Mixed porokeratosis with a novel mevalonate kinase gene mutation:A case report
2022-06-23HongJunXuGuangDongWen
lNTRODUCTlON
Porokeratosis is a rare, acquired, or inherited disorder of keratinization, which presents as a keratotic papule or plaque with an annular ridge-like border[1]. Its main histological characteristic is a cornoid lamella, a thin column of parakeratosis leading to a ridge-like hyperkeratotic border. Numerous types of porokeratosis have been described and there are reports of more than one type of porokeratosis developing in the same patient and in multiple members of an affected family[2]. Inherited or sporadic genetic defects have an important role in porokeratosis. Correlations between gene mutations and clinical phenotypes of porokeratosis have been reported previously[3]. Porokeratosis lesions may alter a patient’s appearance or function. Furthermore, some cases develop squamous cell carcinoma within the porokeratosis lesions. Currently, no therapeutic interventions with good efficacy are available although various topical, surgical, destructive, and systemic therapies appear to be effective in some patients. Here, we report a rare case of disseminated superficial actinic porokeratosis (DSAP) and porokeratosis ptychotropica (Ppt) associated with a mevalonate kinase (MVK) gene mutation which was successfully treated by surgery.
CASE PRESENTATlON
Chief complaints
A 45-year-old man complained of long-standing skin lesions.
History of present illness
The lesions started as brown patches on his face and gradually spread to the trunk and extremities with verrucous plaques 30 years ago. Involvement of the scrotum occurred 20 years ago.
History of past illness
The patient had no medical history and reported no history of ultraviolet exposure, immunosuppression, or immunodeficiency caused by human immunodeficiency virus (HIV) infection, tumors, or drugs.
Personal and family history
The patient’s father and one of his brothers had similar lesions for years.
Physical examination
Porokeratosis represents a heterogeneous group of hereditary and acquired disorders of the clonal hyperproliferation of keratinocytes[4]. The characteristic ridge-like, keratotic border termed the “cornoid lamella” confirms the diagnosis of porokeratosis. Several clinical variants of porokeratosis have been described, all of which share this distinctive feature.

Laboratory examinations
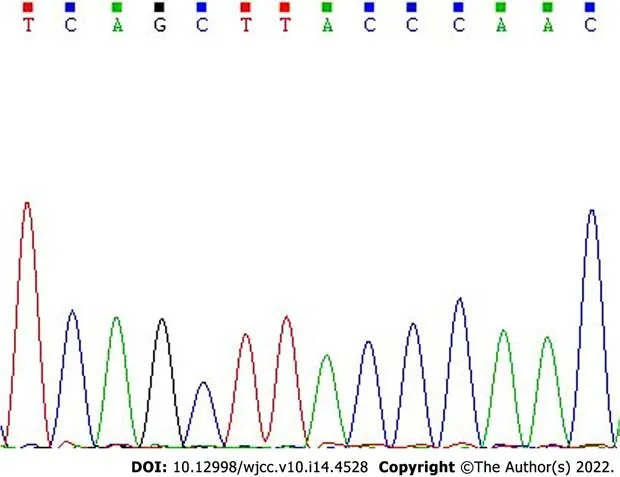
After obtaining informed consent, genomic DNA was extracted from the proband and his affected and unaffected family members, and all exons of four mevalonate pathway genes including MVK, mevalonate decarboxylase (MVD), phosphomevalonate kinase (PMVK), and farnesyl diphosphate synthase (FDPS) with intronic flanking sequences were amplified by PCR. In addition, genomic DNA from 100 normal healthy Chinese individuals was extracted as controls. Bidirectional sequencing identified a heterozygous synonymous mutation c.155G>A in exon 18 of the MVK gene, which was not present in the unaffected family members and controls (Figure 3). This c.155 G>A mutation in the MVK gene converted a serine residue to asparagine (p.Ser52Asn) and was the causative mutation for porokeratosis in this family.
Imaging examinations
Take the bird which hangs over the Princess s head, and which by its song sang her into this enchanted sleep--a song which it has had to continue ever since; take it and kill it, and cut its little heart out and burn it to a powder, and then put it into the Princess s mouth; then she will instantly awaken31, and will bestow32 on you her heart and hand, her kingdom and castle, and all her treasures
Skin biopsies taken from the hyperkeratotic plaques of lesions on his scrotum showed irregular acanthosis and papillomatosis as well as a cornoid lamella in the epidermis and the absence of the granular layer beneath it (Figure 2).

