-specified reasons. For patients who underwent HA,14 (74%) of 19 were able to return to a sedentary work demand level,13 (72%) of 18 returned to a light demand level,and 2 (50%) of 4 returned to work at a heavy work level (Table 5). For patients who underwent rTSA,17 (68%) of 25 returned to a sedentary work level and 9 (60%) of 15 returned to a light work demand level (Table 5). Hurwit[11] concluded no significant difference between the two groups in terms of return to low- and moderate-intensity work,despite an older age for patients undergoing rTSA.

Despite a higher rate of RTW for HA patients,no significant differences were found by Hurwit[11]. A potential limitation with this study was the significant difference in average age of each cohort (68.6 years for rTSA patients and 60.8 years for HA patients),even though this did not affect RTW rates[11]. Furthermore,this study only had sufficient sample sizes for sedentary and light duty workers. Due to the lack of heavy duty workers,especially in rTSA,it is possible to hypothesize that heavy laborers may have experienced more difficulty in returning to work.
Comparison of RTW between WC and non-WC
Work-related injuries are a common cause of disability in the United States and have significant implications for workers,employers,insurers,and physicians[18,55,56]. WC status has shown to have a detrimental effect on clinical outcomes following orthopedic surgery[57,58]. The impact of WC status on postoperative outcomes is an important consideration for patients undergoing shoulder arthroplasty.
2. Tumbled out of its ears: This version of the story was sanitized for a Victorian sensibility. In the original story by Charles Perrault, the donkey s feces are gold.Return to place in story.
In Jawa[56],a cohort of 13 WC patients (average age of 55.9 years) who underwent TSA were compared to a control group of 63 patients (average age of 63.2 years) who also underwent TSA. While RTW rates were not cited for the control group,only 4 (31%) of the 13 WC patients were able to RTW following TSA. Of the four patients who returned,one returned to the same job with lifting restrictions and the other three changed jobs to those that require less lifting. From the nine patients who did not return,7 did not return due to functional restrictions after the surgery and 2 had retired. Additionally,Jawa[56] found the ASES score to be significantly lower in the WC cohort compared to the control group. From this study,authors concluded no WC patients were able to return to full duty work at their current job and that WC patients receiving TSA had poorer outcomes compared to non-WC patients.
Despite the lack of difference in RTW rates following shoulder arthroplasty for patients with or without WC claims,many studies in orthopedic literature have found poorer outcomes,lower satisfaction rates,and more pain in patients with WC status after shoulder arthroplasty[55,56,59,60]. Similar findings exist in the shoulder literature outside of shoulder arthroplasty. For example,in numerous rotator cuff studies,patients with WC status have been found to be significantly less compliant with postoperative protocols and have less improvement in functional outcomes and pain after controlling for confounding factors such as age,marital status,education level,preoperative expectations,work demands,smoking,comorbidities,duration of symptoms,size of tear,and repair technique[61-64]. Furthermore,other similar results have been found in WC cohorts undergoing acromioplasty,superior labral anterior-posterior tear,and biceps tenodesis for failed superior labral anterior-posterior repair[65-68]. Regardless of procedure type,the differences in pain and outcomes persist,suggesting that WC status may play a crucial role in inferior outcomes.
DlSCUSSlON
RTW guidelines
While the decision to RTW depends on a variety of factors,all physicians have the goal of returning patients to maximal function in the shortest period of time with the least residual disability[69,70]. Based on the available literature,guidelines can be proposed for average time to RTW for each work demand level within each type of shoulder arthroplasty (Table 6). We determined these averages through a pooled analysis[71].

Throughout the rehabilitation process,physicians must assess patients,especially those with WC status,in terms of work restrictions and limitations. Given the little published evidence for guidelines regarding physical restrictions after shoulder arthroplasty,the work restrictions are commonly based on the physician’s clinical judgment[69]. On the other hand,work limitations are easier to define as they are based on the patient’s ability to perform a certain task[69].
Particularly for WC patients who undergo shoulder replacement and rehabilitation and have still failed to RTW at their desired work demand level,work conditioning or work hardening therapy regimens can be prescribed[69,72]. Work conditioning,a task simulation program lasting two to four hours per day for three to five days per week,is meant to develop a patient’s ability to tolerate specific tasks they would typically encounter at work. Work hardening has the same goal in mind with a higher intensity lasting up to eight hours per day for five days per week[69].
The two were also ill-fated in another way. They had not only wedded each other, but they wedded their recessive9 genes10. When her first son, Loren, arrived, Marianne knew something was wrong. He didn t respond to sound. For a year, Marianne struggled and consulted with doctors who told her nothing was wrong.
