Association between tourniquet use and intraoperative blood loss during below-knee amputation
2022-07-30AldenWylandErikWoelberLiamWongJordanArakawaZacharyWorkingJamesMeeker
INTRODUCTION
Since its 2century introduction to amputation surgery by Heliodorus,the tourniquet has been nearly as enduring as the knife itself[1,2].Yet despite the amputation of over 150000 Lower limbs annually in the United States,there are wide variations in tourniquet practice patterns and no consensus on their necessity during limb removal[3].
Not far from the shore Prince Milan noticed thirty little white garments lying on the grass, and dismounting from his horse, he crept down under the high bulrushes, took one of the garments and hid himself with it behind the bushes which grew round the lake
Tourniquet application during limb amputation is controversial.Historically,the high rate of mortality associated with early amputations was attributed to both delayed septicemia and immediate blood loss,leading surgeons such as Esmarch,Lister,and Cushing to improve upon early designs during the 19and 20centuries[2].Today,tourniquet use is associated with decreased intraoperative blood loss and fewer transfusions in below knee amputations performed primarily in vascular surgery settings[4,5].However,this has hardly settled the question of whether they should be used routinely for hemorrhage control during orthopedic limb removal.Throughout the dissection,use of a tourniquet may provide a drier surgical field by slowing intraoperative bleeding,but at the same time may limit the palpation of neurovascular structures[6-8].Additionally,blood loss continues beyond the intraoperative period,and application of a tourniquet may prevent the surgeon from identifying damage to small vessels that continue to ooze postoperatively.There is also a theoretical risk of damaging fragile atherosclerotic vessels as pneumatic pressure increases,leading to swelling and blood loss in the perioperative period after the tourniquet has been removed[9].This may explain studies finding no difference in total blood loss or transfusions with tourniquet use in studies of both below knee amputation and total knee arthroplasty[9-12].
There is a paucity of literature describing the association between tourniquet use and blood loss during below knee amputation in orthopedic populations,which include patients undergoing surgery for neoplastic disease,trauma,and infection[11].Furthermore,blood loss in prior studies has typically been recorded using surgeon estimation,which is subjective,imprecise,and does not account for perioperative “hidden” blood loss that continues after closure of the wound[10,13,14].
All statistical analysis was performed using R version 3.6.3 including the packages tableone,dplyr,ggplot2,and chest.Statistical significance was determined at 0.05.The study was reviewed by our statistician Dr.Erik Woelber.
MATERIALS AND METHODS
With Institutional Review of Board approval,we retrospectively reviewed consecutive patients undergoing below knee amputation by orthopedic surgeons at a single academic institution over a tenyear period from January 1,2008 to December 31,2018.The hospital is a tertiary referral center for soft tissue sarcomas and a Level 1 trauma center.This study was conducted following STROBE guidelines[15].
I am not surprised, she said to herself, that this wicked man, who intends to kill my master, will eat no salt with him; but I will hinder his plans
Patients were identified by CPT code for below-knee amputation.To prevent confounding by other sources of bleeding,patients were excluded if the indication for below-knee amputation was a trauma that had occurred within one week,if they had active gastrointestinal bleeding,or if they had a diagnosed bleeding disorder.We excluded patients with through-knee amputations.
Data for identified patients was collected from chart review including demographic characteristics (age,sex),known or potential modifiers of blood loss (kidney dysfunction,platelet count),and surgical data (indication for surgery,intraoperative transfusions).A full list of variables that were collected can be found in Supplementary Table 1.Tourniquet use and tourniquet time were taken from surgeon operative reports.Post-operative hemoglobin and hematocrit results were taken within 72 h of the operation.We used the first post-operative hemoglobin in blood loss calculations.

Blood loss was determined using a series of calculations.Preoperative blood volume was calculated using patient height,weight,and gender by the Nadler formula[16]:
Blood volume (Male) = 0.3669 × H+ 0.03219 × W + 0.6041.
Blood volume (Female) = 0.3561 × H+ 0.03308 × W + 0.1833.
Total blood loss was then determined using calculated blood volume,change in hemoglobin concentration,and the mass of hemoglobin transfused intraoperatively,based on modification of the formula by Wied[10]: Total mass of Hgb lost = Blood volume (L) × (Hgb preop - Hgb postop) × 10 + mass of transfused Hgb.Where mass of transfused Hgb = 61.25g × intraoperative units transfused[16].Blood loss (L)= total mass of Hgb lost/ (Hgb preop × 10).
