Impact of different waves of COVID-19 on emergency medical services and out-of-hospital cardiopulmonary arrest in Madrid,Spain
2022-09-01JoseMarNavalpotroPascualDianaMongeMartManuelJosGonzlezLeFernandoNeriaSerranoCarlosAlonsoBlasBelMuozIsabelYagoMuecasCuestaAlfredoCarrilloMoyaJuanLesGonzlezAlonsoMateosRodrguez
Jose-María Navalpotro-Pascual ,Diana Monge Martín ,Manuel-José González León ,Fernando Neria Serrano ,Carlos Alonso Blas ,Belén Muñoz Isabel ,Yago Muñecas Cuesta,Alfredo Carrillo Moya,Juan Les González,Alonso Mateos Rodríguez,
1 Madrid Emergency Medical Services,SUMMA 112,Madrid 28045,Spain
2 School of Medicine,Francisco de Vitoria University,Madrid 28223,Spain (School of Medicine,Universidad Francisco de Vitoria,Madrid 28223,Spain)
Out-of-hospital cardiac arrest (OHCA) is one of the three leading causes of death in industrialized countries.Some studies have described the impact of the first COVID-19 pandemic wave in terms of the number of cases and OHCA survival rates in various regions,but few have addressed the relationship between the successive phases and how they affected OHCA.The 14-d cumulative incidence peaked at more than 990 cases,with these rates remaining above 200 for an eight-month period between 15 March 2020 and 15 March 2021 in Madrid,Spain.
The objectives of the current study were twofold.First,we sought to describe how the different waves in the first pandemic year affected the healthcare activity of the Spanish emergency medical services (EMS).Second,we compared effects of the pandemic year on OHCA care to those of the preceding non-pandemic year in terms of initiating cardiopulmonary resuscitation and survival in a community with a high incidence of COVID-19.
METHODS
This was a retrospective study based on a continuous OHCA registry of the EMS Servicio de Urgencia Médica de la Comunidad de Madrid (SUMMA 112) in Spain.The registry collected all variables according to the definitions of the Utstein style,and neurological status was defined according to the Cerebral Performance Categories scale.
The study period was from 15 March 2019 to 14 March 2021.The data were divided into a non-pandemic period (NPP) from 15 March 2019 to 14 March 2020 and a pandemic period (PP) from 15 March 2020 to 14 March 2021.The PP was further divided into four sub-periods according to the 14-d cumulative incidence.All patients with OHCA who were treated with SUMMA 112 during the study period were included in our analysis.
Patients were categorized into one of the abovedescribed periods according to the date of their OHCA onset.
Quantitative data are described using medians and interquartile ranges (IQRs),and qualitative data are described with number and percentage values.Comparative analyses were performed using Pearson’s Chi-square test or Fisher’s exact test for qualitative variables and the Wilcoxon test for quantitative variables.Differences were considered statistically significant when the-value was less than 0.05.All statistical analyses were performed using R software v 4.1.
RESULTS
General characteristics of patients in the NPP and PP
During the PP,there were 1,743 patients with OHCA,compared with 1,781 patients during the NPP.The general characteristics of the patients included in both periods were shown in Table 1.
Compared with NPP,more OHCAs occurred at home during the PP (79.0% vs.84.5%;<0.001).There were no significant differences in the percentage of witnessed cardiac arrests (1,443 [81.0%] during NPP vs.1,418 [81.5%]during PP;=0.693) or resuscitation attempts prior to EMS arrival (708 [39.8%] during NPP vs.693 [39.8%] during PP;=0.997).
Compared with NPP,the percentage of advanced life support (ALS) attempts compared to the total number of OHCAs attended was lower during PP (62.9% during NPP vs.59.4% during PP;=0.034),although the percentage of shockable rhythms did not differ significantly (167 [15.0%]vs.155 [15.1%];=0.946).
