Efficacy and safety of external application of Chinese herbal medicine for psoriasis vulgaris:a systematic review of randomized controlled trials
2022-07-20LINYiLIXunWANGZiZHENGXiaoranHANGHaiyanLILingling
LIN Yi,LI Xun,WANG Zi,ZHENG Xiaoran,HANG Haiyan,LI Lingling
LIN Yi,WANG Zi,ZHENG Xiaoran,HANG Haiyan,LI Lingling,Department of Dermatology,Dongzhimen Hospital,Beijing University of Chinese Medicine,Beijing 100700,China
LI Xun,Centre for Evidence-Based Chinese Medicine,Beijing University of Chinese Medicine,Beijing 100029,China
Abstract OBJECTIVE:To evaluate the clinical efficacy and safety of external application of Chinese herbal medicine (ex-CHM) for psoriasis vulgaris (PV).METHODS:Different search portals,including the China National Knowledge Infrastructure Database,China Science and Technology Journal Database,Wanfang,SinoMed,clinicaltrials,PubMed,Cochrane Library,and Cochrane Central Register of Controlled Trials,were searched for randomized controlled trials (RCTs) that compared the ex-CHM intervention with other treatment protocols for PV,with available data as of November 25,2020.The Review Manager 5.3 software was used for analysis.RESULTS:Nineteen RCTs involving 1988 participants were included,of which twelve RCTs qualified for the Meta-analysis.The results showed that the addition of CHM bath to narrow-band ultraviolet B (NB-UVB) had a higher response rate [RR=1.29;95% CI (1.19,1.40);P< 0.000 01];lower psoriasis area severity index (PASI)[MD=-3.15;95% CI (-4.79,-1.52);P=0.000 2)],adverse reactions rate [RR=0.32;95% CI (0.15,0.66);P=0.002],and recurrence rate [RR=0.48;95% CI (0.30,0.79);P=0.004] than NB-UVB alone.The addition of CHM fumigation to NB-UVB also showed a higher response rate [RR=1.29;95% CI (1.11,1.49);P =0.000 7] and lower adverse reactions rate [RR=0.44;95% CI (0.24,0.79);P=0.006].In addition,CHM bath could reduce the adverse reactions induced by 308 nm excimer laser and improve patients' quality of life better than phototherapy.CHM fumigation could improve the efficacy of calcipotriol ointment and reduce the adverse reactions.CHM fumigation combined with external washing plus acitretin showed better results than using acitretin alone.No statistical difference was observed between CHM external washing and calcipotriol ointment or CHM ointment and retinoic acids.CONCLUSIONS:Current evidence showed that CHM bath and fumigation appeared to be efficient and safe for PV treatment.However,no definite conclusion could be drawn due to the low quality of included studies and thus more well-designed studies are needed for further assessment.
Keywords:psoriasis;Chinese herbal medicine;treatment outcome;safety;randomized controlled trial;systematic review
1.INTRODUCTION
Psoriasis is a chronic and inflammatory skin disease associated with hereditary and environmental factors and mediated by the immune system.With changes in the social environment,psoriasis incidence is on the rise with 3% of the population affected worldwide,1making the condition a major public health challenge.2
Psoriasis vulgaris (PV),which affects about 80% of psoriasis patients,3,4is a key classification in the treatment of psoriasis,of which the typical clinical manifestations include scaly erythema or plaques.The use of conventional medicine (CM),such as glucocorticoids,tretinoin,and calcineurin inhibitors,is the current external treatment for PV.However,in severe cases,the patients need to receive combined treatments through systemic therapy,phototherapy and biological agents.Although these treatments can take effect immediately,their downsides include potential contraindications and adverse reactions,making them unsuitable for long-term therapy.For example,tretinoin may induce deformity,and thus cannot be used in pregnant women.5External application of calcipotriol ointment can easily cause symptoms of local irritation,such as skin erythema,burning sensation and pruritus.6Moreover,PV can recur easily after a sudden stop in glucocorticoid treatment.7Biological agents are costly,some of which may pose a risk of inducing tumors and activating the hepatitis B virus.8Thus,effective and safe therapies which are available at a low cost are urgently needed.
China has a long history of treating psoriasis with Chinese Herbal Medicine (CHM).Traditional Chinese Medicine believes that psoriasis is mainly caused by‘excessive blood-heat-toxin’,which obstructs the normal skin development.External application of CHM (ex-CHM) means applying the CHM externally in the form of an ointment,decoction,among others.It is also based on symptom pattern identification such as blood-heat syndrome,blood-dryness syndrome,and blood-stasis syndrome,so that the drugs can directly take effect at the disease location,and on regulating and harmonizing theQiand blood9Also,some of the CHM may have antiinflammatory and antiproliferation effects.10In addition,ex-CHM can be used for long-term treatment with low cost and minor irritation.Some studies have shown that ex-CHM is effective and safe for use in PV.However,the sample size of each study is limited and their quality is uneven.Therefore,evidence-based medicine is needed to confirm its efficacy and safety.
Only one systematic review (2012)11evaluated the clinical efficacy and safety of ex-CHM for PV.A total of ten RCTs were included with 1435 patients involved.The results showed that ex-CHM could improve the response rate of ultraviolet B (UVB) or narrow-band ultraviolet B (NB-UVB) and reduce the number of adverse reactions.Furthermore,ex-CHM and external application of conventional medicine (ex-CM) showed equivalent efficacy.However,the conclusions did not accurately distinguish the ex-CHM therapies and the included studies were few in number and generally low quality.In recent years,more relevant studies have been reported,however no updated systematic reviews have been performed.Therefore,the purpose of this review is to evaluate the efficacy and safety of ex-CHM for PV treatment,and to provide high-level evidence for further clinical application.
2.MATERIALS AND METHODS
2.1.Inclusion criteria
The following were the inclusion criteria of the study:Participants:psoriasis vulgaris patients with clear diagnostic criteria.
