Treatment satisfaction and medication adherence among hypertensive patients in a teaching hospital in Ekiti State,Nigeria
2022-06-30OluwaseyiAbiodunAKPORFlorenceOlutolaOLOWOLAJU
Oluwaseyi Abiodun AKPOR,Florence Olutola OLOWOLAJU
Department of Nursing Science, College of Medicine and Health Sciences, Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria
ABSTRACT
Objective:This study investigates treatment satisfaction and medication adherence among hypertensive patients attending the medical outpatient clinic of a teaching hospital in Ekiti State, Nigeria.
Materials and Methods:The study design was descriptive and cross-sectional using quantitative research strategy.A systematic sampling technique was used in selecting 270 participants; a structured questionnaire was used for data collection.Medication adherence was assessed using the 8-item Morisky Medication Adherence Scale, and treatment satisfaction was assessed using the 14-item Treatment Satisfaction Questionnaire for Medication.
Results:The study findings revealed that majority (73.7%) of the study participants had good knowledge of hypertension, while 44.4% had a good level of treatment satisfaction.Test of association of participants’ sociodemographic characteristics revealed age (χ2 = 23.773, P = 0.003)and occupation (χ2 = 21.251, P = 0.019) to be significantly associated with treatment satisfaction.The level of medication adherence by the participants was observed to be relatively poor (50.4%).The educational status (χ2 = 23.914, P = 0.001) and monthly income (χ2 = 10.406,P = 0.034) of the participants showed significant association with medication adherence.
Conclusion:The study recommends that improving patients’ understanding of their disease and treatment with subsidizing hypertensive medications by the government will enhance medication adherence.
Keywords: Hypertension, medication adherence, morbidity, mortality, outpatient clinic, treatment satisfaction
INTRODUCTION
Hypertension ranks first among the preventable causes of death worldwide.Annually, the number of patients with hypertension continues to increase in developing countries.[1,2]The prevalence of hypertension varies by ethnicity, with African-Americans having the highest prevalence at 37%.[3]Since the goal of treatment is to reduce blood pressure to the normal level, antihypertensive medications are usually prescribed in conjunction with lifestyle modification.It may, therefore, be necessary for a patient with high blood pressure to need more than one medication for effective control of blood pressure, and controlling high blood pressure is a lifelong commitment.[4-6]
Patients’ satisfaction with medication is an important measure of quality health care, as it portrays the health-care provider’s success at meeting client needs and it is a key determinant of patient’s perspective on behavioral intention.[7]Hypertensive patients must be satisfied with the treatment received so as to enhance their adherence to the treatment regimen.Iloh and Amadi[3]described treatment satisfaction as a predictor of medication adherence.Adherence is a dynamic process involving the use of the medication at the prescribed frequency and dose.Adherence to medication in hypertensive patients involves patients’ regular use of medications,adherence to the prescribed diet, and executing other lifestyle changes.Positive lifestyle changes and medication adherence significantly prevent associated complications in hypertensive patients.[4]
Adherence to treatment is a key factor in achieving successful therapeutic intervention.Poor adherence to prescribed treatment can result in serious health consequences.In order to achieve the best therapeutic outcomes among hypertensive patients, an adherence rate of 80% or more is needed.Among patients with chronic ailments like hypertension, research findings have acknowledged that approximately 50% do not take their medications as prescribed.This poor adherence to medication leads to increased morbidity and death.[2,8]
Adherence to the medication among hypertensive patients has become a major challenge in Nigeria and other developing countries, leading to serious complications of hypertension.[9]Iloh and Amadi[3]equally stated that treatments satisfaction among hypertensive patients is likewise a significant challenge among Nigerians, which has affected medication adherence.It is also stated that treatment satisfaction and good medication adherence can decrease cardiovascular-related morbidity and mortality rate among hypertensive patients.[3]Some reported factors that determine the level of medication adherence by patients include the length of medication period, side effects of medicines, the complexity of the treatment, communication between patient and doctor,patient satisfaction with health-care system, socio-economic factors, education, and cost of treatment.[9]Therefore, lack of treatment satisfaction among hypertensive patients with poor adherence to their medications could be the major reason for the increased rate of hypertensive complications in the previous years.Hence, this study investigated treatment satisfaction and medication adherence among hypertensive patients attending the medical outpatient clinic of a teaching hospital in Ekiti State, Nigeria.