We excluded five variables with > 5% data missingness (functional capacity,erythrocyte sedimentation rate,C-reactive protein,A1c,and albumin).The only remaining variable with missing data (creatinine,2%) was included in regression analysis.Characteristics of patients undergoing below knee amputation with and without tourniquet were compared using t tests or chi square tests as appropriate.
For our primary outcome,we performed a univariate linear regression to determine the association between tourniquet use and blood loss.We also ran subgroup analyses by indication for surgery,using a Wilcoxon due to the non-parametric distribution of blood loss and the low number of observations in each subgroup.We then performed a forward stepwise regression with potential modifiers of the association between tourniquet use and blood loss,sequentially retaining variables that changed the estimation of the association by greater than 10 percent.We excluded the surgeon as a variable from this analysis as it was thought to lie on a causal pathway between indication and blood loss and was not generalizable.We also excluded operative time due to the directionality of its association with tourniquet use and because it likely lies along the causal pathway between tourniquet use and blood loss[11].To avoid spurious associations,we only included variables that were logically associated tourniquet use and blood loss,and limited the variables tested to 10% of the number of observations.We included interaction terms for variables of interest.
We then performed two logistic regressions in a similar fashion using postoperative transfusion and reoperation in one year as outcomes.Postoperative transfusions were only included if administered during the immediate inpatient stay.Reoperations included stump revisions,revision to a higher-level amputation (above-the-knee),and irrigation and debridement.
The primary purpose of this study was to determine whether tourniquet use in orthopedic patients undergoing below knee amputation was associated with a difference in calculated blood loss relative to no tourniquet use.Secondarily,we assessed whether tourniquet application was associated with postoperative transfusions during the inpatient stay or reoperation within one year.We hypothesized that tourniquet use would not be associated with decreased blood loss,postoperative transfusions,or reoperation within one year.