Intervention measures:the experimental group received ex-CHM interventions,which included CHM ointment,emulsion,bath,fumigation,external washing,etc.,whereas the control group received the placebo,CM,or physical therapy.Both groups could have common basic therapies.
Outcome measures:the primary outcome measure was the response rate evaluated by the psoriasis area and severity index (PASI).The efficacy index (EI)=(Pretreatment PASI score– Post-treatment PASI score)/Pretreatment PASI score×100%,and the EI ≥ 60% was considered effective.12The secondary outcomes included PASI,recurrence rate (number of relapses/recoveries),dermatology life quality index (DLQI) and adverse reactions.
Types of studies:randomized controlled trials (RCTs).
2.2.Exclusion criteria
The following were the exclusion criteria of the study:(a)studies published repeatedly.(b) studies without sufficient data for analysis.
2.3.Search methods
To obtain all relevant published or registered RCTs,the following websites were searched:PubMed,Cochrane Library and the Cochrane Central Register of Controlled Trials,clinicaltrials,SinoMed,China National Knowledge Infrastructure Database,China Science and Technology Journal Database,and Wanfang from their inception dates to November 25,2020,with no language restrictions applied.The search terms consisted of three aspects:clinical condition (psoriasis,etc.),intervention(herb,bath,etc.),and study type (clinical,random,etc.).The search strategy used for PubMed has been provided in S1 of supplementary materials.
2.4.Selection of studies
All the retrieved articles were imported into Endnote.x9 software and selected by two authors (LIN Yi and LI Lingling) independently.Unmatched articles were excluded by screening the titles and abstracts after removal of duplicates.The remaining articles were downloaded and read to select publications based on the inclusion and exclusion criteria.The reasons for excluding articles needed to be recorded.For duplicate articles,if the contents were the same,the paper with the earliest publication date was selected;if not,the more complete one was selected.
2.5.Assessment of risk of bias
Two authors (LIN Yi and LI Lingling) independently assessed the methodological quality of the included studies using the “risk of bias” (ROB) assessment recommended by Cochrane Handbook 5.2.Any disagreement was resolved through discussion with a third author (LI Xun).
2.6.Data extraction
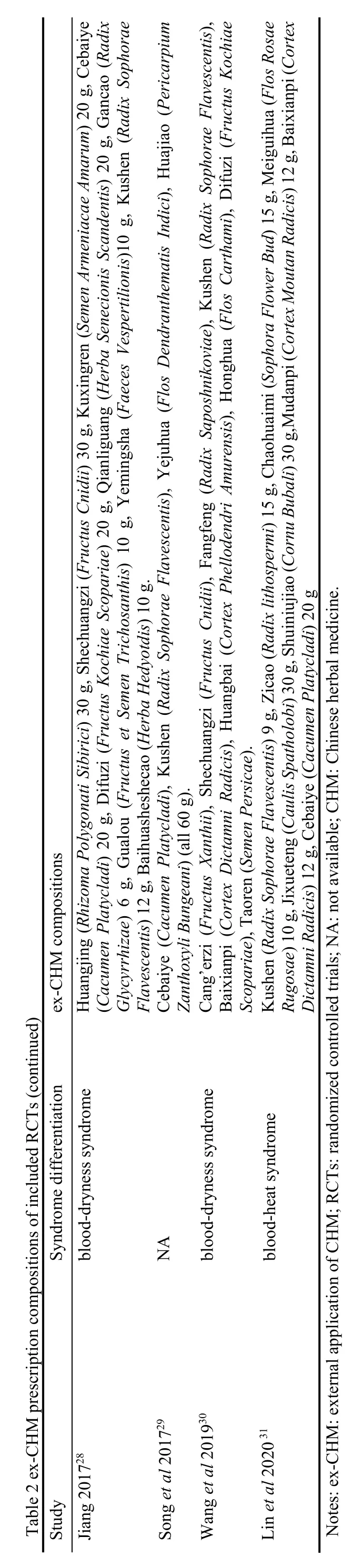
Two authors (LIN Yi and LI Lingling) independently extracted the data from each selected study using a data extraction table based on MS Excel.The information included the following:the first author,publication year,diagnostic criteria,disease stages,syndrome differentiation,sample size,age of patients,treatment duration,interventions (including compositions of ex-CHM prescriptions),follow-up periods,outcome measures,and corresponding data for efficacy values.Disagreements were resolved through discussion with a third author (LI Xun).If the data were unclear,the corresponding author of the paper was contacted to clarify the data.
2.7.Data analysis
The included studies were evaluated for clinical heterogeneity,and theI² test was used for statistical heterogeneity evaluation.WhereP> 0.10,I² < 50%,the fixed-effects model was adopted;WhereP< 0.10,I² ≥50%,the statistical heterogeneity was considered significant,and the random-effects model was adopted.Subgroup analysis or descriptive analysis was performed in studies with significant heterogeneity,and sensitivity analysis was used to find the sources of heterogeneity.Dichotomous data were expressed as a risk ratio (RR) and 95% confidence interval (CI),whereas the continuous data were expressed as a mean difference (MD) and 95%CI.A funnel plot was applied to evaluate the publication bias when more than ten trials were included.Review Manager 5.3 software (provided by the Cochrane Library,London,UK) was used for Meta-analysis.
3.RESULTS
3.1.Study selection
A total of 7581 articles were searched out,and 19 RCTs13-31in Chinese were included in this review(Figure 1).
3.2.Methodological quality of included RCTs
Only 11 out of 19 studies described the specific content of the random methods.16,18-21,23-25,28-30No study described the allocation concealment.The 19 studies not using blinding methods were assessed as “high risk,” and no study mentioned blinding of the outcome assessment.In one study,25there was a loss of follow-up,which affected the accuracy of the recurrence rate and caused an incomplete outcome dataset,therefore this study was assessed as “high risk.” Two studies15,17were assessed as “high risk” in terms of “selective outcome reporting”because the outcomes of adverse reactions were not mentioned in the methods sections.An “unclear risk”assessment was given to all studies since it was hard to tell if there were any other significant biases (Figure 2).