Survival on arrival at the hospital decreased significantly during the PP (387 [34.6%] during NPP vs.313 [30.3%] during PP;=0.037).When analyzing the status of patients at hospital arrival,the percentage who arrived with recovery of spontaneous circulation (ROSC)decreased during the pandemic (348 [31.1%] during NPP vs.262 [25.4%] during PP).
General characteristics of patients in the different waves
The influence of different waves of the pandemic (three waves and one plateau period after the first wave) on OHCA care was shown in Table 2.

Table 1. General characteristics of patients included in the NPP and PP
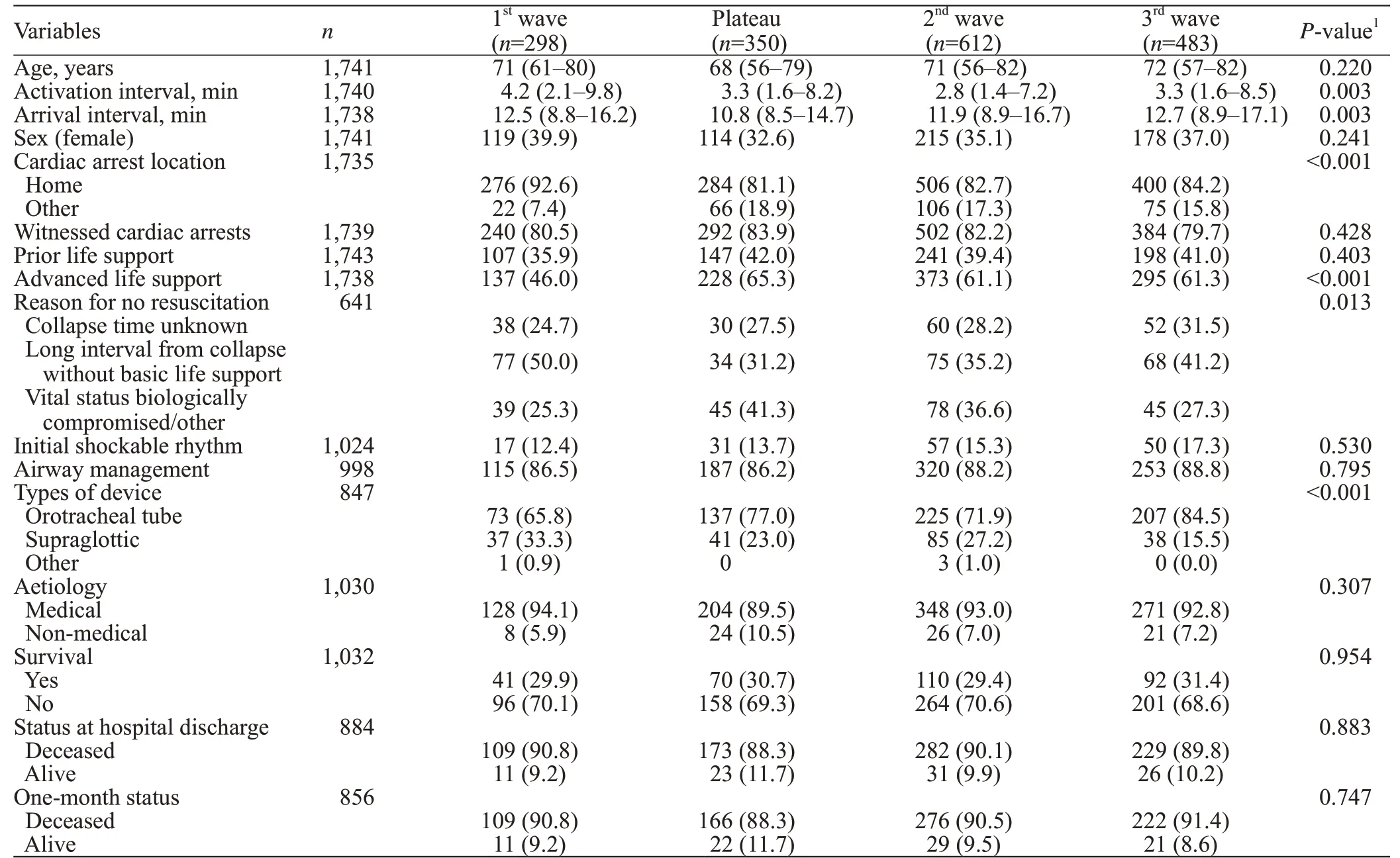
Table 2. General characteristics of patients included in the different waves
During the first wave,the proportion of resuscitation attempts was significantly lower than that during the other waves: 46.0% during the first wave vs.65.3% during the plateau,61.1% during the second wave,and 61.3% during the third wave (<0.001).There was no significant difference when comparing the percentage of shockable rhythms(=0.530) or whether the airway was managed (=0.795).Significant differences were found when comparing the type of airway management,with supraglottic airway devices used more in the first wave (33.3%) compared to the plateau period (23.0%) and the second (27.2%) and third waves(15.5%;<0.001),respectively.
