Model established based on blood markers predicts overall survival in patients after radical resection of types II and III adenocarcinoma of the esophagogastric junction
2022-09-01ZhiJianWeiYaTingQiaoBaiChuanZhouAbigailRankineLiXiangZhangYeZhouSuManXuWenXiuHanPanQuanLuo
Zhi-Jian Wei,Ya-Ting Qiao,Bai-Chuan Zhou,Abigail N Rankine,Li-Xiang Zhang,Ye-Zhou Su,A-Man Xu,Wen-Xiu Han,Pan-Quan Luo
Zhi-Jian Wei,Bai-Chuan Zhou,Li-Xiang Zhang,A-Man Xu,Wen-Xiu Han,Pan-Quan Luo,Department of General Surgery,The First Affiliated Hospital of Anhui Medical University,Hefei 230022,Anhui Province,China
Ya-Ting Qiao,Department of Gastrointestinal Surgery,Affiliated Hospital of Hefei University,Hefei 230056,Anhui Province,China
Abigail N Rankine,Department of Clinical Medicine,Anhui Medical University,Hefei 230032,Anhui Province,China
Li-Xiang Zhang,Department of Gastroenterology,Anhui Provincial Key Laboratory of Digestive Disease,The First Affiliated Hospital of Anhui Medical University,Hefei 230022,Anhui Province,China
Ye-Zhou Su,Department of Obstetrics and Gynecology,The First Affiliated Hospital of Anhui Medical University,Hefei 230022,Anhui Province,China
Abstract BACKGROUND In recent years,the incidence of types II and III adenocarcinoma of the esophagogastric junction (AEG) has shown an obvious upward trend worldwide.The prognostic prediction after radical resection of AEG has not been well established.AIM To establish a prognostic model for AEG (types II and III) based on routine markers.METHODS A total of 355 patients who underwent curative AEG at The First Affiliated Hospital of Anhui Medical University from January 2014 to June 2015 were retrospectively included in this study.Univariate and multivariate analyses were performed to identify the independent risk factors.A nomogram was constructed based on Cox proportional hazards models.The new score models was analyzed by C index and calibration curves.The receiver operating characteristic (ROC) curve was used to compare the predictive accuracy of the scoring system and tumor-node-metastasis (TNM) stage.Overall survival was calculated using the Kaplan-Meier curve amongst different risk AEG patients.RESULTS Multivariate analysis showed that TNM stage (hazard ratio [HR] = 2.286,P = 0.008),neutrophil-tolymphocyte ratio (HR = 2.979,P = 0.001),and body mass index (HR = 0.626,P = 0.026) were independent prognostic factors.The new scoring system had a higher concordance index (0.697),and the calibration curves of the nomogram were reliable.The area under the ROC curve of the new score model (3-year: 0.725,95% confidence interval [CI]: 0.676-0.777;5-year: 0.758,95%CI:0.708-0.807) was larger than that of TNM staging (3-year: 0.630,95%CI: 0.585-0.684;5-year: 0.665,95%CI: 0.616-0.715).CONCLUSION Based on the serum markers and other clinical indicators,we have developed a precise model to predict the prognosis of patients with AEG (types II and III).The new prognostic nomogram could effectively enhance the predictive value of the TNM staging system.This scoring system can be advantageous and helpful for surgeons and patients.
Key Words: Adenocarcinomas of the esophagogastric junction;Neutrophil-to-lymphocyte ratio;Platelet-tolymphocyte ratio;Prognosis;Tumor-node-metastasis
lNTRODUCTlON
Adenocarcinomas of the esophagogastric junction (AEG),which are located within 5 cm of the esophagogastric junction,are classified into three subgroups: Types I,II,and III.Type I AEG (adenocarcinoma of the distal esophagus) is most prevalent in Western countries;types II and III AEG are more prevalent than type I in Asia and are mostly treated as gastric cancer[1,2].The incidence rate of AEG has significantly increased over the past two decades and is increasing more rapidly than any other type of neoplasm[3,4].
Surgery is considered the only curative treatment for patients with AEG;however,the survival rate is not good even with surgery[5].
At present,many studies are exploring non-invasive and sensitive biomarkers that can accurately predict the prognosis of patients with AEG.Among these,carcinoembryonic antigen (CEA) has been used for the early diagnosis of cancer[6].Cancer-related systemic inflammatory responses,such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR),play an important role in the progression and outcome of tumors[7,8].Patients with a high NLR have a poor prognosis[9].Malnutrition is also related with the prognosis of patients;however,few studies have assessed the predictive value of inflammatory,nutritional,and blood tumor markers for overall survival (OS) in patients with AEG (types II and III)[10].This research established a nomogram to explore the value of blood markers.
MATERlALS AND METHODS
