Pneumonia and seizures due to hypereosinophilic syndrome—organ damage and eosinophilia without synchronisation: A case report
2022-06-27TetsuroIshidaTomonoriMurayamaSeijuKobayashi
lNTRODUCTlON
Hypereosinophilic syndrome (HES) is a marked blood and tissue eosinophilia of unknown aetiology with a variety of clinical manifestations. Since 1975, the disease has been defined by three criteria: (1)Blood eosinophilia ≥ 1500/mmfor longer than 6 mo (or death before 6 mo associated with signs and symptoms of hypereosinophilic disease); (2) Lack of evidence for parasitic, allergic, or other known causes of eosinophilia; and (3) Presumptive signs of organ involvement, such as heart failure,gastrointestinal dysfunction, central nervous system abnormalities, fever, or weight loss[1].
However, there are several problems with these criteria. First, according to these criteria, clinicians must wait 6 mo to diagnose a patient with multiple organ involvement. Second, an increase in eosinophils does not necessarily correlate with organ damage. Some patients may have a marked increase in eosinophils but only mild symptoms, while others may have a mild increase in eosinophils but significant organ damage[2]. Therefore, two diagnostic criteria have now been proposed to replace the classic three: (1) Blood eosinophilia of greater than 1500/mmon at least two occasions or evidence of prominent tissue eosinophilia associated with symptoms and marked blood eosinophilia; and (2)Exclusion of secondary causes of eosinophilia, such as parasitic or viral infections, allergic diseases,drug-induced or chemical-induced eosinophilia, hypoadrenalism, and neoplasia[3]. However, this revision of the diagnostic criteria does not solve all the problems in the diagnosis and treatment of HES.We anticipate that this case will aid in the diagnosis and treatment of similar cases.
CASE PRESENTATlON
Chief complaints
The patient had no chronic illnesses such as hypertension, diabetes, or asthma, and no history of cancer.She was a non-smoker and did not habitually drink alcohol. She had a well-balanced diet and lived a healthy lifestyle.
History of present illness
Her respiratory distress started during the night 1 d before presentation. It improved after 1 h and was still mild over the next morning and evening hours. However, 22 h later, her symptom got worse again during the night.
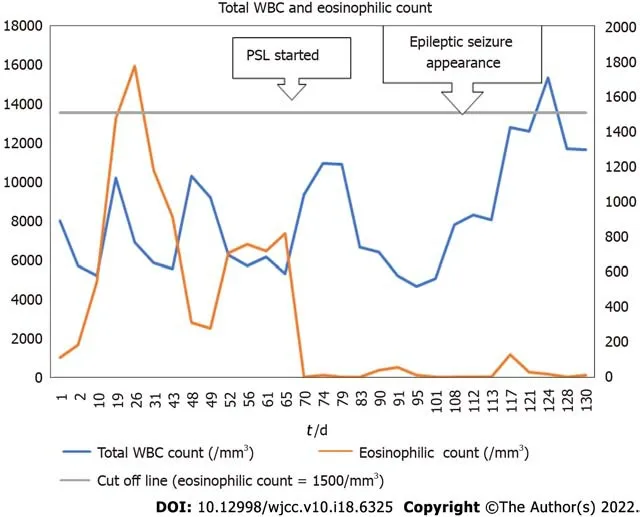
On day 1, her rapid antigen tests using a throat swab were negative for influenza A and B and COVID-19. Her electrocardiogram (ECG) showed no abnormalities on admission and on loss of consciousness on day 108. In her blood analyses, there were no abnormalities in the electrolyte, glucose, lipid, liver function, and renal function parameters. The antinuclear antibody (ANA) titre at 1:40 serum dilution was positive but staining patterns at 1:40 serum dilution was negative for homogeneous, discrete speckled, speckled, nucleolar, and peripheral staining. Anti-neutrophil cytoplasmic antibody (ANCA)and HIV tests were negative. On day 32, the patient’s IgE level was slightly high at 237 IU/mL (normal:27.54-138.34), but her IgG, IgA, and IgM levels were normal. Blood analyses also showed that eosinophils and brain natriuretic peptide (BNP) levels were high. The highest values for each were 1760/mmon day 26 for eosinophils and 738.1 pg/mL on day 1 for BNP (Figures 1 and 2). The blood and sputum taken on day 26 were negative on culture for bacteria or fungi and no parasites were found.However, on day 109, blood culture was positive for methicillin-resistant Staphylococcus epidermidis,and the β-D-glucan level was high (316.0 pg/mL). On day 128, blood tests showed normal levels of ammonia. The patient’s post-consciousness EEG showed spikes and waves in Fp1, F1, C3, P3, and O1(Figure 3). Her echocardiogram showed no thrombi in the atria or ventricles.
