Comparison of impact of adjuvant treatment of midazolam, fentanyl, and magnesium sulfate with intrathecal bupivacaine on block characteristics and postoperative analgesia in knee arthroplasty: A randomized clinical trial
2022-07-02HesameddinModirEsmailMoshiriMehranAzamiTayebeSadatSayafiSharifi
Hesameddin Modir, Esmail Moshiri✉, Mehran Azami, Tayebe Sadat Sayafi-Sharifi
1Anesthesiology Department, Arak University of Medical Sciences, Arak, Iran
2Department of Orthopedic Surgery, Arak University of Medical Sciences, Arak, Iran
3Student Research Committee, Arak University of Medical Sciences, Arak, Iran
ABSTRACT
KEYWORDS: Block characteristics; Bupivacaine; Fentanyl;Hemodynamic changes; Intrathecal; Magnesium sulfate; Midazolam
1. Introduction
As a promising procedural option for patients with end-stage osteoarthritis of the knee, knee arthroplasty can improve health outcomes, when non-surgical treatments remain no longer perceivably effective alternatives[1-3].
Knee arthroplasty is evinced to be intertwined with occasionally formidable postoperative pain, and it is recognized as a factor attributing to limited rehabilitation, culminating in prolonged hospital stays, and eventually augmenting the treatment-related cost burden[4,5]. Pain management is vital for improving the quality of a patient’s postoperative recovery, which can be boosted through effective preventive analgesia techniques[5]. Hitherto a lot of methods with reported success have been developed to manage postoperative pain, including different analgesics, methods of analgesic administration, and available diverse methods of how procedures should be ongoing[6]. It is expected to offer substantial advantages like the rapid onset of action, improved patients’ comfort,less demand for medication, and favorable sensory and motor block[7].
The fourth most abundant cation found in the human body is magnesium sulfate, as an antagonist of N-methyl-D-aspartate receptors. Therefore, magnesium sulfate is endowed with an analgesic effect and primarily plays a role in the regulation of intracellular calcium levels alongside. Fundamental role of magnesium sulfate in analgesia is mediated by local anesthetics,which decreasingly reduced the permeability of intracellular calcium,whereas calcium channel blockers may potentiate the analgesic effect of the agents[8].
Many studies mirrored well-established efficacy of magnesium in decreasing the time of onset of the block while increasing the quality and duration of anesthesia[9-11]. The clinical significance of magnesium sulfate was previously discovered to be a cost-effective solution that provides postoperative analgesia[12].
Fentanyl is cited as a synthetic narcotic which can, when being administered with local anesthetics for spinal anesthesia, prolong the duration of postoperative analgesia[13]. It is pointed out that the duration of analgesia can be prolonged by administering 100 mg magnesium sulfate or 25 μg fentanyl as adjuvants to bupivacaine,while more hemodynamic stability and fewer side effects were reported in the former[14]. Experimental and clinical studies confirm the documented effects of intrathecal midazolam, including the prolonged duration of analgesia and a short time to achieve motor block, and reduced postoperative nausea and vomiting[2,15].Despite the fact that knee arthroplasty has been declared an ideal solution among the most commonly practiced orthopedic surgeries and the tremendous advances made in surgical and anesthesia techniques, plenty of patients continue to suffer from acute postoperatively developed pain. It is thus necessarily true that we need to develop effective measures to reduce the pain. Due to a lack of studies directed to compare the efficacy of these three drugs on hemodynamic changes and block characteristics in bupivacainebased spinal anesthesia, the present trial aimed at comparing the efficacy of midazolam, fentanyl, and magnesium sulfate as adjuvants to intrathecal bupivacaine on both block characteristics and postoperative analgesia in knee arthroplasty.
2. Patients and methods
2.1. Study design
This double-blind clinical trial recruited 105 patients scheduled for knee arthroplasty under spinal anesthesia at the Valiasr and Amir Al-Momenin Hospitals (Arak, Iran) from June 2021 to September 2021.
2.2. Inclusion and exclusion criteria
Inclusion criteria included (1) Patients aged 18 to 60 years; (2)American Society of Anesthesiologists classⅠ andⅡ; (3) Who scheduled for knee arthroplasty; (4) Body mass index ≤30 kg/m2;(5) Who agreed with performing spinal anesthesia or experienced failure of the anesthesia.