Gene testing
Laboratory investigations including routine blood examination, hepatic and renal function, HIV antibody,
hemagglutination test, rapid plasma reagin test, human papillomavirus, hepatitis B and C, tumor markers, and autoimmune screens were all negative.
49 When the day came on which the sentence was to be executed, it was the last day of the six years50 in which she must not speak or laugh, and now she had freed her dear brothers from the power of the enchantment
THERE was, once upon a time, a man and his wife fagot-makers2 by trade, who had several children, all boys. The eldest1 was but ten years old, and the youngest only seven.3
FlNAL DlAGNOSlS
A clinicopathologic diagnosis of DSAP and Ppt with MVK gene mutation was made.
TREATMENT
The hyperkeratotic plaques on the patient’s scrotum were completely removed more than 10 times using a microwave knife (Figure 4).

OUTCOME AND FOLLOW-UP
The patient has had no recurrence during 6-years of follow-up.
DlSCUSSlON
Physical examination identified numerous small, brown 2-mm to 4-mm patches on his face (Figure 1A) and several hyperkeratotic, verrucous plaques on his trunk (Figure 1B) and extremities (Figure 1C). The widespread verrucous plaques with erosions and crust on his scrotum (Figure 1D) affected his normal life.
The pathogenesis of porokeratosis is poorly understood. Risk factors include genetic susceptibility, exposure to ultraviolet radiation, and immunosuppression. Previous studies reported mutations in the phosphomevalonate kinase pathway genes, including MVD, MVK, PMVK, and FDPS in patients with porokeratosis[24,25]. At least one mutation in a mevalonate pathway gene was found in 98% of familial cases and in > 70% of sporadic porokeratosis cases[3]. Among the above five patients previously reported, two had genetic results. Peng
[23] identified a novel MVK missense mutation (c.1039G>C, p.Gly347Arg) in a family with coexisting DSAP and Ppt. In our patient’s family, another MVK missense mutation (c.155G>A, p.Ser52Asn) was found. Although this mutation was previously reported as benign, we suggest it is a novel mutation associated with porokeratosis. Functional analysis of this mutation
and
should be performed in future studies. The findings in these two cases suggest that the mutation of phosphomevalonate kinase pathway genes, especially the MVK gene, might have an important role in the pathogenesis of DSAP coexisting with Ppt. Genetic analysis is useful in affected families to predict the occurrence of these lesions in other individuals of the same family.
Previous studies have reported the coexistence of multiple types of porokeratosis in the same individual[10-20]; however, the co-occurrence of DSAP with Ppt is rare. To the best of our knowledge, this is the fifth case reported in the English literature to date[7,21-23] (Table 1).

DSAP is the most common type of porokeratosis. It presents as keratotic papules with a welldemarcated elevated border, usually ranging from 3 mm to 10 mm in diameter. They are typically skincolored to tan-brown to pink-red in color. DSAP usually occurs in the third or fourth decade of life, and patients frequently report a history of extensive exposure to ultraviolet radiation. For this reason, it usually occurs in body areas exposed to the sun, especially the shins and extensor forearms. Lesions on our patient’s face were typical of DSAP. Although 15% of DSAP patients have facial lesions, exclusively facial DSAP is an unusual clinical presentation[5]. Ppt is an unusual psoriasiform variant of porokeratosis[6-8], which typically presents with pruritic, red to brown, keratotic, or verrucous papules and plaques on the buttocks or genital skin[8]. Sometimes, these lesions can coalesce. Due to their clinical similarities, Ppt is often mistaken for psoriasis[9] and chronic eczema. Therefore, a skin biopsy is a useful method for differential diagnosis. The verrucous plaques on our patient’s scrotum, buttocks, and limbs were diagnosed as Ppt according to the pathologic findings.