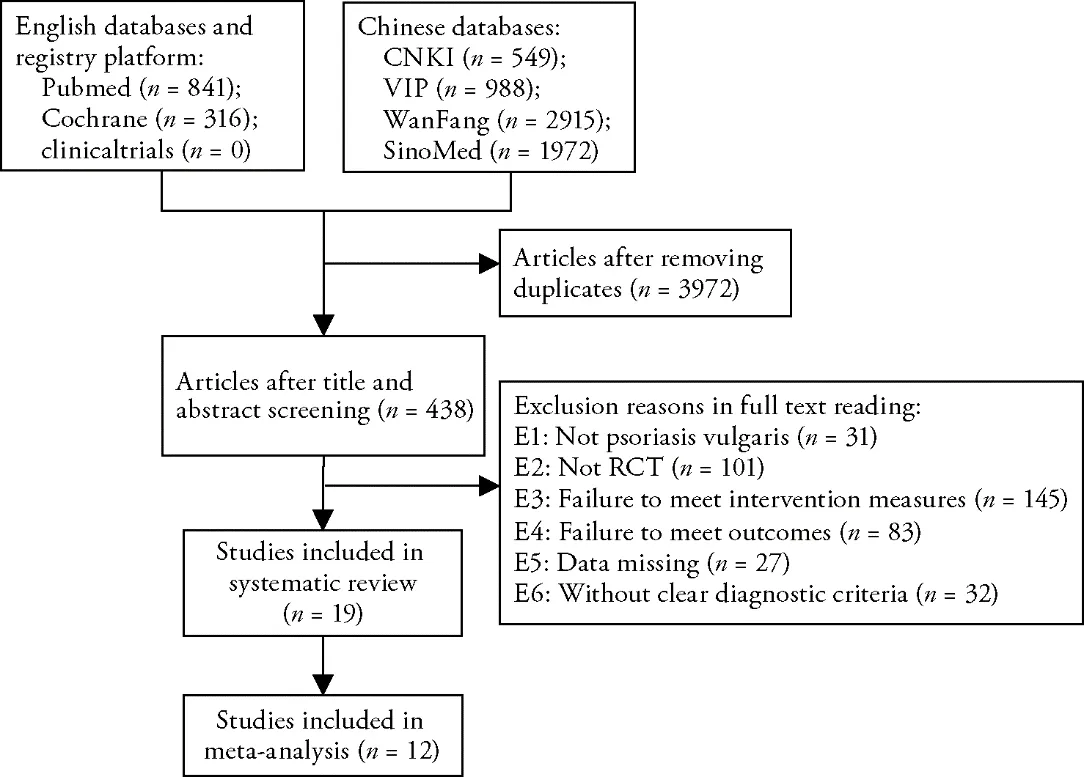
Figure 1 Flowchart depicting the study selection
3.3.Basic information of included studies
The characteristics of the 19 studies included were extracted and shown in Tables 1 and 2.The 19 RCTs were all conducted in China with a total of 1988 patients,including 1004 in the experimental groups and 984 in the control groups.Each study had clear diagnostic criteria.One study13was a multi-center RCT.Eight studies contained participants with quiescent stage psoriasis.13,14,16,17,22,28-30Differentiation of syndromes was used in seven studies.As to the interventions investigated,the experimental groups had four kinds of ex-CHM therapies,including the external application of the ointment,CHM fumigation,CHM bath,and CHM external washing.Each study used one CHM compound prescription.The CHM used mainly included blood-cooling medicinals :Zicao(Radixlithospermi),Shengdihuang(Radix Rehmanniae),Mudanpi (Cortex Moutan Radicis),etc.,heat-clearing medicinals:Jinyinhua (Flos Lonicerae),Tufuling (Rhizoma Smilacis Chinae),Kushen (Radix Sophorae Flavescentis),Huangqin (Radix Scutellariae Baicalensis),etc.,blood-activating medicinals:Danshen(Radix Salviae Miltiorrhizae),Honghua (Flos Carthami),etc.,and blood-nourishing medicinals:Danggui (Radix Angelicae Sinensis),Yamazi (Semen Lini Usitatissimi),etc.The control groups used CM (oral or external) and phototherapy.In addition,the outcomes based on the response rate and adverse reactions were reported in all studies.The PASI assessment was not reported in five studies.14,17,18,22,26Two studies17,22reported the recurrence rate with a follow-up period of six months.DLQI was reported in four studies.21,23,27,29
3.4.Efficacy and safety of ex-CHM
3.4.1.Response rate
All the 19 RCTs reported the response rate of the interventions.Descriptive analysis was performed for seven studies since their clinical heterogeneity was significant due to differing interventions (Table 4).Two studies compared CHM ointment with CM (tretinoin cream,25acitretin26) and the differences were not statistically significant.Another two studies28,30comparing CHM external washing with calcipotriol ointment showed no statistical differences in terms of response rates.In one study,24CHM fumigation combined with external washing improved the efficacy of acitretin.In another study,31CHM fumigation plus calcipotriol ointment showed better efficacy than calcipotriol ointment alone.One study23showed that the addition of CHM bath to single 308nm excimer laser irradiation did not significantly improve the efficacy.
The other 12 studies were pooled in the Meta-analysis and were divided into 4 subgroups based on interventions.A fixed-effects model was adopted.The results showed that CHM bath or fumigation could improve the efficacy of a single NB-UVB.CHM bath could also improve the efficacy of NB-UVB plus urea ointment or ex-hormone(Table 3).
3.4.2.Publication bias
A funnel plot of the response rate was drawn to evaluate publication bias.The results showed that the left and right distributions were asymmetrical,suggesting a possible publication bias (Figure 3).