Exclusion criteria included (1) History of drug abuse;(2) Cardiovascular problems; (3) Coagulation disorders; (4)Arrhythmia; (5) Mental health problems; (6) Lack of peripheral and central neuropathy; (7) Local infection at the spinal anesthesia injection site (Figure 1).
2.3. Grouping
The patients were divided into three groups (the midazolam group,the fentanyl group, and the magnesium sulfate group) using a balanced block randomization technique procedure (block size: 6),while whose allocation continued until reaching the total sample size of each group, i.e. 35 patients in each group,
2.4. Intervention
The eligible participants were hospitalized at least one day before surgery and received nothing orally for 8 h. Before the operation,patients’ baseline such as heart rate and mean arterial blood pressure were recorded using non-invasive blood pressure monitoring, and arterial blood oxygen saturation was measured by a pulse oximeter.
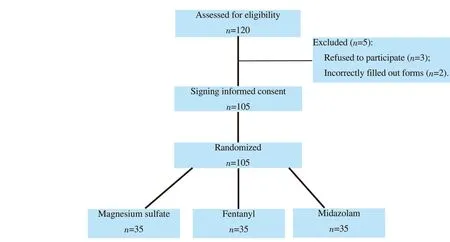
Figure 1. The study flowchart.
All subjects were treated with 10 mL/kg crystalloid (Ringer) and placed in a supine position after transfer to the operating room.The midazolam group received 2 mg preservative-free midazolam(Caspian Tamin Pharmaceutical Company, Rasht, Iran) with 15 mg hyperbaric bupivacaine 0.5%[2]; The fentanyl group received 50 μg fentanyl (Caspian Tamin Pharmaceutical Company, Rasht, Iran) with 15 mg hyperbaric bupivacaine 0.5% (AstraZeneca Pharmaceutical industry company, United Kingdom, imported by Cobel Darou,Tehran, Iran)[9]; The magnesium sulfate group receiving 100 mg preservative-free magnesium sulfate 10% (Pasteur Institute of Iran,Tehran, Iran) with 15 mg hyperbaric bupivacaine 0.5%[14].
For adequate matching among all groups, the volume of the intervention drug was 1 mL in separate sterile syringes and added to 15 mg hyperbaric bupivacaine 0.5% used in all three groups. Thus,the total volume of intrathecal drug administration was adjusted to 4 mL. Surgery was started after spinal anesthesia that was performed using a 25- or 26-gauge Quincke needle at the L3/L4 or L4/L5 intervertebral space.
2.5. Data collection
Mean arterial pressure, heart rate, and oxygen saturation were recorded at 15-minute intervals intraoperatively, during recovery(recovery refers to from the stop of post-anesthesia care unit to the beginning of surgery), and at the scheduled postoperative times (2,4, and 6 h). Hypotension was defined as a decrease of pressure by 20% from the baseline and bradycardia as heart rate<45 beats per minute and SaO2<92%. Remedial action to control hypotension or bradycardia, if occurred, was conducted by administering 15 mg ephedrine and 0.5 mg atropine, respectively[16]. An anesthesiologist measured and recorded the sensory and motor block to T8 or higher in each group, i.e. the level of the first block was assessed by pin prick method using a needle every 1 min after anesthesia, while the second by the Bromage scale every 5 min[17].
It is remarkable to note that the surgeon started surgery once the sensory and motor block was assessed. An intern measured pain scores using the VAS scale, in which zero and ten correspond to the lowest and highest, at 1, 2, 4, 6, and 12, 24 h postoperatively. If VAS was >3 at any time after surgery, patients were given a 100 mg diclofenac sodium suppository (Darou Pakhsh Co., Iran) and the overall dose and the time of administration were recorded[18].Moreover, the time to achieve sensory block to T12 and L1 and Bromage score of 0 and 1 was noted, when recording any other potential complications such as nausea, vomiting, chills, bradycardia,hypotension, and dizziness and conducting further remedial action,if be severe. Furthermore, all cases of analgesic insufficiency and treatment failure were recorded and another technique was chosen for anesthesia and patient preparation for surgery.
Data were measured and recorded by an intern who was not aware of group allocation to ensure a double-blind study. Adjuvants were administered to each group, and spinal anesthesia was prepared by a nurse anesthetist and performed by an anesthesiologist. Consequently,the study was double-blind due to the lack of awareness of each patient and evaluator about the order of groups and interventions.