When recovery from shoulder arthroplasty has reached a therapeutic plateau for either non-WC or WC patients,a physician must rate the residual permanent impairment and individually assess how long each injured patient should remain on this plateau before considering them at maximum medical improvement (MMI)[69]. MMI is established when no further treatment will significantly change the patient’s outcome; at this point,a patient can be recovered completely without any residual impairment or have some permanent impairment[69,73]. Specifically for TSA,Cabarcas[74] established MMI at twelve months postoperatively. While Puzzitiello[75] established MMI for rTSA at twelve months following surgery,Matar[76] found patients undergoing rTSA may reach MMI as early as six months after surgery. If a patient has reached MMI,but has failed to achieve their pre-injury or prior level of work status,then a physician can utilize a functional capacity evaluation to determine the patient’s ability and impose final work restrictions[69]. Although the results of the FCE are often used to set work limitations,some studies have questioned its utility as FCE does not take biopsychosocial factors into account and possibly measures a patient’s tolerance to an activity as opposed to the patient’s true ability[69,77,78].
After MMI has been reached,there are two outcomes:(1) The patient is able to RTW with or without permanent restrictions at the same job; or (2) The patient finds a new job because the employer cannot accommodate the patient’s work limitations[69]. Using evidence-based guidelines to determine MMI for TSA,rTSA,and HA is important not only for counseling patients,but also modifying their expectations prior to surgery.
2. Who lived together in a house of their own: Note that these bears do not live in caves or any place normally associated with bears. From their first moment on the page, these bears are the epitome15 of civilized16, human society. These bears live in a house, the symbol of community, not barbarism.Return to place in story.
Limitations and future research directions
Our narrative systematic review and analysis has several limitations. First,identification and inclusion of references utilized for this review relied on the previously described search strategy in 4 different databases. We searched 4 different databases in order to limit the possibility of overlooking studies related to shoulder arthroplasty and RTW. Second,our data relied on the data reported in the included studies. Therefore,we are limited by the clarity of the results reported as well as the study design and level of evidence. As a result,we utilized the MINORS score to evaluate the quality of the 12 included studies and any potential publication bias. We found that the 12 studies were of acceptable quality and determined no findings suggestive of publication bias. Additionally,our data shows a high level of heterogeneity which may lead to treatment bias effect. Similarly,with regard to work intensity,our study is limited by what was reported and those studies may exclude important nuances that could have led to functional consequences. Furthermore,the heterogeneity of our data is reflective of the reality of clinical practice and often most accurately represents what orthopedic surgeons encounter in the clinical setting[79-81]. Despite these limitations,the findings in our study provide important data that help orthopedic surgeons manage patient expectations about RTW following TSA,rTSA,or HA.
In the future,systematic reviews and analyses regarding shoulder arthroplasty and RTW will hopefully have access to references that are more homogenous with higher levels of evidence. Although the reality that a high level of heterogeneity may be inevitable in the clinical research setting,additional research should be conducted that compares short- and long-term outcomes following TSA,rTSA,and HA and a patients’ ability to RTW. Furthermore,revision arthroplasty and ability to RTW may be a topic worth exploring as the average age of patients undergoing shoulder replacement is decreasing.
CONCLUSlON
The majority of patients are able to RTW following TSA,rTSA,and shoulder HA. The rates of RTW following TSA (71%-93%) seem to be consistently higher than those reported for HA (69%-82%) and rTSA (56%-65%),although this may reflect demographic differences such as age in patient populations. Sedentary,light demand jobs generally have higher rates of RTW than moderate or heavy demand jobs. On average,most patients who underwent TSA,rTSA,or HA were able to RTW at an average duration between 1 mo to 4 mo depending on work demand level. Furthermore,WC status negatively influenced clinical outcomes following shoulder arthroplasty.
The children were supposed to have spent Thanksgiving with their father that year, but because of the flu they were home with me, for a very special Thanksgiving Day. They were feeling better, and we all ate the goodness of the Lord’s bounty9 -- and our community’s love. Our hearts were truly filled with thanks.
ARTlCLE HlGHLlGHTS
Research background
Over the last two decades,the number of shoulder arthroplasties,including total shoulder arthroplasty(TSA),reverse TSA (rTSA),and shoulder hemiarthroplasty (HA),has increased at exponential rates.Due to satisfactory clinical and functional long-term outcomes,the number of shoulder replacements performed will continue to rise into this next decade. Additionally,these procedures are becoming more prevalent in younger and more active populations. With younger individuals who compose a significant amount of the workforce receiving shoulder replacements,patients will begin to place a higher priority on their ability to return to work following shoulder arthroplasty.
Round her were numbers of Church dignitaries, and on either side were standing two rows of tapers31, the largest of them as tall as a steeple, and the smallest as tiny as a Christmas-tree candle
Research motivation
Prior studies have shown varying levels of return to work after shoulder arthroplasty based on arthroplasty type,diagnosis,and work intensity. While informative,a compilation comparing various demographics,arthroplasty types,diagnoses,and work intensities has not been performed in recent years.