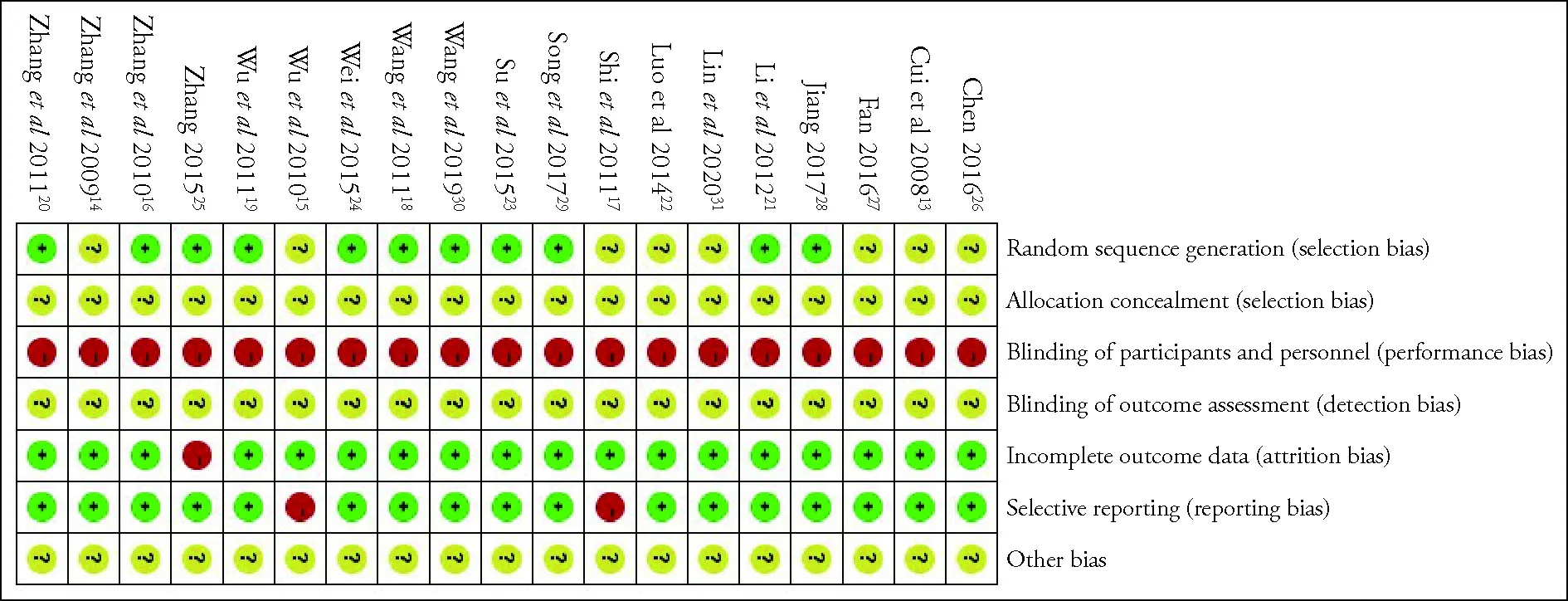
Figure 2 Risk of bias summary

Figure 3 Funnel plot of the response rate
3.4.3.PASI
A total of 14 studies reported PASI scores.Descriptive analysis was performed on six studies since their clinical heterogeneity was significant due to their differing interventions (Table 4).Two studies showed no statistical difference between CHM ointment25or CHM external washing30and ex-CM.In one study,28CHM external washing plus ex-CM was better than ex-CM alone in improving PASI.In another study,24it was shown that the addition of CHM fumigation combined with external washing to acitretin could improve the PASI much better than the control.One study31showed that CHM fumigation plus calcipotriol ointment had lower PASI scores than single calcipotriol ointment.In one study,23CHM bath plus 308nm excimer laser could improve the PASI scores better than using 308nm excimer laser alone.
The other eight studies were pooled in the Meta-analysis and were divided into 4 subgroups based on interventions.The random-effects model was adopted since the groups showed significant statistical heterogeneity (P<0.10,I2=88%).A sensitivity analysis showed that no significant decrease was observed in heterogeneity when we excluded the study one by one,which may be related to different sample sizes.The results showed that,compared with NB-UVB alone,the addition of CHM fumigation or bath could improve the PASI outcome(Table 3).
3.4.4.Recurrence rate


Two studies17,22accurately reported the recurrence rate with follow-up of recovered patients for six months.The fixed-effects model was adopted since the statistical heterogeneity was not significant (P>0.1,I2=42%):RR=0.48,95%CI(0.30,0.79),P=0.004.The result showed that the recurrence rate of CHM bath plus NBUVB was significantly lower than NB-UVB alone.
3.4.5.DLQI
Four studies21,23,27,29reported the DLQI.In each study,the DLQI in the experimental group was lower than the control group after treatments,and the differences were statistically significant (P<0.05;Table 5).
3.4.6.Adverse reactions
The adverse reactions were monitored in 19 studies during the course of treatment,of which adverse dermatological reactions were observed:pruritus,13-17,20-24,26-27,31skin flushing,19,29erythema,13,14,16,17,20-23,26,31skin dryness,14-15,18-22,24,27,31scorching hot,16,18,27,28,30burning pain,14,19,26,29stabbing pain,28blister,23and skin irritations.25A few patients had systemic adverse reactions:stuffy discomfort20caused by CHM fumigation and gastrointestinal discomfort24caused by acitretin.These adverse reactions above were all alleviated after symptomatic treatment or by adjusting the dosage.No severe adverse reactions occurred and no patient in any trial terminated the treatment due to adverse reactions.