MATERIALS AND METHODS
Research design and setting
A descriptive design was employed using a quantitative approach to determine the treatment satisfaction and medication adherence of hypertensive patients.The study was carried out at the medical outpatient clinic of a teaching hospital in Ekiti State.Ekiti State is situated within the tropics in the southwest region of Nigeria, consisting of 16 local government councils.The hospital is a tertiary health institution that caters for the secondary and tertiary health needs of Ekiti people and neighboring states in the southwestern part of the country.
Target population
The target population for this study were adult male and female hypertensive outpatients of the hospital who attended the hypertensive clinic for at least 6 months.Hypertensive outpatients’ clinic holds every Wednesday with an average population of 80 patients per visit.Based on the hospital clinic records, a sample size of 270 was used for the study using the Taro Yamane sample size calculation.
Inclusion criteria
The inclusion criteria for this study include being male or female adult patients; attending the medical outpatient clinic at the study setting; being diagnosed with hypertension for at least 6 months; and gave informed verbal and written consent to participate in the study.
Exclusion criteria
The exclusion criteria include aged <18 years; diagnosis not up to 6 months; and those who did not consent to participate in the study.
Sampling technique
This study utilized a systematic sampling technique that involved four stages.In Stage 1, the patients in the outpatient clinic register were numbered from 1 to 2625.In Stage 2, a sampling interval was obtained by dividing the population of patients on the register (2625) by the required sample size (270) to obtain approximately ten patients.In Stage 3, a random start was selected between 1 and 10 by balloting.In Stage 4, 270 respondents were finally taken by selecting every tenth patient on the numbered register.
Instrument for data collection
A well-structured adapted questionnaire was used for data collection.The items of the questionnaire were based on information adopted from previous publications[3,10]and other relevant literature search; hence, modifications of the items were made in order to meet the objectives of the study.The questionnaire consisted of six sections: Section A is the demographic profile of the participants; Section B examined the knowledge of hypertensive patients; Section C addressed questions on treatment satisfaction; Section D assessed medication adherence among hypertensive patients;and Section E identified barriers to medication adherence.The questionnaire comprised 41 questions that answered relevant questions relating to the study.
Data management and statistical analysis
IBM SPSS Statistics 20.0 (IBM Corp., Armonk, New York, USA.)was used for data analysis.Social demography characteristics were evaluated as frequencies and percentages (%).Knowledge of hypertension was scored with 1 for a correct response and 0 for an incorrect response.Treatment satisfaction was scored with 0 for “not satisfied,” 1 for “partially satisfied,”2 for “satisfied,” and 3 for “very satisfied.” The medication adherence level was scored with 0 for “strongly disagree and disagree,” 1 for “agree,” and 2 for “strongly agree.” The total scores for these variables were separately calculated based on their aforementioned categories using descriptive statistics.Tests of the relationship were carried out using Chi-square analysis.All analyses were at a probability level of 0.05.
For knowledge level, a participant whose cumulative score for knowledge category ranged from 0 to 10 (poor knowledge), 11 to 14 (moderate knowledge), and 15 to 19 (good knowledge).For adherence level, a participant whose cumulative score for adherence category ranged from 0 to 13, 14 to 20, and 21 to 27 was regarded as having poor adherence, moderate adherence, and good adherence, respectively.In the case of treatment satisfaction level, the cumulative scores of 0-11,12-16, and 17-21 for the treatment satisfaction category were regarded as poor satisfaction, moderate satisfaction,and good satisfaction, respectively.For barriers to medication and adherence, cumulative scores of 1-5, 6-8, and 9-12 for the barrier category were regarded as minor, moderate, and severe barriers, respectively.