RESULTS
She peeped out from among the green rushes, and if the wind caught her long silvery-white veil, those who saw it believed it to be a swan, spreading out its wings
But one day, as the brothers were as usual doing the honours to their guests, an old man turned to them and said, Yes, it is all most beautiful, but there is still something it needs! And what may that be? A pitcher3 of the water of life, a branch of the tree the smell of whose flowers gives eternal beauty, and the talking bird
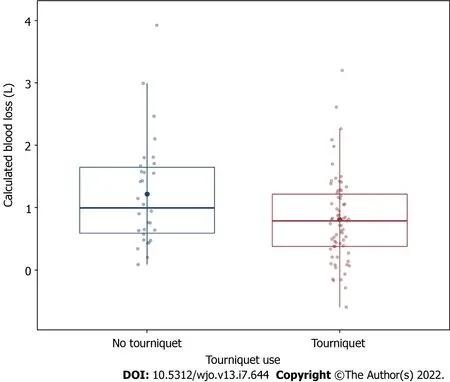
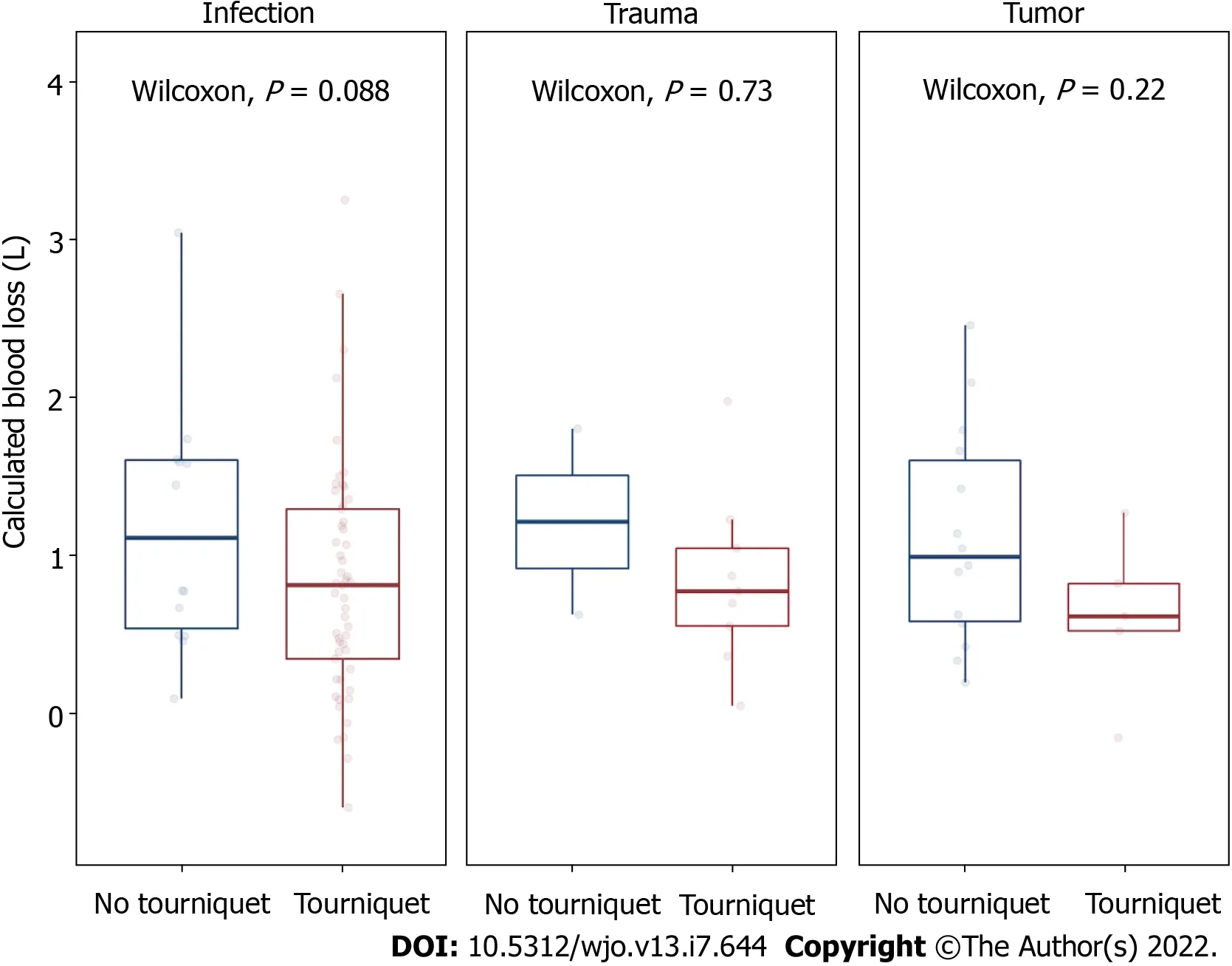
In simple linear regression,tourniquet use was associated with significantly decreased blood loss (-0.41 Liters,SE 0.17,= 0.01) (Figure 1).The calculation allowed for negative blood loss values to occur for 6 patients (6%).The plots reveal a right-skewed distribution of calculated blood loss for both tourniquet and non-tourniquet patients.In the analysis of restricted subgroups,no individual group showed a statistically significant decrease in blood loss with tourniquet use (Figure 2).
Another limitation is that in the patients with an infectious etiology,which was primarily due to diabetes,the presence of peripheral vascular disease was not taken into account,which could affect blood loss.
Thirteen patients in the tourniquet group (19%) and six patients in the non-tourniquet group (20%) received a postoperative transfusion.Twenty patients in the tourniquet group (30%) and 13 patients in the non-tourniquet group (43%) underwent an unplanned reoperation within one year of the index surgery.Adjusted secondary analyses showed no statistically significant association between tourniquet use and either inpatient blood transfusion after the first postoperative lab draw (OR 0.83,CI 0.25-2.72,= 0.75) or reoperation at one year (OR 0.84,CI 0.26-2.79,= 0.78).
We performed a retrospective cohort study on consecutive patients who underwent BKA over a tenyear period at a tertiary care hospital.Blood loss was estimated using the Nadler equation for preoperative blood volume and a novel formula that utilizes preoperative and postoperative hemoglobin levels and transfusions.Univariate and forwards stepwise multivariate linear regression were utilized to determine an association between tourniquet use and blood loss.