Descriptive analysis was performed on seven studies with significant clinical heterogeneity and studies with systemic adverse reactions (Table 4).One study25compared CHM ointment with ex-CM,and the difference was not statistically significant.In another study,18the combination of CHM ointment reduced the adverse reactions caused by oral CM.Two studies28,30compared the CHM external washing with calcipotriol ointment with no statistical differences observed.In one study,31CHM fumigation could reduce the adverse reactions caused by calcipotriol ointment.One study23showed that the addition of CHM bath to 308 nm excimer laser had fewer adverse reactions.In another study,24comparing with acitretin alone,CHM fumigation combined with external washing plus acitretin showed no significant advantage in reducing the adverse dermatological reactions.However,gastrointestinal discomforts were not observed in the treatment group.A patient experienced stuffy discomfort during CHM fumigation,20but the symptom disappeared after lowering the temperature in the treatment cabin.
The other 12 studies were divided into 4 subgroups to analyze the adverse dermatological reactions.The heterogeneity was significant in group 2 (P<0.10,I2=73%).The sensitivity analysis showed that the heterogeneity decreased when one study19was excluded(P>0.10,I2=45%),which may be related to its large phototherapy dose.In that study,CHM bath combined with NB-UVB showed more phototoxic reaction than NB-UVB alone.As a result,the 11 studies were pooled in the Meta-analysis [RR=0.41;95%CI(0.29,0.57),P<0.000 01].Furthermore,the fixed-effects model was adopted.The results showed that CHM bath or fumigation plus NB-UVB could reduce the adverse dermatological reactions of NB-UVB.Compared with NB-UVB plus urea ointment or ex-hormone,the combination of CHM bath to them showed no significant differences in reducing dermatological adverse reactions(Table 3).

Table 3 Meta-analysis of the response rate,PASI,adverse dermatological reactions (comparing ex-CHM with other therapies for psoriasis vulgaris treatment)
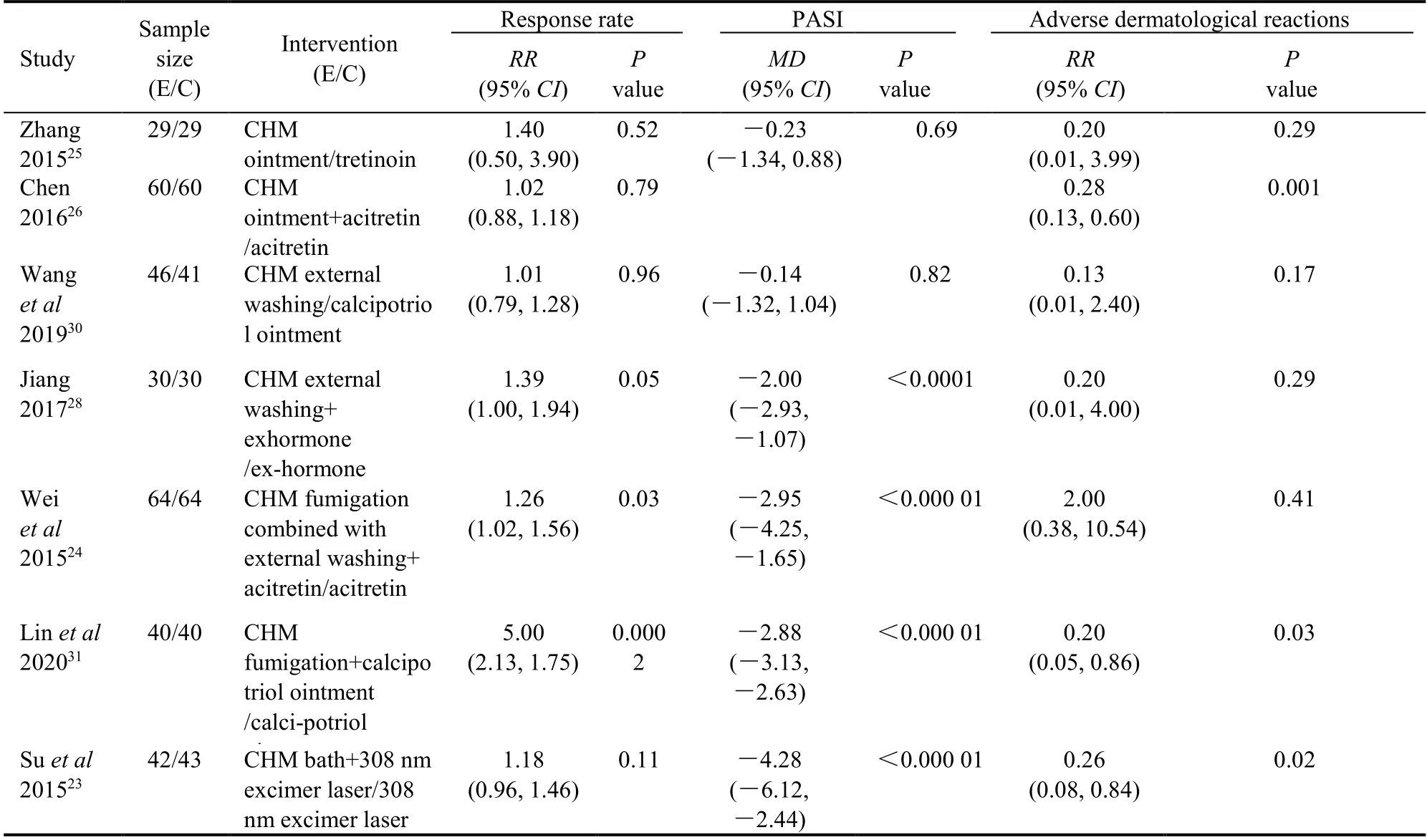
Table 4 Descriptive analysis of the response rate,PASI,adverse reactions (comparing ex-CHM with other therapies for psoriasis vulgaris treatment)

Table 5 Descriptive analysis of DLQI (comparing ex-CHM with other therapies for psoriasis vulgaris treatment)
4.DISCUSSION
This systematic review included 19 RCTs that mainly compared the ex-CHM plus other therapies with other therapies.A total of 12 RCTs were included in the Metaanalysis:CHM bath and fumigation showed some efficacy and safety by increasing the response rate,reducing the PASI score and adverse reactions of NBUVB.A combination with CHM bath could also reduce the recurrence rate of NB-UVB and improve the efficacy of NB-UVB plus urea ointment or ex-hormone.In addition,one study23showed that CHM bath plus 308nm excimer laser could reduce the adverse reactions and DLQI better than 308 nm excimer laser alone.The combination of CHM bath could also decrease the DLQI better than NB-UVB,27NB-UVB plus urea ointment,29NB-UVB plus ex-hormone,21thereby improving the patients' quality of life.In one study,the addition of CHM fumigation to calcipotriol ointment had better results than calcipotriol ointment alone.In another study,24CHM fumigation combined with external washing could improve the efficacy of acitretin and reduce the adverse reactions of gastrointestinal discomfort.In a CHM fumigation study,20a patient experienced stuffy discomfort during fumigation and the symptom disappeared after lowering the temperature in the treatment cabin.The apparent absence of statistical differences between CHM external washing and calcipotriol ointment,or CHM ointment and tretinoin(oral/external) in terms of the response rate may result from few studies included with insufficient sample size.The clinical efficacy of CHM ointment or external washing need to be evaluated further by more studies.