History of past illness
A 94-year-old Asian woman presented to our hospital for dyspnoea and wet cough. She also had abdominal pain and bloody stools. She was admitted to our hospital with a diagnosis of heart failure and sigmoid colon ulceration (day 1).
Personal and family history
There was no specific history.
Physical examination
当前,我国正在大力倡导绿色理念。因此,在果树的防虫治虫的过程当中,同样可以将绿色理念融入其中。绿色防治方式在果树病虫害防治中的应用,不但可以对病虫害进行有效的防治,而且对周边环境起到环保的作用。基于此,果树管理人员需要当期对果园进行清理,例如果园当中的杂草、枯萎的树木、落叶等进行及时的清理,并将此部分的废弃物采取火烧的方式进行处理。不仅可以将病虫害进行消除,而且还极大的保持了果园的清洁度。
Laboratory examinations
菌株:伤寒沙门菌GIFU 10007(野生株,WT),rpoE缺陷株(ΔrpoE), rpoS缺陷株(ΔrpoS),RNase E缺陷株(Δrne),RNase III缺陷株(Δrnc)由本实验室保存,缺陷株使用自杀质粒法制备.asrC启动子缺陷株(ΔPasrC),WT+pBAD(WT含pBAD/gIII),WT+pBAD-asrC(WT含pBAD-asrC)由本实验室制备[18].
The patient was 148 cm tall, weighed 42 kg, and her vital signs were as follows: blood pressure 111/43 mmHg; pulse 90/min; respiratory rate 14/min; and SpO98% (room air). On chest auscultation, her heart rhythm was regular and no heart murmur was found. However, auscultation of respiratory sounds found wheezing. Her abdomen was flat and soft and abdominal auscultation found neither increased nor decreased intestinal peristalsis. There was no rebound tenderness or abdominal guarding.However, there was intermittent and spontaneous abdominal pain and bloody stools. Her eyelid conjunctiva did not show jaundice or pallor. Her oral and nasal cavities and skin surfaces showed no abnormal findings. Her upper limbs showed no abnormalities. However, her lower extremities showed indurated oedema.
Imaging examinations
Non-contrast computed tomography imaging of the patient’s chest showed bilateral pleural effusions and infiltrative shadows (Figure 4). Her gastrointestinal endoscopy showed multiple ulcers in the sigmoid colon (Figure 5). Histopathological examination showed colonic gland prolapse, vitrification of the stroma, and an infiltration of inflammatory cells, but no evidence of malignant transformation. Noncontrast magnetic resonance imaging of the patient’s head showed extensive periventricular hyperintensity (Figure 6).
MULTlDlSClPLlNARY EXPERT CONSULTATlON
Norihisa Okuda MD, Vice-president and Chief, Department of Respiratory Medicine, Hokujinkai Ishibashi Hospital
The patient’s eosinophils in the blood tests exceeded 1500/mmonly once, but she had high eosinophils multiple times without meeting this threshold. Additionally, it was clear that the eosinophilic infiltrate was causing serious damage to the nervous, respiratory, cardiovascular, and digestive systems. We should not have delayed the initiation of her treatment any longer to meet the classical diagnostic criteria. Biopsies of organs other than her sigmoid colon were considered for a more precise examination and imatinib initiation was considered for more effective treatment, but both were too invasive for the elderly patient. Given that she and her family did not wish to undergo these tests and treatments, we did not pursue these options. Although Japan is a country with some of the richest medical resources in the world, the hospital where the patient was admitted had no intensive care unit or specialists in collagen diseases and autoimmune diseases, and the same is true for other similar rural hospitals. The use of limited medical resources is an important issue in this country as in the rest of the world.
FlNAL DlAGNOSlS
The patient was diagnosed with epileptic seizures and pneumonia caused by HES.