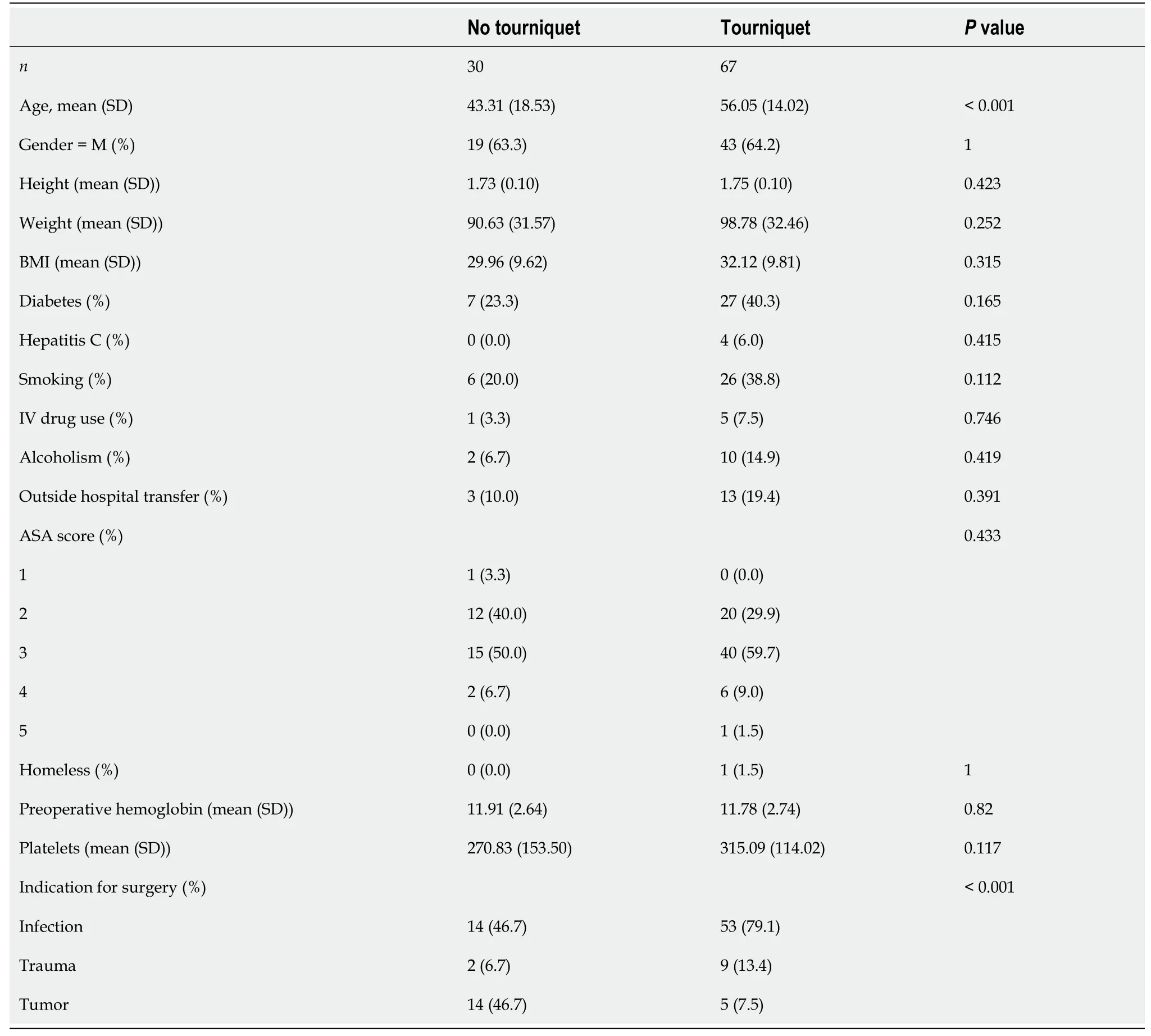
138 patients undergoing below knee amputation were identified by chart review.41 patients were excluded because they sustained a trauma within the prior week,leaving 97 patients for analysis.Of the patients identified,67 underwent surgery with a tourniquet and 30 did not.Indications included infection (69%,= 67),trauma (11%,= 11),and tumor (20%,= 19).Demographic characteristics are shown in Table 1.The tourniquet group was older (5643 years,0.001) and had categorical differences in indication for surgery (0.001).
DISCUSSION
Our results indicate that tourniquet use during below knee amputations performed on orthopedic surgery patients is associated with significantly decreased surgical blood loss.The magnitude of the as sociation is noteworthy,as a 488 mL decrease with use of a tourniquet equates to an approximately ten percent difference in total blood volume lost.