The results showing CHM bath could improve the efficacy and reduce the adverse reactions of NB-UVB were consistent with the conclusions of the previous systematic review.In addition,this review included more studies involving more kinds of ex-CHM therapies and we distinguished these therapies in the analysis.Furthermore,the outcome measure of DLQI was added in this review.The results showed that CHM fumigation also had good efficacy and safety.The addition of CHM bath could also decrease the recurrence rate of NB-UVB treatment,reduce the adverse reactions of 308nm excimer laser,and improve the life quality of patients who received NB-UVB or NB-UVB plus ex-CM.
The significant efficacy and safety of CHM bath and fumigation are most likely related to the efficacy of CHM and the physicochemical effects of external treatments.The pathological manifestations of psoriasis include hyperkeratosis of the epidermis,telangiectasia of the dermis,and infiltration of neutrophils.The immune response involving helper T cells (Th17) is an important immunological mechanism in psoriasis.Interleukin 22(IL-22) and IL-17,which are produced after activation of Th17,can directly lead to the abnormal proliferation of keratinocytes (KC) .32,33Under the stimulus of these cytokines,KC releases vascular endothelial growth factor,tumor necrosis factor alpha (TNF-α),and IL-23,promoting distortion and hyperplasia of skin blood vessels and infiltration of neutrophils.34Besides the effects of CHM syndrome differentiation,pharmacological studies have shown that some CHM used in the included studies can also affect the immunological mechanism of psoriasis35and reduce its pathological manifestations.For example,Tufuling (Rhizoma Smilacis Chinae) can selectively inhibit T lymphocytes from releasing inflammatory factors.36The Zicao (Radix lithospermi)plays a role in the treatment of inflammation,itching,and general skin protection.37The Alkannin can inhibit the proliferation of HaCat cells and the secretion of related cytokines.38The Oxymatrine in Kushen (Radix Sophorae Flavescentis)39can inhibit the expression of IL17 and IL22 induced by Th17 in KC,inhibit the proliferation of epidermal cells,and reduce the TNF-α level in serum.40The physicochemical effects of bath and fumigation therapies should not be ignored as both include“hydrotherapy effect” and “thermal effect”.41The bath therapy involves storing CHM decoction in a container with the whole or part body soaking in.The CHM can be absorbed through the skin,orifices,and acupoints so that they can play the role for the overall treatment by dredging the meridian and harmonizing theQiand blood.The fumigation therapy involves the use of the CHM decoction steam produced by the steam equipment to fumigate the skin.The CHM steam can transport into the blood circulation through the skin and play its therapeutic effect.The hydrotherapy effect of bath and fumigation therapies can effectively remove the scales,scabs,and secretions on the skin.The thermal effect can make skin pores dilate,thereby promoting drug absorption.It can also dilate the capillaries and promote blood circulation,which helps in reducing inflammation.41
As to adverse reactions,CHM bath and fumigation could reduce the skin dryness,itching,erythema,flushing,burning,and blisters caused by phototherapy.This is because the hydrotherapy effect can remove the scales and scabs,thus increasing the passing rate of NB-UVB and 308nm excimer laser and reducing the required irradiation dose.Therefore,phototherapy dosage should be reduced after CHM bath or fumigation to avoid aggravating phototoxic reactions.CHM fumigation combined with external washing could reduce the gastrointestinal discomfort caused by acitretin.This is probably because the thermal effect can improve blood circulation,accelerate gastrointestinal motility,and promote body metabolism.In a CHM fumigation study,20a patient experienced mild stuffy discomfort,which was related to excessive temperature in the treatment cabin.Therefore,the temperature should be adjusted according to the patients' tolerance,generally between 38 ℃ and 45 ℃,8to avoid this type of adverse reactions.
Two studies with a 6-month follow-up period found that combining CHM bath with NB-UVB could decreased the recurrence rate better than NB-UVB alone,indicating that CHM bath could prolong the recovery period of patients with psoriasis vulgaris and delay the recurrence time.This is probably because the CHM bath can effectively improve the efficacy of NB-UVB and regulate the body as a whole.By improving the efficacy and reducing the adverse reactions and recurrence,the life quality of patients can therefore be improved.