洞庭湖湿地旅游开发起步晚,已有产品单一,以传统的湖区风光参观为主,针对特色湖湘文化产品开发稀少,游客体验感欠佳。其湖区中部旅游景观产品十分单调,无层次立体感,连唯一有特色的旅游项目——观鸟,时空制约明显。

TREATMENT
In addition to rehabilitation, the patient was treated with furosemide for heart failure, ceftazidime and vancomycin and fungard and PSL for pneumonia and levetiracetam (LEV) for seizures.
OUTCOME AND FOLLOW-UP


Ishida T was the patient's primary care physician and contributed to the literature review and manuscript preparation; Murayama T and Kobayashi S reviewed the literature and contributed to the preparation of the manuscript; and All authors gave their approval for the final version to be submitted.
This study was conducted at Iwanai Kyokai Hospital (209-2, Aza-Takadai, Iwanai-cho, Iwanai-gun,Hokkaido 045-0013, Japan). We are grateful to the patient who gave her consent to take part in this study. We would also like to thank Dr. Kawasaki, Dr. Yamazaki, and Dr. Kuroda in the Department of Internal Medicine at Iwanai Kyokai Hospital for their help and support. We thank Leah Cannon, PhD,from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
DlSCUSSlON


First, we will discuss diagnosis of HES. As mentioned at the beginning of this report, the diagnostic requirement for HES is a blood eosinophil count ≥ 1500/mmfor at least 6 mo according to the classical diagnostic criteria or measured at least twice according to the diagnostic criteria proposed by Simon[3]. In this case, neither of these criteria were met at the time the diagnosis was made. In our case, the patient’s blood eosinophil count exceeded 1500/mmonly once and this did not necessarily coincide with the most severe period of organ damage. Some clinicians suggested that we should have waited until her eosinophil count had risen again and her symptoms had worsened before deciding on a diagnosis. However, as stated in the Multidisciplinary Expert Consultation, we needed to start her treatment as soon as possible. This was considered a higher priority than meeting the strict diagnostic criteria. In addition, the disease course in this case meets the criterion of "or death before 6 mo associated with signs and symptoms of hypereosinophilic disease" listed in the supplementary information in the classical criteria[3]. Heart failure, sigmoid colon ulceration, pneumonia, and epilepsy signified damage to each of these organs in our patient. Therefore, the diagnosis of HES in this case was appropriate. With regard to treatment, the focus is on PSL. As is well known, PSL is a drug that needs to be tapered off, not stopped abruptly. Furthermore, a longer PSL treatment course is commonly required for eosinophilic pneumonia. However, in this case, given the early decline in the eosinophil count after initiation of PSL therapy, perhaps it should have been tapered or stopped earlier.
定理 2.3 设X={x1,x2,…,xr},→是[0,1]上的正则蕴涵算子。对任意的a,[0,1], a+a→b≤1+b。若([0,1],ρ)完备,则(F(X),H)完备。
Next, we would like to discuss the diagnosis and treatment of epilepsy. Common causes of loss of consciousness in older people include heart disease, autonomic disorders, other conditions such as anaemia, ischaemia and varicose veins, or anticholinergic drugs[5]. Our patient had congestive heart failure at the time of admission, but her condition improved. She did not have any blood clots identified that could have caused cerebral embolism. Her vital signs, including blood pressure and ECG, were normal. Therefore, it was considered unlikely that the loss of consciousness was due to circulatory problems. Her post-consciousness electroencephalogram (EEG) suggested that there were epileptic discharges around the left anterior frontal lobe, motor cortex, central sulcus, sensory cortex, and visual cortex. The rather unremarkable EEG findings compared with the clinical findings may be because this EEG was done after the LEV treatment was started. The epileptic discharges may have been more intense before the administration of antiepileptic drugs. We were not able to do rapid or continuous monitoring EEG at our hospital. In diagnosing and treating her epilepsy, we were forced to prioritise life-saving treatment over rigorous diagnosis.