We collected blood and clinical data of patients with AEG (types II and III) who were hospitalized at the First Affiliated Hospital of Anhui Medical University between January 2014 and June 2015.Patients were analyzed retrospectively according to the inclusion and exclusion criteria.The inclusion criteria were as follows: (1) Patients confirmed with AEG (types II and III) by pathological diagnosis;(2) Radical resection of the tumor;(3) Absence of heart diseases or organ failure;and (4) Peripheral blood test results obtained within 1 wk before surgery.The exclusion criteria were as follows: (1) Previously untreated malignancy;(2) Previously accepted radiation treatment or chemotherapy before the treatment;(3) Presence of certain diseases,such as infection,which could influence the peripheral blood cell counts;(4) Patients who died within 30 d after surgery because of sudden accidents,such as pulmonary embolism;and (5) Patients with incomplete data.In accordance with the inclusion criteria,440 patients with AEG were included in the study.Finally,a cohort of 355 patients was analyzed based on the exclusion criteria.The patient admission process is shown in Supplementary Figure 1.This study was conducted conforming to the TRIPOD guidelines.This study included 355 patients and the testing group,including 120 patients,who were hospitalized at the First Affiliated Hospital of Anhui Medical University between January 2018 and June 2018.
Data on patients’ demographic and clinicopathological features were gathered from the medical records of our hospital,including age,gender,body mass index (BMI),tumor size,differentiation grade,tumor-node-metastasis (TNM) stage,tumor location,surgery time,cancerous node,smoking,and comorbidities.The pathological tumor stage was categorized according to the 7thedition of the American Joint Committee on Cancer TNM staging system.The routine laboratory data evaluated were as follows: Neutrophil,lymphocyte,and platelet counts;prealbumin,albumin,hemoglobin,CEA,CA199,and fibrinogen levels.
Peripheral blood tests were performed within 1 wk before surgery,and the following indices were determined: NLR,PLR,and prognostic nutritional index (PNI).The NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count,and the PLR was calculated by dividing the absolute platelet count by the absolute lymphocyte count.The PNI was calculated as serum albumin (g/L) + 5 × total lymphocyte count (109/L)[11].The NLR,PLR,and PNI were grouped into low and high groups according to the Youden index (maximum [sensitivity + specificity-1])[12].The BMI (kg/m2) was divided into the following three groups: < 18.5 (low group),18.5-24.9 (normal group),and ≥ 25 (high group).The CEA,CA199,albumin and prealbumin levels were grouped based on their normal values.
All patients with Siewert type II/III AEG underwent radical surgery with celiac and mediastinal lymphadenectomy.All the patients underwent radical D2 lymphadenectomy.They received four to six cycles of first-line adjuvant combination chemotherapy after surgery with oxaliplatin plus 5-fluorouracil/leucovorin or a prodrug of 5-fluorouracil (capecitabine;CapeOX).
Statistical analysis
Multivariate and univariate survival analyses were performed using the Cox proportional hazard pattern.Harrell’s concordance index (C-index) was used in the nomogram to evaluate the model performance for the prognosis of patients with AEG.Calibration and receiver operating characteristic (ROC) curves were used to verify the accuracy of the new scoring system.Survival analysis was compared using Kaplan-Meier method,and the nomogram was constructed using the R package “rms,” “Hmisc,” “lattice,” “Formula,” and “foreign.” The data are presented using the Statistical Package for the Social Sciences software (16.0 version) and RStudio software (version 1.1.447- 2009-2018;RStudio,Inc.).APvalue < 0.05 was considered statistically significant.
RESULTS
The baseline characteristics of 355 patients are presented in Table 1.Overall,281 (79.1%) male and 74 (20.9%) female patients were included.The median age of the patients was 65 years (range,29-85 years).The median follow-up period was 52 mo (range,1.5-72 mo).
Table 2 shows the results of univariate risk factors.Age,prealbumin,TNM stage,tumor size,histological type,CEA,PNI,PLR,NLR,BMI,hemoglobin,and cancerous nodes were significant indicators.The variables with aPvalue < 0.05,as determined by the univariate analysis,were included in the multivariate analysis.Among them,TNM stage (hazard ratio [HR] = 2.286,P =0.008),NLR (HR = 2.979,P =0.001),and BMI (HR = 0.626,P =0.026) were independent prognostic factors (Table 3).
A model was constructed to predict OS of AEG patients based on the Cox analysis (Figure 1).Each subgroup variable was assigned a score.A scoring system was used to assign a score to each variable (Table 4).To apply the nomogram,a vertical line was delineated to indicate the row to assign point values for each variable.Subsequently,the corresponding scores were summed to obtain the total score.Finally,a vertical line from the total point was drawn to obtain the 3-year and 5-year survival probability.