The limitations of this systematic review are the poor methodological quality of some included studies and the lack of long-term follow-up of adverse reactions and recurrence.In addition,the lack of studies comparing the efficacy of placebos reduces the reliability of the results.Finally,the included studies are all conducted in China,and the efficacy and safety of ex-CHM for populations in other countries remain to be studied,for there may bedifferences in response to drugs based on race.Therefore,relevant studies are suggested to be carried out in more countries for further evaluation and promotion on a larger scale.The limitations above should be considered when interpreting the results and providing a reference for clinical decisions.Future studies should focus on improving the clinical and methodological quality.Studies using other ex-CHM therapies can be carried out to enrich the contents and evidence-based medicine implications of ex-CHM therapies.
In conclusion,this systematic review shows that ex-CHM has advantages in treating psoriasis vulgaris to some extent,especially CHM bath and fumigation.However,more multi-center,large-sample,high-quality RCTs are still needed to confirm the results due to methodological flaws in each of the included studies.Although the efficacy of CHM ointment and external washing is not significant,the lack of study numbers and insufficient sample size may explain this finding,and thus further studies must be conducted.
5.REFERENCES
1.Parisi R,Symmons DP,Griffiths CE,Ashcroft DM.Global epidemiology of psoriasis:a systematic review of incidence and prevalence.J Invest Dermatol 2013;133:377-85.
2.Griffiths CEM,Walt JM,Ashcroft DM,et al.The global state of psoriasis disease epidemiology:a workshop report.Br J Dermatol 2017;177:e4-7.
3.Biondi Oriente C,Scarpa R,Pucino A,Oriente P.Psoriasis and psoriatic arthritis.Dermatological and rheumatological cooperative clinical report.Acta Derm Venereol Suppl (Stockh)1989;146:69-71.
4.Ayala F.Clinical presentation of psoriasis.Reumatismo 2007;59:40-5.
5. Bruner CR,Feldman SR,Ventrapragada M,Fleischer Jr AB.A systematic review of adverse effects associated with topical treatments for psoriasis.Dermatol Online J 2003;9:2-12.
6.Yang DQ,Zhang LX,Bai YP.Clinical observation of sequential therapy of calcipotriol ointment and halometasone cream in the treatment of plaque psoriasis.Lin Chuang Pi Fu Bing Xue Za Zhi 2009;38:401-3.
7.Ma WP,Liu J,Zhu HP.Conversion of psoriasis vulgaris to erythrodermic psoriasis caused by glucocorticoid:a case report.Pi Fu Bing Yu Xing Bing 2010;32:63.
8.Psoriasis Professional Committee of Dermatology Branch of Chinese Medical Association.Chinese guidelines for the diagnosis and treatment of psoriasis (2018 full edition).Zhong Hua Pi Fu Ke Za Zhi 2019;52:667-710.
9.Cheng YY,Lu YP.Clinical application of Sanzi granule.Zhong Yi Wai Ke Za Zhi 2014;23:63-4.
10.Man MQ,Shi Y,Man M,et al.Chinese herbal medicine (Tuhuai extract) exhibits topical anti-proliferative and antiinflammatory activity in murine disease models.Exp Dermatol 2008;17:681-7.
11.Li N,Li YQ,Li HY,Guo W,Bai YP.Efficacy of externally applied Chinese herbal drugs in treating psoriasis:a systematic review.Chin J Integr Med 2012;18:222-9.
12.Zheng XY.Guiding principles for clinical research of new Chinese medicine.Beijing:China Medical Science and Technology Press,2002:299-302.
13.Cui BN,Sun YX,Liu WL,Liao GL.Efficacy observation of narrow-spectrum uvb combined with Yuyin prescript tion bath in the treatment of psoriasis vulgaris.Zhong Guo Zhong Xi Yi Jie He Za Zhi 2008;355-7.
14.Zhang CM,Wei G,Zhang CH,Pang L,Shi YJ,Cai Y.The efficacy of Chinese herbal medicine fumigation combined with ultraviolet irradiation in the treatment of psoriasis and their efficacy on Thl/Th2 cytokines in serum.Zhong Hua Wu Li Yi Xue Yu Kang Fu Za Zhi 2009;491-2.
15.Wu LN,Huang LN,Xue RZ.Efficacy observation and nursing care of narrow-spectrum uvb combined with Chinese herbal medicine bath in the treatment of psoriasis vulgaris.Pi Fu Xing Bing Zhen Liao Xue Za Zhi 2010;17:242-4.
16.Zhang YS,Wei LP.Efficacy observation of NB-UVB combined with Chinese herbal medicine in the treatment of psoriasis vulgaris.Zhong Guo Ma Feng Pi Fu Bing Za Zhi 2010;26:815.
17.Shi XL,Pan YM,Ma HY,Yang XF.Clinical efficacy observation of NB-UVB combined with Chinese herbal medicine bath in the treatment of psoriasis vulgaris.Zhong Guo Ji Guang Yi Xue Za Zhi 2011;20:314-7.
18.Wang ZX,Wang HJ,Yu ZH,et al.Efficacy observation of Chinese herbal medicine bath combined with NB-UVB in the treatment of psoriasis vulgaris.Henan Da Xue Xue Bao (Medical Science) 2011;30:226-7.
19.Wu B,Chen XD,Xia D,et al.Efficacy observation of Chinese herbal medicine bath combined with NB-UVB in the treatment of psoriasis vulgaris.Zhong Guo Zhong Xi Yi Jie He Pi Fu Xing Bing Xue Za Zhi 2011;10:304-5.
20.Zhang CH,Zhang CM,Du XX,Cai Y.Efficacy observation of Chinese herbal medicine fumigation combined with ultraviolet radiation in the treatment of psoriasis vulgaris.Zhong Hua Wu Li Yi Xue Yu Kang Fu Za Zhi 2011;33:937-9.
21.Li J,Sun SM,Yang ZB.Efficacy of Traditional Chinese Medicine bath combined with narrow spectrum uvb in the treatment of psoriasis vulgaris and the analysis of quality of life.Zhong Guo Zhong Xi Yi Jie He Pi Fu Xing Bing Xue Za Zhi 2012;11:161-2.