In all three waves,there was a significant increase in the number of calls received at the dispatch centre compared to the NPP.Most calls were notably during the first wave.This work overload was assumed in the dispatch centre itself without increasing the mobilization of resources for face-toface patient care (supplementary Figure 1).
DISCUSSION
The resuscitation attempt rates decreased significantly during the first pandemic wave,as reported in other studies,but we also found that they recovered to non-pandemic levels during the remainder of the PP.The greatest pressure and work overload were experienced in the dispatch center,with a very significant increase in the number of calls without significant changes in the mobilization of resources.
The most common reason for non-resuscitation was the longer interval time in arrival of the EMS.During the PP,the aetiology of OHCA was most frequently medical,as other researchers have reported.
We found no significant differences in whether the airway was managed,but our study and other studies have indicated that supraglottic airway management devices were more commonly used during the PP,a pattern that changed over time.
OHCA survival at hospital admission was significantly reduced,as previously described in other studies.One prediction might have been that as the first wave ended and COVID-19 incidence fell,the survival rate would have improved;however,it remained low,with no significant changes during the successive waves.
When comparing survival at the time of hospital discharge and comparing one-month survival rates,we found no significant differences between the NPP and PP,but there was a trend towards worse survival during the pandemic.We also found no significant differences in these outcomes among the different periods of the pandemic.
The results of this study highlight the influence that COVID-19 has had on OHCA and on EMS activity,showing how the pandemic has increased stress on the Emergency Coordination Centre in terms of attending the population.In the community of Madrid,as in Nantesand Lausanne,the number of calls increased during the first pandemic wave,whereas some studies in other regions showed that the number of calls actually decreased.In Madrid,the increased number of EMS calls continued through successive waves,and this overload led to a delay in activation time for available resources throughout the PP.In some regions where the calls decreased,activations often decreased as well.In other places,however,despite an increased number of calls,resource dispatches decreasedor remained the same,as in Madrid,with a similar pattern occurring during subsequent waves.One possible inference is that at the time of high call volume,the various call handling systems significantly influenced how both resource dispatch and response time were handled,as Penverne et aldemonstrated.
CONCLUSIONS
The different waves of the pandemic variably affected OHCA care.Survival from OHCA has decreased since the onset of the pandemic and has not recovered since then.The number of calls to EMS increases as artificial intelligence increases,although the number of mobilizations does not.
None.
The OHSCAR registry has been approved by ethics committees in Northwestern Malaga,Aragon,Cáceres,Navarra,and the Basque Country.
The authors declare that they have no competing interests.
JMNP and DMM designed the study.JMNP,AMR,and CAB coordinated the study and verified the data.DMM and FNS performed and supervised the statistical analysis.MJGL and BMI participated in the literature search.FNS and MJGL participated in data analysis and table and figure design.JMNP,MJGL,BMI,ACM,YMC,and JLG contributed to the development of the study and the data collection.All authors critically reviewed and approved the final version.All authors had full access to all study data and took the ultimate responsibility for the decision to submit this paper for publication.
All the supplementary files in this paper are available at http://wjem.com.cn.