Table 1 Characteristics of the recruited patients

Table 2 Univariate analysis of adenocarcinoma of the esophagogastric junction (types II and III) patients

Table 3 Multivariate analysis of adenocarcinoma of the esophagogastric junction (types II and III) patients

Table 4 Nomogram scoring system
Calibration curves were used to verify the performance of the model in predicting OS of patients with AEG (Figures 2 and 3),and the results showed that the actual OS curve of the nomogram fits the predicted OS curve.Besides,the calibration curve in the testing group for 3-year OS was also good (Figure 4),and the C-index of the model was 0.697 (95% confidence interval [CI]: 0.660-0.734),indicating that this model was reliable.Besides,the area under the ROC curve (AUC) of the new score model (3-year: 0.725,95%CI:0.676-0.777;5-year: 0.758,95%CI:0.708-0.807) was larger than that of the TNM stage (3-year: 0.630,95%CI: 0.585-0.684;5-year: 0.665,95%CI: 0.616-0.715) (Figures 5 and 6),which indicated that the constructed nomogram was a reliable scoring system.
In addition,we divided the patients into two groups according to the total nomogram score (low-risk: < 58 and high-risk: ≥ 58) (Figure 7).The results showed that high-risk patients with AEG had a poor prognosis.The Kaplan-Meier curves indicated that the nomogram had excellent results in predicting survival.

Figure 1 Nomogram for predicting overall survival after curative resection of gastric cancer.

Figure 2 Calibration curves of the prognostic nomogram for 3-year overall survival.

Figure 3 Calibration curves of the prognostic nomogram for 5-year overall survival.
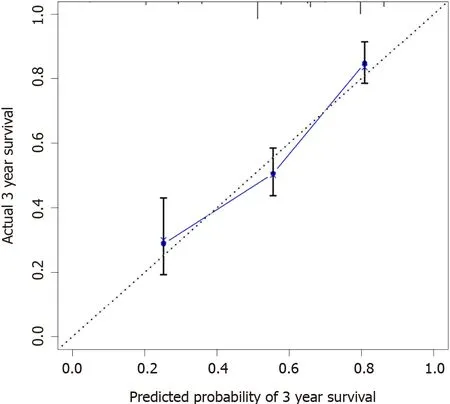
Figure 4 Calibration curves in the testing group for 3-year overall survival.

Figure 5 The receiver operating characteristic curves of the prognostic nomogram and tumor-node-metastasis staging for 3-year overall survival.

Figure 6 The receiver operating characteristic curves of the prognostic nomogram and tumor-node-metastasis staging for 5-year overall survival.