Ethical considerations
Before commencement of the study, the research proposal was submitted to the Research and Ethics Committee of the Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria, and approval was obtained on the May 25th,2021, with protocol number EKSUTH/A67/2021/05/003.Participants’ rights to full disclosure and self-determination were explained, they were informed about the nature of the study and what findings needed to be obtained, and thus,informed consent was obtained.Participants were informed that they had the right to choose voluntarily if they wanted to participate in the research or terminate their participation to ensure self-determination.To ensure confidentiality and anonymity, the names of the respondents or any form of identity were not be required on the questionnaire.
RESULTS
Participants’ sociodemographic characteristics
Almost half (45.6%) of the participants were above the age of 51 years and 63% were females.Majority (68.1%) were married, while 14.2% were widowed; 68.8% of the participants had tertiary education, while 8.9% had no formal education.Almost half (48.5) of the participants were public servants,with 48.5% earning more than 50,000 Naira Nigerian currency (more than $100) monthly.
Participants’ knowledge level of hypertension
In general, participants’ knowledge level of hypertension showed that majority of the participants (199 [73.7%])had good knowledge, 65 (24.1%) of them had moderate knowledge, while only 6 (2.2%) of them had poor knowledge.Sociodemographic distribution of participants with the highest number with good knowledge of the disease showed that they were in the age range of 51-60 years (57),female (128), married (142), Christians (165), had tertiary education (127), received monthly income greater than N 50,000 (105), public servants (102), and had been diagnosed of the disease for more than 2 years [Table 1].
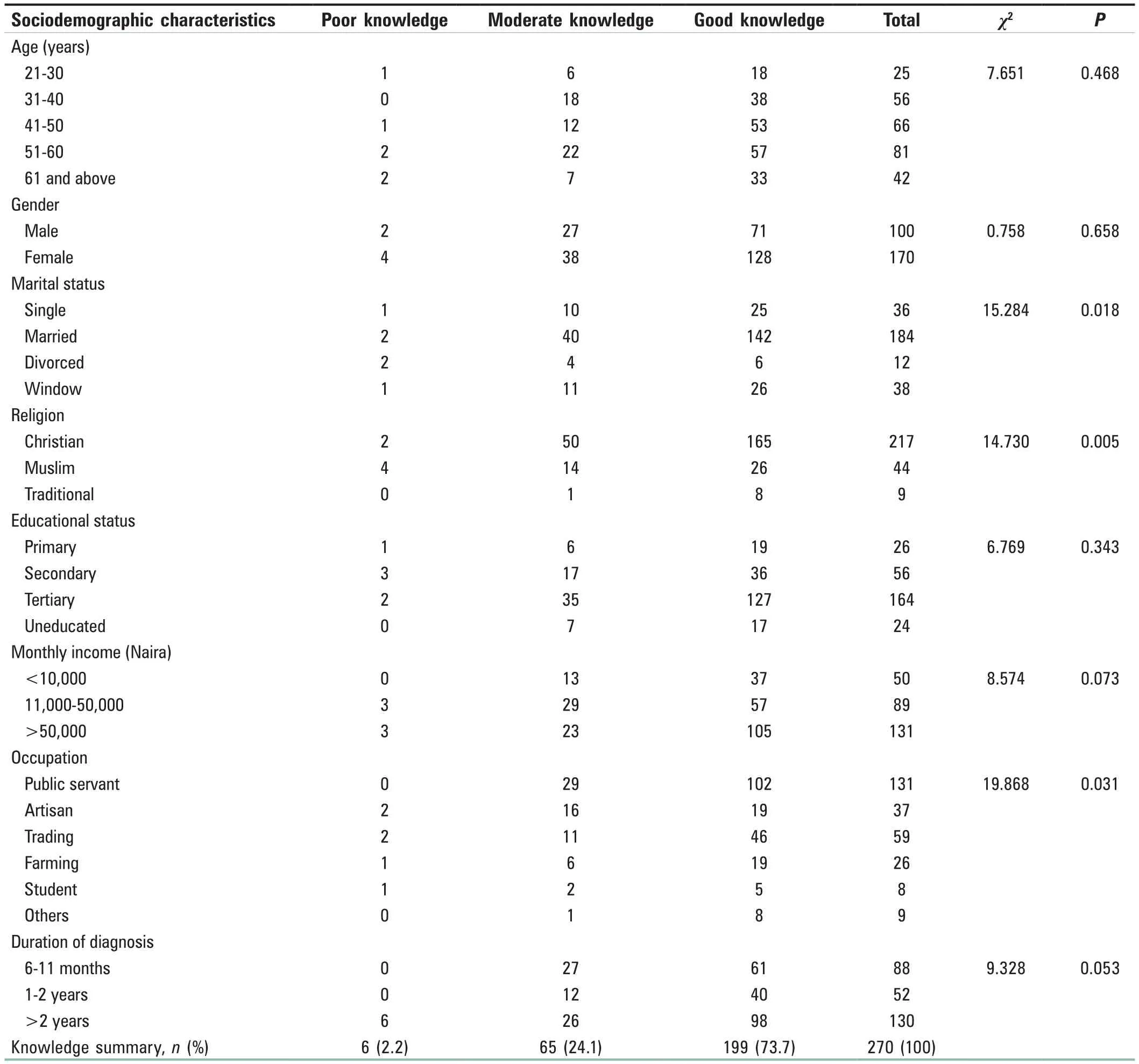
Table 1: Knowledge level distribution of the participants (n=270)
Out of the sociodemographic characteristics of the participants, only religion (χ2= 14.730,P= 0.005), marital status (χ2= 15.284,P= 0.018), and occupation (χ2= 19.868,P= 0.031) were observed to be significantly associated with the participants’ knowledge level of the disease [Table 1].
Participants’ level of treatment satisfaction
The treatment satisfaction level of the participants revealed that 44.4% had good satisfaction, 38.5% had moderate satisfaction, and 17.1% had poor satisfaction.Out of the total number of participants who experienced good treatment satisfaction, the highest number of them were aged 51-60 years (44), 74 were female, 86 were married, 94 were Christians, 63 of them had tertiary education level, 54 were public servants, and 51 of them had been diagnosed of hypertension for over 2 years [Table 2].
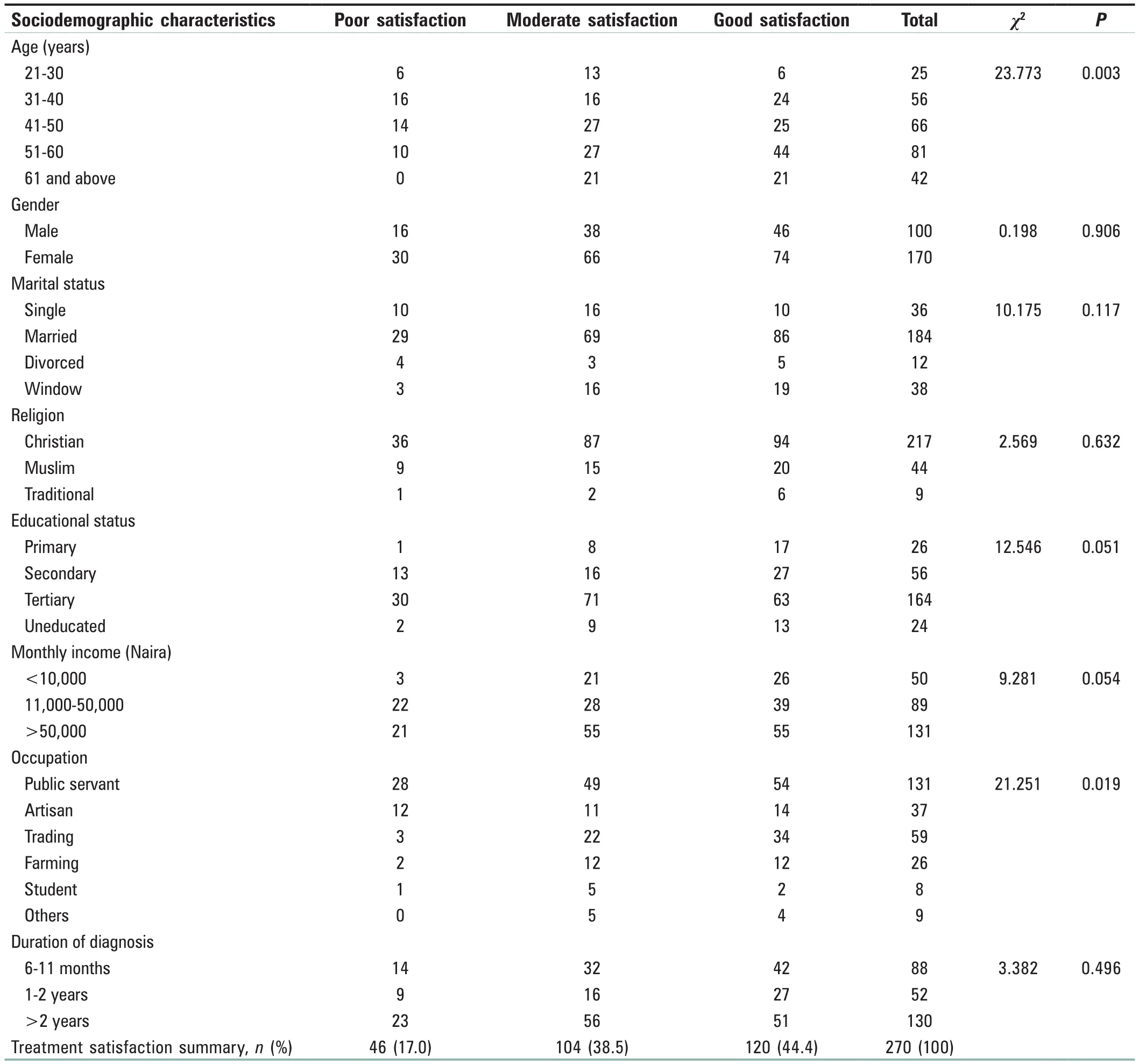
Table 2: Level of treatment satisfaction of the participants (n=270)
Participants’ level of adherence to medication