By the beard of the Prophet I never saw such a thing in all my life! My very humble31 thanks, replied the Grand Vizier, as he bent his long neck; but, if I may venture to say so, your Highness is even handsomer as a stork than as a Caliph
Our findings are consistent with the results of prior studies in non-orthopedic populations.A nonrandomized study found that tourniquet use in vascular patients undergoing below-knee amputation is associated with decreased surgical blood loss,fewer postoperative transfusions,and fewer complications[4].Similarly,a prospective,randomized,blinded study found that tourniquet use in peripheral arterial disease patients is associated with less intraoperative blood loss,a smaller perioperative drop in hemoglobin,fewer transfusions,and similar complication rates[5].
In great haste the old man sprang from his bed, and covered the flower with the cloth the old witch had given him, and in a moment the beautiful Princess Hyacinthia stood before him
Our secondary analysis did not demonstrate a statistically significant association between tourniquet use and inpatient postoperative transfusions.A prior study found that as much blood is lost following above-knee amputations postoperatively as during the procedure,which could explain this result[10].Another study echoed the finding that tourniquet use during BKA is associated with less intraoperative blood loss,but no difference in total blood loss (including the postoperative period)[11].In the joint arthroplasty literature,tourniquet use is not associated with a difference in transfusions or total blood loss[12].In our study,it is also possible that we did not have adequate power to detect a difference in transfusions due to their rarity.
Bettelheim states: Starvation anxiety has driven him [Hansel] back, so now he can think only of food as offering a solution to the problem of finding his way out of a serious predicament (Bettelheim 1976). Unfortunately, Hansel appears to have forgotten that birds will eat bread crumbs and destroy his trail. Return to place in story.
Our secondary analysis also did not demonstrate a statistically significant association between tourniquet use and reoperations at one year.At least one study comparing reoperation rates with and without a tourniquet found no difference in the rate of conversion to a higher-level amputation at 30 days[11].
Then she went on her way till she came to the common, where she sat down and began to comb out her hair; then Curdken ran up to her and wanted to grasp some of the hair from her head, but she called out hastily: Wind, wind, gently sway, Blow Curdken s hat away; Let him chase o er field and wold Till my locks of ruddy gold, Now astray and hanging down, Be combed and plaited in a crown
So the girl seated herself on the horse, and rode a wearisome long way onward14 again, and after a very long time she came to a great mountain, where an aged woman was sitting, spinning at a golden spinning-wheel
This study had multiple limitations.First,the calculation of intraoperative blood loss relies on several assumptions: It assumes that all patients are adequately resuscitated following their operation at the time of their first postoperative blood draw (and thus may have underestimated total blood loss),and it does not account for changes in intravascular volume cause by vasoconstriction or fluid shifts.The calculation also does not account for any blood volume in the amputated limb.In theory,the equation overestimates blood loss because it is based off of a pre-operative patient weight,but this impact is negligible and should be equal in both groups.Patients taking anticoagulation or antiplatelet medications could also have increased blood loss and this was not taken into account in our analysis.However,patients are usually instructed to stop such medications before an operation.These calculations impose rigid mathematical formulas on patients representing a range of body compositions and physiologic responses to surgery that are dynamic and idiosyncratic.This may be particularly relevant in tertiary referral centers that see a non-representative range of body habitus and patients with impaired compensatory responses to hemorrhage.However,calculated blood loss has several advantages over surgeon estimation,including its standardization and immunity to the bias of a surgeon’s visual assessment.It is also easily replicable at other centers and avoids the logistical hassles of alternative methods such as weighing surgical drapes and sponges.
A second limitation is that our patient population was heterogenous and derived from an academic center,and therefore potentially less generalizable.This fact is offset by our study being the first to approach this question in an orthopedic patient population,which differs from the more commonly studied general surgery population in terms of indications and patient characteristics.Second,the patients underwent procedures by a diverse group of surgeons employing a range of surgical techniques,increasing the external validity of our results.
Results of multivariate regression are shown in Table 2.Of the tested variables,only the indication for surgery modified the association between tourniquet use and blood loss above the 10% threshold for inclusion.Though it differed significantly between tourniquet and non-tourniquet groups,age did not significantly modify the association between tourniquet use and blood loss.Two patients with missing data for creatinine were excluded from stepwise regression modelling but were included in the final multivariate model.The interaction term between tourniquet use and indication for surgery was not significant (= 0.84 for trauma and= 0.99 for tumor,relative to infection).
Our study found no evidence of effect modification by the indication for surgery,indicating that use of a tourniquet does not have a variable effect on blood loss in oncology,infection,and trauma patients.However,the subgroup analysis was not powered to detect a difference in blood loss;comparisons within these groups were affected by small sample sizes,particularly in the group undergoing amputation due to trauma (= 11).Thus,both the individual subgroup analyses and the lack of evidence for effect modification should be interpreted with caution.