Regarding the seizure type, her epilepsy was most likely a complex partial seizure. Complex partial seizures are more likely to occur in older adults and cause disorientation, but they do not cause tonic or clonic seizures[6]. The fact that LEV treatment was effective in preventing the seizure symptoms was also one of the reasons for the diagnosis. However, the presence of eyelid twitching also suggests that her seizure type may have been absence seizures. Absence seizures are generally more common in young children and have a shorter duration of disorientation. However, if the seizure is an atypical absence seizure, the disturbance of consciousness may be prolonged. In Japan, LEV may be administered at doses of up to 3000 mg/d. However, in this case, the patient was elderly, and it was feared that increasing the dose of LEV might cause side effects such as malignant syndrome. The LEV dose was not increased because there were no obvious epileptic seizures after the start of LEV at a dose of 1000 mg/d. In this case, the patient’s loss of consciousness was prolonged even after an intramuscular injection of 10 mg diazepam and was, therefore, considered to be benzodiazepine-refractory.LEV, fosphenytoin, and valproic acid are suitable for the treatment of epilepsy which does not improve with benzodiazepines. In elderly patients, there is no difference in the safety or therapeutic efficacy between these three drugs[7]. LEV was chosen in this case because it can be started intravenously and can be seamlessly transferred to the oral route if oral medication becomes available later. We considered hepatic encephalopathy as a possible cause of our patient’s impaired consciousness, but this was ruled out by the normal blood ammonia levels and the fact that the EEG showed no triphasic waves.
随钻电磁波电阻率测井理论分析……………………………………………………………………………张立山,修 华(3.15)
While all ANA staining patterns were negative, the ANA titre was positive at 1:40 dilution. This result indicates that our patient may have had a collagen disease. Therefore, we needed to differentiate the collagen diseases with eosinophilia granulomatosis with polyangiitis (EPGA) and polyarteritis nodosa (PAN), from HES. EPGA, formerly known as Churg-Strauss syndrome, is characterised by asthma, eosinophilia of the blood and tissues, and small vessel vasculitis. The clinical symptoms are variable but can be divided into two main subtypes: The "vasculitis" type, which is positive for ANCA and shows glomerulonephritis, purpura, and inflammation of multiple peripheral nerves. The other is the "eosinophilic" type, which is negative for ANCA but is characterised by a markedly high level of eosinophils and damage in the lungs and myocardium[8]. This case is similar to the "eosinophilic" type,but EPGA is less likely to cause central nervous system damage such as seizures.
PAN is a vasculitis that targets medium-sized arteries and leads to multi-organ failure. The target organs include the heart and the gastrointestinal tract. We note that damage to the central nervous system has also been reported[9]. However, damage to the lungs has rarely been reported[10]. The present case is not typical but is similar to both EPGA and PAN. However, the pathological findings in the sigmoid colon did not show the features of either of these diseases.
而这又引起一个学界经常讨论的“磨洋工”问题。那到底有没有人偷懒、怠工呢?笔者就此问题进行了访问:答1:在生产队做工,不会有多卖力,除了包工。我们这边一般都有脱粒机打谷,因为我们这里人少田多,基本上都是包工。做集体工,有时肯定会拖拉点的,不会很卖力,只是普普通通去做。包工了大家就卖力了。(LXH170509[注]引文后为访谈记录编号。大写的英文字母为访谈对象姓名的首字母,“170509”表示此访谈于2017年5月9日做的。引言括号内容为笔者所加。下同。 )答2:没有什么偷懒的。工也做,就是慢一点。(LQJ170709)答3:有些人啊,(现在)请别人做工,也有个别比较懒点。(XJD170707)
从表1可以看出,双氧水脱硫技术可以适应较高烟温、较大气量、不同二氧化硫浓度的烟气治理,具有流程简单、脱硫效率高、运行费用低,可以减少二次污染等优点。因此本文主要探索双氧水脱硫在电解铝烟气治理用的应用。
In terms of brain imaging findings, the differential diagnosis in this case also includes cerebral amyloid angiopathy (CAA). The Modified Boston Criteria for CAA are based on imaging and pathological findings. The disease can be classified as: (1) Definite CAA; (2) Probable CAA with supporting pathology; (3) Probable CAA; and (4) Possible CAA. The novelty of this criteria is that (3)and (4) do not require a pathological examination[11]. In this case, at the request of the patient and her family, no pathological examination of the brain tissue was performed after her death. Generally, the hallmark of CAA on brain imaging is multiple sporadic lesions confined to the cerebral cortex, corticosubcortical junction grey matter, and subcortical white matter. However, some subtypes of CAA, such as cerebral amyloid angiopathy-related inflammation (CAA-ri), present with mass-like lesions as in this case[12]. CAA-ri is known to respond well to treatment with steroids and immunosuppressive drugs. In this case, treatment was given with the expectation that the patient might be diagnosed with CAA-ri.There is a report that CAA-ri can cause seizures[13], which seems to be consistent with the symptoms in this case. However, there are no previous studies on its frequency. Similar cases need to be studied in the future.