With respect to the level of adherence to medication by the participants, only 9.3% showed good adherence, while half (50.4%) of the participants showed poor and 40.4% had moderate adherence to medication.Of the number of participants that showed poor adherence to medication,41 were in the age range of 41-50 years, 86 were female,96 were married, 113 were Christians, 99 of them had a tertiary level of education, 74 received monthly income that was greater than N 50,000, 86 were public servants, and 69 had been diagnosed of the disease for over 2 years [Table 3].
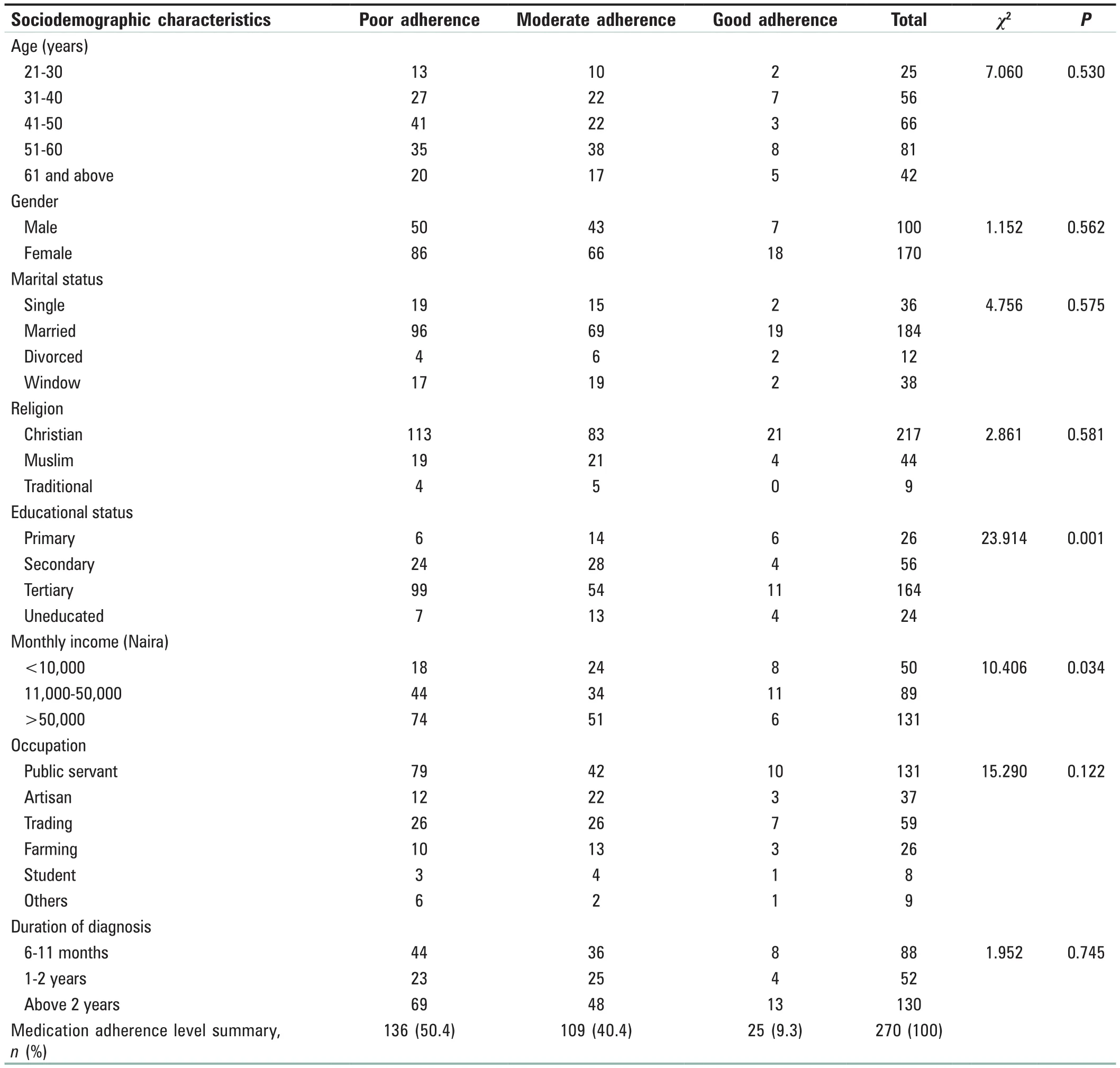
Table 3: Medication adherence level of the participants (n=270)
Only educational status (χ2= 23.914,P= 0.001) and monthly income (χ2= 10.406,P= 0.034) of the participants’sociodemographic characteristics showed significant association with adherence to treatment [Table 3].
Barriers to medication adherence
Barriers to medication adherence included the cost of medication, fear of side effects, multiple medications,and lack of information.Cumulative scores of 1-5, 6-8,and 9-12 for barrier category were regarded as minor,moderate, and severe barriers, respectively.Majority of the participants were observed to report either minor (39.9%)or moderate (46.7) barriers, while 13.7% were severe.Out of the participants whose barriers to medication were considered minor, the highest number of them were in the age range of 41.50 years (34), females (63), married (78),Christians (92), had educational up to tertiary level (74),had monthly income higher than N 50,000 (61), public servants (57), and 59 of them had their diagnosis for over 2 years [Table 4].

Table 4: Barriers to medication adherence (n=270)
Apart from age (χ2= 15.885,P= 0.044) and duration of diagnosis (χ2= 11.681,P= 0.020), no other sociodemographic characteristics of the participants was significantly associated with barriers to medical adherence [Table 4].
DISCUSSION
This study revealed a high knowledge level of hypertension among the study participants.This finding is in line with a similar study conducted by Ralapanawaetal.,[10]where more than two-thirds of the study participants had adequate knowledge of hypertension.In addition, this present study showed that there is no significant relationship between patients’ knowledge and medication adherence.This finding was at variance with a similar study conducted by Jankowska-Polańskaetal.,[11]where knowledge and medication adherence showed a significant relationship.Similarly, the finding was at variance with another similar study conducted in Spain by Estradaeta.,[12]where majority of the participants had poor knowledge of hypertension.Good knowledge with poor medication adherence among patients was consistent with the findings of Pirasathetal.[13]from a tertiary care center in Northern Sri Lanka, where the participants’ knowledge of hypertension was good, but their adherence to medication was poor.Majority of the participants in this study showed either poor or moderate adherence to treatment.