CONCLUSION
We found that tourniquet use during below knee amputation is associated with decreased calculated intraoperative blood loss.The decision to use a tourniquet depends on multiple factors related to the individual patient,the underlying pathology being treated,and surgeon preferences.However,based on these results,we recommend that surgeons performing this procedure use a tourniquet if they wish to minimize blood loss.Analysis of a larger database may provide supporting evidence for tourniquet use in specific patient subgroups including patients with malignant tumors and those who sustained acute traumatic injury.
ARTICLE HIGHLIGHTS
Research background
Below-knee amputation (BKA) is common procedure in the orthopedic population.Etiology for patients requiring this surgery are primarily trauma,infection,and neoplastic disease.There is currently no consensus among orthopedic surgeons regarding the use of a tourniquet in these patients.
It was not until he had sought vainly for the imaginary monster that he realised that this was the Princess herself, and by that time he was deeply in love with her, for indeed it would have been hard to find anyone prettier than Potentilla, as she sat by the brook8, weaving a garland of blue forget-me-nots to crown her waving golden locks, or to imagine anything more gentle than the way she tended all the birds and beasts who inhabited her small kingdom, and who all loved and followed her
Research motivation
The motivation behind this study is to determine a possible method to minimize blood loss in BKA operations.
Research objectives
To compare blood loss between patients who received a tourniquet during their BKA procedure and those who did not.
Research methods
When he came to the outskirts26 of the wood he said to his followers27: You wait here, I ll manage the giants by myself ; and he went on into the wood, casting his sharp little eyes right and left about him
Research results
We found that patients undergoing a BKA operation with tourniquet use were associated with a 488 mL decrease in calculated blood loss.This is significant for orthopedic surgeons wanting to minimize blood loss in BKA operations.
Research conclusions
This study utilized a calculated blood loss rather than the commonly utilized estimated blood loss,and proposes that a tourniquet should be used if orthopedic surgeons wish to minimize blood loss in BKA operation.
Research perspectives
Research should be conducted on a larger population across multiple centers to determine a stronger association and increase external validity.
The nightingale sang so sweetly that the tears came into the emperor’s eyes, and then rolled down his cheeks, as her song became still more touching and went to every one’s heart
Woelber E,Meeker J and Working Z contributed the study conception and design;Wyland AE,Wong LH and Arakawa J contributed the generation,collection of the data;Wyland AE and Woelber E contributed the assembly,analysis and/or interpretation of the data;Wyland A,Woelber E,Meeker J and Working Z contributed to drafting and revising the manuscript.
This study was approved by the Institutional Review Board (STUDY00020406).
All study participants or their legal guardian provided informed written consent about personal and medical data collection prior to study enrolment.
Each author certifies that he or she has no commercial associations (consultancies,stock ownership,equity interest,patent/Licensing arrangements,) that might pose a conflict of interest in connection with the submitted article.
Data and study materials are available upon reasonable request from the corresponding author at meekerj@ohsu.edu.Consent was not obtained,but the data are anonymous and the risk of identification is low.
The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
: United States: Alden E Wyland 0000-0003-2703-6460;Erik Woelber 0000-0002-4173-2860;Liam H Wong 0000-0003-4429-1789;Jordan Arakawa 0000-0001-9729-302X;Zachary M Working 0000-0003-1768-1001;James Meeker 0000-0002-8346-7938.
8.Looking-glasses:In other words, mirrors. Mirrors are also a sign of luxury and wealth. In fairy tales, mirrors can be representative of a character s true nature which they reflect. Mirrors are especially important in Snow White and the Seven Dwarfs57.
: Wang LL
: A
: Wang LL
杂志排行

World Journal of Orthopedics的其它文章
- Risk of methicillin-resistant Staphylococcus aureus prosthetic joint infection in elective total hip and knee arthroplasty following eradication therapy
- Outcomes after arthroscopic repair of rotator cuff tears in the setting of mild to moderate glenohumeral osteoarthritis
- Clinical and mechanical outcomes in isolated anterior cruciate ligament reconstruction vs additional lateral extra-articular tenodesis or anterolateral ligament reconstruction
- Does orthotics use improve comfort,speed and injury rate during running? Preliminary analysis of a randomised control trial
- Septic arthritis of the hand:Current issues of etiology,pathogenesis,diagnosis,treatment