22.Luo GP,Qu YB,DI DK,et al.Clinical observation of traditional Chinese medicine bath combined with narrow-spectrum uvb in the treatment of psoriasis.Hubei Zhong Yi Za Zhi 2014;36:12-3.
23.Su LN,Yi XM,Ding YF,Yu N,Ma J.Clinical observation and quality of life evaluation of 42 patients with plaque psoriasis treated with Traditional Chinese Medicine bath combined with 308nm excimer laser.Zhong Guo Pi Fu Xing Bing Xue Za Zhi 2015;29:967-9.
24.Wei B,Jiang ZL.Clinical observation of acitretin combined with Shufu powder fumigation and washing in the treatment of psoriasis vulgaris.Zhong Guo Zhong Xi Yi Jie He Pi Fu Xing Bing Xue Za Zhi 2015;14:45-7.
25.Zhang YL.Clinical efficacy observation of proposed Xiaobi ointment in the treatment of psoriasis blood-heat syndrome.Beijing:Beijing University of Chinese Medicine,2015:29-40.
26.Chen L.Clinical efficacy observation of Fushu Zhiyang ointment combined with acitretin in the treatment of psoriasis vulgaris.Zhong Guo Bao Jian Ying Yang 2016;26:84-5.
27.Fan JJ.Clinical efficacy study of Shufu powder combined with narrow-band uvb in the treatment of psoriasis vulgaris.Guangxi:Guangxi University of Traditional Chinese Medicine,2016:17-27.
28.Jiang NL.Clinical study of Runfu Zhiyang lotion in the treatment of psoriasis vulgaris (deficiency of blood and dryness of wind syndrome).Hunan:Hunan University of Traditional Chinese Medicine,2017:3-14.
29.Song X,Tang SW,Jiang WC,Yang Y,Wang QL,Xie SQ.Traditional Chinese Medicine bath combined with NB-UVB irradiation in the treatment of stable psoriasis vulgaris and their effect on patients' quality of life.Zhong Guo Pi Fu Xing Bing Xue Za Zhi 2017;31:757-9+783.
30.Wang JQ,Lu YP.Clinical observation of Niupixuan lotion in the treatment of psoriasis vulgaris of deficiency of blood and dryness of wind syndrome.Shanxi Zhong Yi 2019;35:40-1+46.
31.Lin J,Fang YM,Ma LL,Ji C,Li YY.Clinical study on the treatment of psoriasis with traditional Chinese medicine steam therapy combined with Calcipotriol Ointment.Xin Zhong Yi 2020;52:94-7.
32.Fragoulis GE,Siebert S,Mclnnes IB.Therapeutic targeting of IL-17 and IL-23 cytokines in immune mediated diseases.Annu Rev Med 2016;67:337-53.
33.Luan L,Han S,Wang H,Liu X.Down-regulation of the Th1,Th17and Th22 pathways due to anti-TNF-α treatment in psoriasis.Int Immunopharmacol 2015;29:278-84.
34.Kollipara R,Downing C,Gordon R,Tyring S.Interleukin-23 in the pathogenesis and treatment of psoriasis.Skin Therapy Lett 2015;20:1-4.
35.Chen X,Zhang RT,Duan XW,Xue M,Qu TG,Li LL.Effectiveness of Xiaoyin Jiedu granules in the treatment of psoriasis vulgaris in patients with blood-heat symptom patterns in terms of Traditional Chinese Medicine.J Tradit Chin Med 2020;40:863-9.
36.Wang JP,Zhang HY,Fu XC.Study advances of chemical constituents and pharmacological effects of Rhizom a Smilacis Glabrae.Hai Xia Yao Xue 2013;25:42-4.
37.Deng S,May BH,Zhang AL,Lu C,Xue CC.Topicl herbal formulae in the management of psoriasis:systematic review with Meta-analysis of clinical studies and investigation of the pharmacological action of main herbs.Phytother Res Ptr 2014;28:480-97.
38.Xie XR,Zhang L,Liu X,Lin Y,Zhang L,Li P.Effect of shikonin on the proliferation of keratinocytes and expression of chemo kine induced by IL-17.Zhong Guo Zhong Yao Za Zhi 2015;40:946-9.
39.Zhou Y,Mou KH,Han D,et al.Matrine can inhibit the expression of keratinocytes IL17RA,IL21R and IL22 R1 induced by Th17.Xian Jiao Tong Da Xue Xue Bao (Medical Sciences) 2014;35:695-9.
40.Shi HJ,Zhou R,Jin SJ,Yang J,Zhang XM.Effects of oxymatrine on levels of IL-2,IL-10 and TNF-α in serum of mouse models with psoriasis.Hua Xi Yao Xue Za Zhi 2010;25:418-20.
41.Yu JJ.Systematic evaluation of the efficacy of external application therapies of Chinese medicine in the treatment of psoriasis vulgaris.Guangzhou:Guangzhou University of Chinese Medicine,2013:29-31.
杂志排行

Journal of Traditional Chinese Medicine的其它文章
- Effectiveness of redcore lotion in patients with vulvovaginal candidiasis:a systematic review and Meta-analysis
- Effectiveness and safety of electroacupuncture for the treatment of pain after laparoscopic surgery:a systematic review
- Effect of astragaloside IV on the immunoregulatory function of adipose-derived mesenchymal stem cells from patients with psoriasis vulgaris
- Shenqihuatan formula (参七化痰方) reduces inflammation by inhibiting transforming growth factor-beta-stimulated signaling pathway in airway smooth muscle cells
- Drug response biomarkers of Pien Tze Huang (片仔癀) treatment for hepatic fibrosis induced by carbon tetrachloride
- Wenshen Yangxue decoction (温肾养血方) promotes follicular development in aged female mice via stimulation of the silent information regulator 3/forkhead transcription factor O1 3a pathway