The level of treatment satisfaction among the respondents in this study was very good, with 82.9% having a high level of treatment satisfaction.Patient satisfaction is an important and commonly used indicator for measuring the quality of health care.One of the key elements used to capture the global impression of patients is perceived benefit and satisfaction with treatment.[14]This suggests that the high level of treatment satisfaction among the participants was a result of the perceived benefit seen in the treatment given to them.Despite the good treatment satisfaction observed in this study,adherence to medication was relatively poor or moderate,with only a small percentage of the participants observed to have good adherence.This finding is at variance with the results of a similar study by Ajayietal.,[15]where treatment satisfaction independently increases medication adherence.
A patient’s satisfaction with medication is said to be an important measure of health-care quality since it offers information on a provider’s success at meeting the needs of a client, hence is regarded as an important determinant of patient’s perspective on behavioral intention.[7]To ensure adherence to treatment medication, hypertensive patients must be satisfied with the treatment given.Iloh and Amadi[3]described treatment satisfaction as a predictor of medication adherence.
This study showed that only 9.3% of the participants had a good adherence level to medication.This finding is in contrast with a similar study conducted in Nigeria, where the level of medication adherence of the study participants was on average (50.7%).[7]Patients’ adherence to medication is likely to be inadequate, especially when the patient lacks important knowledge about the disease and its outcome.However when knowledge is improved, there is likely to be an improved adherence to medication.
Furthermore, Saartietal.[2]found a positive association between treatment satisfaction and medication adherence in a study conducted among hypertensive patients in Palestine.Treatment satisfaction is a vital determinant of patient’s general health-related choices such as adherence and readiness to continue with their treatment regimen.[3,16]According to Zyoudetal.,[17]the concepts of medication adherence and treatment satisfaction are commonly used to assess patient care and treatment outcomes, and usually, a positive association is expected between these concepts.However, in this study, treatment satisfaction among the participants was high but with poor medication adherence.This may be because a long-term illness such as hypertension makes medication adherence difficult for the patients since patients are expected to take this medication for life.[18]Adherence to the medication among hypertensive patients has also become a major challenge in Nigeria and other developing countries.[9]Although, Iloh and Amadi[3]in their study conducted in Nigeria, revealed that treatments satisfaction among hypertensive patients was a major challenge, resulting in poor medication adherence, this finding was at variance with this study, as the high level of patient satisfaction does not positively influence patient medication adherence.In patients with chronic illness such as hypertension, studies have shown that roughly 50% of patients do not take their medications as prescribed.[2]
As found in this study, the parameters which significantly predict the participants’ medication adherence were educational level and income, while age and occupation predicted treatment satisfaction of the participants.The relationship of the participants’ education and income status with their medication adherence is in line with a similar study conducted among hypertensive patients by Shietal.[19]which also showed a significant association between patients’ educational status and income with medication adherence.Similarly, Mohamedetal.[9]acknowledged some factors that determine patient’s medication adherence such as the duration of medication, side effects, the intricacy of the treatment, communication between patients and health-care providers, patient satisfaction with care provided, financial status and educational level, as well as the cost of treatment.According to the present study,individuals with higher income and education were more likely to adhere to the use of antihypertensive agents.This may be related to the high consciousness of medication benefits and the availability of funds to procure their medications.
CONCLUSION
The findings of this study revealed that the level of knowledge of the respondents about hypertension and its treatment regimen was good.The treatment satisfaction level of the study participants was good, but their adherence to treatment medication was relatively poor.The study further revealed that barriers to medication adherence by the participants were either minor or moderate.These study findings could be useful in the care of hypertensive patients, especially during early treatment, at a point where improving medication adherence and treatment satisfaction is still possible.Hence,it is vital that nurses and other health-care providers assist in improving patients understanding of their disease and treatment through continuous health education.Similarly,subsidizing hypertensive medications by the government will definitely enhance medication adherence since monthly income had been established to be a determining factor in the study.
Acknowledgments
The authors are grateful to the Research Ethics Committee of the Ekiti State Teaching Hospital, Ado-Ekiti, Nigeria, for approval granted to carry out the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