2.6. Endpoints
The primary outcomes were block characteristics and pain score,moreover, hemodynamic parameters were recorded as the secondary outcome.
2.7. Ethical consideration and trial registration
This study was a part of a research undertaken as a general medicine thesis, with the ethics code of IR.ARAKMU.REC.1399.258 and clinical trial code of IRCT20141209020258N164, and written informed consent and verification of entry/exit criteria were obtained before the study.
2.8. Statistical analysis
The sample size for each group was calculated based on the results of the pain score in our recent study[15] considering a study power of 80%, and a confidence interval of 95%. Therefore, 35 cases were recruited for each group.
Data were analyzed by SPSS 20 software. Categorical data were expressed as frequency and percentage, and quantitative data with normal distribution (checked by Shapiro Wilk test) were expressed as mean and standard deviation. One-way ANOVA and Tukey’s post-hoc tests were used to compare quantitative variables. The significant level of this study was set at α=0.05.
3. Results
In this randomized double-blind clinical trial, 105 patients [54(51.4%) men and 51 (48.6%)] women) were randomized into three groups receiving magnesium sulfate, fentanyl, and midazolam,respectively, with a mean age of (54.50±4.91) years, whereas mean body mass index was (22.79±1.84) kg/m2. Data analysis revealed no statistically significant intergroup difference in terms of oxygen saturation, mean blood pressure, duration of surgery (P>0.05)(Table 1). In addition, postoperative complications including nausea, vomiting, bradycardia, dizziness, as well as hypotension did not observe in any patients, and three groups were without any complication.
The heart rate of the three groups before the operation were 87.82±11.08, 88.48±11.19, and 87.45±8.45 per min in the midazolam group, fentanyl group, and the magnesium sulfate group, respectively. Statistically, significant intergroup differences were found in terms of heart rate at 15, 30, 45, 60, 75, and 105 min after beginning of operation (P=0.010, 0.008, 0.008, 0.004, 0.017,0.034, respectively), with a lower rate in the midazolam group.In addition, the trend of heart rate was depicted by retreaded measurements in Figure 2.
学者王国龙在 《解放战争时期中国共产党对山东解放区的民众动员研究》中重点考察了解放战争时期中国共产党对山东解放区的民众动员,分析了民众动员的背景、基础、历史进程、动员方法以及评价等内容。[9]
Statistically, significant intergroup differences were observed in terms of the onset of sensory block after spinal anesthesia, the time to achieve sensory block to T8 or higher, and the time to achieve sensory block to T12 and L1 (P<0.05) with minimum levels observed in the midazolam group (Table 2).
Similarly, statistically significant intergroup differences were seen in the time to achieve motor block to T8 or higher and the onset of the motor block after spinal anesthesia (P=0.001), and shorter time was observed in the midazolam group. No statistically significant intergroup difference was found in terms of the time to achieve motor block to Bromage Score 0 or 1 (spinal anesthesia wearing off) and pain scores (Table 3 and Table 4) (P>0.05).

Table 1. Demographic and baseline information of the three groups.
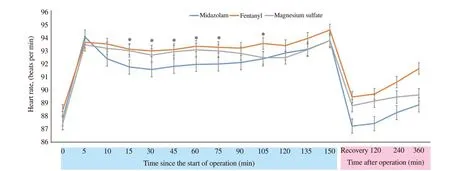
Figure 2. Changes of heart rate overtime in different groups. *: Comaprison among the three groups, P<0.05. Recovery refers to from the stop of postanesthesia care unit to the beginning of surgery.

Table 2. Comparison of sensory block.

Table 3. Comparison of motor block.

Table 4. Comparison of pain scores.