CONCLUSlON
HES can cause damage to many organs and has an undulating disease course. Therefore, HES must be differentiated from other diseases such as EPGA, PAN, and CAA. In this case, the diagnosis was more difficult because of the time lag between the various clinical symptoms and the eosinophilia. The focus of treatment was to determine the appropriate dose and duration of PSL and LEV therapy. We conclude that this case report can be used as a reference for the diagnosis and treatment of similar cases.
ACKNOWLEDGEMENTS
中医有时以毒攻毒会使用毒性药材,含有毒性药材的中成药应该在中医师的指导下使用,不能自行服用,并且需要注意药物的相互作用,中药常见毒性药材如下:马钱子、白附子、附子、半夏、天南星、巴豆霜、山豆根、北豆根、吴茱萸、苦杏仁、苦楝皮、牵牛子、猪牙皂、罂粟壳、贯众、制川乌、鹤虱、川楝子、重楼、雄黄、朱砂、全蝎、蟾酥、蜈蚣。
FOOTNOTES
Furosemide 20 mg/d for 10 d from the day of admission (day 1) relieved her congestive heart failure symptoms for a period of time. A diet suitable for digestion and absorption made her bloody stools and abdominal pain disappear. Rehabilitation, including gait training and flexibility exercises to prevent loss of range of motion and contractures throughout the body, was also initiated. However, from day 56, her congestive heart failure symptoms recurred, and pneumonia also appeared. Treatment with 20 mg/d furosemide was restarted from that day, but without effect. Ceftazidime 2 g/d was also ineffective in treating the pneumonia. On day 68, the patient was diagnosed with HES and treatment with prednisolone (PSL) 25 mg/d was started. After that, the pneumonia and heart failure symptoms gradually improved, so the PSL was gradually reduced to 15 mg/d. Her rehabilitation was also resumed.However, on day 108, her eyes suddenly rolled upwards, and she showed eyelid twitching and loss of consciousness. Her breathing stopped and her SpOdropped to 70% (room air). Oxygen therapy(reservoir mask: 10 L/min) was started immediately. Diazepam 10 mg intramuscular injection was also given and after 5 minutes her SpOimproved to 90% (reservoir mask: 10 L/min) and her seizures stopped. LEV 1000 mg/d was started and subsequently, the seizures did not recur. However, her state of consciousness continued to be unfavourable on the Glasgow Coma Scale, E2 V2 M4[4]. Her respiratory status also improved reaching SpO90% (nasal cannula: O1L), but not higher. On day 109,fungard 50 mg/d, vancomycin 1 g/d and ceftazidime 2 g/d were started and her PSL was increased to 30 mg/d. However, her pneumonia continued to worsen, and she died of pneumonia on day 135.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflicts of interest.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Japan
Tetsuro Ishida 0000-0002-8513-2373; Tomonori Murayama 0000-0003-2371-8421; Seiju Kobayashi 0000-0002-1557-1426.
Ma YJ
A
Ma YJ
猜你喜欢
杂志排行

World Journal of Clinical Cases的其它文章
- Stem cells as an option for the treatment of COVID-19
- Development of clustered regularly interspaced short palindromic repeats/CRISPR-associated technology for potential clinical applications
- Prostate sclerosing adenopathy: A clinicopathological and immunohistochemical study of twelve patients
- Effectiveness and postoperative rehabilitation of one-stage combined anterior-posterior surgery for severe thoracolumbar fractures with spinal cord injury
- Construction and validation of a novel prediction system for detection of overall survival in lung cancer patients
- Identification of potential key molecules and signaling pathways for psoriasis based on weighted gene coexpression network analysis