Research objectives
The aim of the review article was to summarize return to work outcomes following TSA,rTSA,and HA,and analyze the effects of workers’ compensation status on return to work rates and ability.
Research methods
This systematic review and analysis was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A literature search regarding return to work following shoulder arthroplasty was performed using four databases through January 2021. All studies included in this review were analyzed by at least two authors. Included studies were then evaluated using the Methodological Index for Non-Randomized Studies checklist.
Research results
The majority of patients undergoing TSA,rTSA,or HA were able to return to work between one to four months,depending on work demand stratification. While sedentary or light demand jobs generally have higher rates of return to work,moderate or heavy demand jobs tend to have poorer rates of return.Furthermore,workers’ compensation status negatively influenced clinical outcomes following shoulder arthroplasty. Through a pooled means analysis,we proposed guidelines for the average time to return to work following TSA,rTSA,and HA.
Research conclusions
Cvetanovich[21] analyzed 27 shoulders (24 patients) that underwent anatomic TSA with an inlay glenoid component and stemless ovoid humeral head component. Twenty five (93%) of 27 patients were able to RTW with an average duration of 3.7 mo following surgery. Of the 2 patients who were not able to return,one patient cited reasons unrelated to the shoulder and the other patient cited back issues. When stratified by job intensity preoperatively,the rates of RTW were as follows:5/5 for sedentary,2/2 for light,9/9 for moderate,and 9/11 for heavy. Furthermore,of the 25 patients who returned to work,19 (76%) were able to return to their preoperative occupational demands. The 6 patients who returned to work at a lower intensity held heavy intensity occupations[21]. In addition to corroborating high rates of RTW for patients undergoing TSA,the authors found that patients with heavier demand jobs were less likely to RTW at the same occupational level postoperatively than patients in the other work demand classes.
Research perspectives
Further research and analyses comparing short- and long-term outcomes following TSA,rTSA,and HA and a patients’ ability to return to work would provide tremendous benefit. Additionally,revision arthroplasty and ability to return to work may be a topic worth exploring as the average age of patients undergoing shoulder replacement is decreasing.
All authors made significant contributions toward the preparation of this manuscript. Lalehzarian SP wrote the article,critically revised the article,and participated in the final approval of the version to be published; Agarwalla A critically revised the article and participated in the final approval of the version to be published; Liu JN designed the work,critically revised the article,and was responsible for final approval of the version to be published.
All the authors report no relevant conflicts of interest for this article.
The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Very often they spent the day in hunting together, but after a while the wife found that she had so many things to do that she was obliged to stay at home; so he went alone, though he found that when his wife was not with him he never had any luck
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
United States
But he just smiled and nodded and kept on talking. After a while, I just listened. I liked the sound of his raspy(,) voice filling the warm attic. My mother gave my grandfather a colorful shiny hand fan that he used to keep himself cool during the hot afternoons. My father gave him a small transistor6() radio, which my grandfather listened to late at night, tuned7 to the Korean Gospel station. My mother also gave him a goat-hair brush, rice paper, an ink stick, and an inkstone to practice his calligraphy8(), a special kind of writing.
Simon P Lalehzarian 0000-0003-3406-3651; Avinesh Agarwalla 0000-0001-5056-6780; Joseph N Liu 0000-0002-3801-8885.
The big old monster greedily accepted my dime, and I heard the bottles shift. On tiptoes I reached up and opened the heavy door. There they were: one neat row of thick green bottles, necks staring directly at me, and ice cold from the refrigeration. I held the door open with my shoulder and grabbed one. With a quick yank, I pulled it free from its bondage12. Another one immediately took its place. The bottle was cold in my sweaty hands. I will never forget the feeling of the cool glass on my skin. With two hands, I positioned the bottleneck13 under the heavy brass14 opener that was bolted to the wall. The cap dropped into an old wooden box, and I reached in to retrieve15 it. I was cold and bent16 in the middle, but I knew I needed to have this souvenir. Coke in hand, I proudly marched back out into the early evening dusk. Grampy was waiting patiently. He smiled.
Gao CC
A
Gao CC
杂志排行
World Journal of Orthopedics的其它文章
- Calcium pyrophosphate dihydrate crystals in a 9-year-old with osteomyelitis of the knee:A case report
- Evolution of evidence in spinal surgery – past,present and future Scientometric analysis of randomized controlled trials in spinal surgery
- Fragility of statistically significant findings from randomized clinical trials of surgical treatment of humeral shaft fractures:A systematic review
- Revision anterior cruciate ligament reconstruction:Return to sports at a minimum 5-year follow-up
- Short arm cast is as effective as long arm cast in maintaining distal radius fracture reduction:Results of the SLA-VER noninferiority trial
- Histological difference in ligament flavum between degenerative lumbar canal stenosis and non-stenotic group:A prospective,comparative study