4. Discussion
This study is a double-blind trial with a projected enrollment of three stratified randomized groups of patients clinically identified as necessitating knee arthroplasty and being admitted to the Valiasr and Amir Al-Momenin hospitals, Iran, while receiving magnesium sulfate,fentanyl, and midazolam, respectively. No statistically significant intergroup difference was seen in oxygen saturation, mean blood pressure, duration of surgery, postoperative complications (such as nausea, vomiting, bradycardia, dizziness, and hypotension), and time of opioid administration. While the results demonstrated statistically significant intergroup differences in terms of heart rate at 15, 30, 45, 60,75, and 105 min after surgery, with lower in the midazolam group. The midazolam group showed a shorter time to the onset of sensory block after spinal anesthesia, sensory block to T8 or higher and sensory block to T12 and L1 (P<0.05). Besides, the three groups showed significantly in terms of onset of motor block after spinal anesthesia and time to achieve motor block to T8 or higher or Bromage score 3 (P=0.001). No significant intergroup difference was noted in pain scores among the groups (P>0.05).
As a benzodiazepine compound, midazolam acts as an effective preoperative sedative or intraoperative hypnotic agent[19]. Many animal studies have shown the analgesic effects of intrathecal benzodiazepines[19-21]. Other experimental and clinical studies have reported similar effects of intrathecal midazolam[22,23].
Chattopadhyay et al. suggested that midazolam can prolong the duration of analgesia and motor block and reduce postoperative
nausea and vomiting[2]. A study by Paleti et al. compared the efficacy of intrathecal, magnesium sulfate, and midazolam with ropivacaine 0.75% for patients with preeclampsia scheduled for elective cesarean section. They demonstrated that the onset of sensory and motor block in midazolam was faster than that of magnesium sulfate, while the duration of sensory and motor block and of analgesia in magnesium sulfate were prolonged and that intrathecal magnesium with ropivacaine prolongs the duration of analgesia without any complications[24].Similarly, the faster onset of sensory and motor block in midazolam was supported by our trial.
As shown by Katiyar et al.’s study on the efficacy of magnesium sulfate and fentanyl as adjuvants to bupivacaine for infraumbilical surgeries under the subarachnoid block, the overall reported that 100 mg magnesium sulfate or 25 μg fentanyl as adjuvants to bupivacaine provided a longer duration of analgesia, while magnesium sulfate showed better hemodynamic stability with fewer complications[14]. Our study also showed a similar result.
Another similar study compared intrathecal bupivacaine alone with intrathecal bupivacaine midazolam combination in patients undergoing elective infraumbilical surgery, concluding that midazolam prolonged the duration of analgesia and of time to motor block and reduced postoperative nausea and vomiting[2]. This is not consistent with our results where the duration of sensory block was shorter in the midazolam group. The reason for the difference could be due to differences in the drugs used in the study groups.
However, this trial showed the better effect of midazolam in comparing to the fentanyl, and magnesium sulfate with intrathecal bupivacaine on block characteristics and postoperative analgesia, but some limitations observed in our study. First, due to ethical consideration, we didn’t include a control group in this study. Moreover, the follow-up of patients after discharge did not conducted for future complications.
Midazolam could reduce the time to achieve motor block to T8 or higher, and the onset of motor block and sensory block after spinal anesthesia, as well as the time to achieve sensory block to T12 and L1 and the sensory block, developed more rapidly, while the pain did not differ among the groups. Considering the trial’s clinical findings,midazolam can be suggested, if the shorter onset of sensory and motor blocks has been considered. As the lack of complication demanding treatment implies, all the adjuvants could be suggested to be used as an adjuvant with local anesthetics, depending on the patient’s general condition and the anesthesiologist’s discretion.
Conflict of interest statement
The authors report no conflict of interest.
FundingThis article is funded by the research deputy of Arak University of Medical Sciences (No.99258).
AcknowledgmentsWe would like to extend a special debt of gratitude to the Clinical Research Councils of the Valiasr and Amir Al-Momenin Hospitals for their guidance and the research deputy of Arak University of Medical Sciences for his contributions and support throughout the development of this study.
Authors’ contributions
All authors contributed equally to this study.
猜你喜欢
杂志排行

Journal of Acute Disease的其它文章
- A rare fatal case of rabies coexisting with COVID-19
- Ophthalmovigilance in COVID-19: Retinal vascular occlusion
- Lymphocyte count and A-DROP score in COVID-19 patients: A retrospective observational study
- Knowledge, attitude, and practice of house officers towards COVID-19: A multicentered crosssectional study in Egypt
- Efficacy of propofol versus ketamine in modified electroconvulsive therapy: A prospective randomized control trial
- Sudden cardiac death in a case of Crohn's disease with COVID-19: A case report