Figure 7 Survival curves stratified by the score calculated by the nomogram (low risk: <58 and high risk: ≥ 58).
DlSCUSSlON
Early detection of AEG is often difficult,owning to the limitations of diagnostic techniques,resulting in a poor prognosis.At present,the 5-year survival rate of patients with AEG is less than 30%[13].The
epidemiology,genetics,spread pattern,and prognosis of neoplasms in the esophagus,esophagogastric junction,and stomach remain unclear.The process of tumor development is complex.Gastroesophageal reflux disease andHelicobacter pylorihave been reported as risk factors for AEG[14,15].Therefore,many researchers have made significant contributions to improve the prognosis of AEG.Lymph node metastasis,tumor size,differentiation grade,and TNM stage have been defined as prognostic factors[16,17].However,these prognostic factors are difficult to judge before surgery;therefore,research on prognostic serum markers has been widely conducted in recent years.To the best of our knowledge,this study is the first attempt to develop a prognostic nomogram that combines serum markers (including inflammatory markers,nutritional indices,and tumor markers) and clinicopathological characteristics to estimate the 3-year and 5-year survival probability,which was highly accurate in predicting the prognosis of patients with AEG (types II and III).
The multivariate analysis revealed that TNM stage,NLR,and BMI were important factors.Therefore,a model was built by these markers.Moreover,the calibration and ROC curves showed that the nomogram was reliable and precise.
In recent years,nomogram has been used to predict the prognosis of many cancers[18,19].This model has been identified as a new standard that can integrate multiple predictive variables in a weighted manner and intuitively show the influence of variables on individual predictive values.Similar conclusions were obtained in the present study.The AUC of the nomogram was larger than that of TNM stage;therefore,the nomogram and TNM staging system can help in predicting the survival of patients with AEG.Furthermore,this nomogram can be applied in clinical practice to help surgeons evaluate the prognosis of patients and choose appropriate treatment.
Our nomogram contained three variables,and previous studies also got to the same conclusion[9,20].Inflammatory indexes were related with the prognosis of gastrointestinal cancer patients[21].This research found that NLR was an independent risk factor,and the possible mechanism is that systemic inflammation caused by tumors can release a large number of pro-inflammatory mediators,such as Creactive protein,fibrinogen,vascular endothelial growth factor,and transforming growth factor-α.These factors stimulate the process of tumors[22].Meanwhile,neutrophils could prevent natural killer cells and T cells in the system contacting and killing the tumor cells[23,24].Therefore,the NLR should be included in the regular assessment index for patients with AEG.
As an independent prognostic indicator of tumor-related diseases,BMI has raised increasing concerns for researchers in recent years.BMI is related to the prognosis of breast carcinoma,non-small-cell lung cancer,and colorectal cancer,among others[25-27].In this study,we found that BMI was significantly correlated with the prognosis of patients with AEG.However,the underlying mechanism remains unclear.Patients with AEG with a low BMI may have poor nutritional status and immune function[28].This may have an adverse effect on disease progression;therefore,these patients may have a shorter OS.
Our research has two potential limitations.First,this study was a single-center study that did not include a sufficient number of cases to verify the results.Second,the included patients who underwent surgical resection for AEG cannot account for all patients with AEG.
CONCLUSlON
TNM stage,NLR,and BMI are risk factors for the prognosis of patients with AEG.The novel nomogram accurately and reliably predicts the OS after radical resection of patients with AEG (types II and III).This may help clinicians formulate personalized treatment plans.
ARTlCLE HlGHLlGHTS
Research background
In recent years,the incidence of types II and III adenocarcinoma of the esophagogastric junction (AEG)has shown an obvious upward trend worldwide.
Research motivation
The prognostic prediction after radical resection of AEG has not been well established.
Research objectives
To establish a prognostic model for AEG (types II and III) based on routine markers.
Research methods
The construction of the nomog ram was based on Cox proportional-hazards models.The new score model was analyzed by C index and calibration curves.The receiver operating characteristic (ROC)curve was used to compare the predictive accuracy of the scoring system and tumor-node-metastasis(TNM) staging.Overall survival (OS) was calculated using the Kaplan-Meier curve amongst different risk AEG patients.
Research results
Multivariate analysis showed that TNM stage (hazard ratio [HR] = 2.286,P = 0.008),neutrophil-tolymphocyte ratio (NLR) (HR = 2.979,P = 0.001),and body mass index (BMI) (HR = 0.626,P = 0.026)were independent prognostic factors.The new scoring system had a higher concordance index (0.697),and the calibration curves of the nomogram were reliable.The area under the ROC curve of the new score model (3-year: 0.725,95% confidence interval [CI]: 0.676-0.777;5-year: 0.758,95%CI: 0.708-0.807)was larger than that of TNM staging (3-year: 0.630,95%CI: 0.585-0.684;5-year: 0.665,95%CI: 0.616-0.715).
Research conclusions
This model has been identified as a new standard that can integrate multiple predictive variables in a weighted manner and intuitively show the influence of variables on individual predictive values.To the best of our knowledge,this study is the first attempt to develop a prognostic nomogram that combines serum markers (including inflammatory markers,nutritional indices,and tumor markers) and clinicopathological characteristics to estimate the 3-year and 5-year survival probability,which is highly accurate in predicting the prognosis of patients with AEG (types II and III).TNM stage,NLR,and BMI were risk factors for the prognosis of patients with AEG and then a model was built which can predict the prognosis of patients.
Research perspectives
The novel nomogram accurately and reliably predicts the OS after radical resection of patients with AEG (types II and III).This may help clinicians formulate personalized treatment plans.
FOOTNOTES
Author contributions:Wei ZJ and Qiao YT designed this study and drafted the manuscript,and they contributed to this work equally;Zhou BC collected and organized the data;Abigail NR polished the article;Zhang LX,Su YZ,Xu AM,Han WX,and Luo PQ performed the study and participated in the work;Zhang LX,Su YZ,Xu AM,Han WX,and Luo PQ contributed this work equally,and they are all the corresponding author.All authors read and approved the final manuscript.
Supported bythe Natural Science Foundation of Anhui Province,No.2108085QH337.
lnstitutional review board statement:This study was approved by the First Affiliated Hospital of Anhui Medical University.
Conflict-of-interest statement:Patients were not required to give informed consent to the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Zhi-Jian Wei 0000-0003-1094-1894;Bai-Chuan Zhou 0000-0002-6288-1400;Abigail N Rankine 0000-0001-6641-9910;Pan-Quan Luo 0000-0002-2828-7061.
S-Editor:Wang LL
L-Editor:Wang TQ
P-Editor:Wu RR
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Percutaneous direct endoscopic pancreatic necrosectomy
- Factors associated with hypertension remission after gastrectomy for gastric cancer patients
- 3D laparoscopic-assisted vs open gastrectomy for carcinoma in the remnant stomach:A retrospective cohort study
- Pre-colonoscopy special guidance and education on intestinal cleaning and examination in older adult patients with constipation
- Over-the-scope-grasper: A new tool for pancreatic necrosectomy and beyond - first multicenter experience
- ldentifying survival protective factors for chronic dialysis patients with surgically confirmed acute mesenteric ischemia