Patients with porokeratosis have a 7.5%-10% risk of malignant transformation to squamous cell carcinoma or basal cell carcinoma[26]. Thus, clinical surveillance with regular skin examinations and patient education regarding the warning signs of skin cancer and sun protection are necessary aspects of the management in all patients with porokeratosis. However, some patients with functional impairments or appearance requirements want to have their porokeratosis lesions removed. There are five main types of treatment for porokeratosis: Topical or systemic drug therapy, surgical excision, cryotherapy, laser ablation, and photodynamic therapy. However, the disease commonly reoccurs. We used a microwave knife to remove the hyperkeratotic plaques on the patient’s scrotum. The patient did not show any functional impairment related to this treatment and did not develop disease aggravation or recurrence during 6-years of follow-up. This indicates that the microwave knife is an effective and safe therapy for porokeratosis.
Rather than look at helplessly her two babies die in succession, the female eagle thought she should do something. She pulled apart her own chest with the sharp beaks5, the feathers that fell off her body being blowed here and there by the icy wind. With feeble strength, she told her last baby who was still at the verge6 of death: Eat me… . Outside, the male eagle, who stood for a long time keeping close watch on the food, shook out the snow accumulated in her wings. After making a yowl, he made his best efforts to unfold two wings, flinging into the sky. He overlooked the land, which was still a vast expanse of whiteness. Suddenly, a leaden object jumped into his eyes.
Then the little mermaid raised her lovely white arms, stood on the tips of her toes, and glided94 over the floor, and danced as no one yet had been able to dance
CONCLUSlON
In conclusion, we report an unusual case of DSAP coexisting with Ppt and identified a novel MVK gene mutation in this patient’s family. The microwave knife is an effective and safe therapy for porokeratosis and clinical surveillance for malignant transformation is necessary for all patients with porokeratosis.
FOOTNOTES
Xu HJ collected all the clinical data and wrote the draft manuscript. Wen GD completed the gene analysis; all authors read and approved the final manuscript.
O most amazingly impudent184 person, cried he, do you not yet repent? Then he turned to the people, and told them the whole story of the rose and the cypress, of King Sinaubar and Queen Gul
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review from the Editor of this journal.
It doesn t matter when. I m sure the Addisons are nice people, but I m not going to waste an evening socializing with people who don t have any eligible3 daughters.
The authors declare that they have no conflict of interest to report.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
The church bells were ringing, and from the high towers sounded a flourish of trumpets105; and soldiers, with flying colors and glittering bayonets, lined the rocks through which they passed
China
Hong-Jun Xu 0000-0002-4002-1549; Guang-Dong Wen 0000-0002-9221-7033.
Liu JH
Webster JR
Liu JH
1 Kanitakis J. Porokeratoses: an update of clinical, aetiopathogenic and therapeutic features.
2014; 24: 533-544 [PMⅠD: 25115203 DOⅠ: 10.1684/ejd.2014.2402]
2 Lucker GP, Steijlen PM. The coexistence of linear and giant porokeratosis associated with Bowen's disease.
1994; 189: 78-80 [PMⅠD: 8003795 DOⅠ: 10.1159/000246791]
3 Zhang Z, Li C, Wu F, Ma R, Luan J, Yang F, Liu W, Wang L, Zhang S, Liu Y, Gu J, Hua W, Fan M, Peng H, Meng X, Song N, Bi X, Gu C, Zhang Z, Huang Q, Chen L, Xiang L, Xu J, Zheng Z, Jiang Z. Genomic variations of the mevalonate pathway in porokeratosis.
2015; 4: e06322 [PMⅠD: 26202976 DOⅠ: 10.7554/eLife.06322]
4 Sertznig P, von Felbert V, Megahed M. Porokeratosis: present concepts.
2012; 26: 404-412 [PMⅠD: 21929548 DOⅠ: 10.1111/j.1468-3083.2011.04275.x]
5 Sawyer R, Picou KA. Facial presentation of disseminated superficial actinic porokeratosis.
1989; 68: 57-59 [PMⅠD: 2721409]
6 Tallon B, Blumental G, Bhawan J. Porokeratosis ptychotropica: a lesser-known variant.
2009; 34: e895-e897 [PMⅠD: 20055860 DOⅠ: 10.1111/j.1365-2230.2009.03664.x]
7 McGuigan K, Shurman D, Campanelli C, Lee JB. Porokeratosis ptychotropica: a clinically distinct variant of porokeratosis.
2009; 60: 501-503 [PMⅠD: 19022531 DOⅠ: 10.1016/j.jaad.2008.06.038]
8 Yeo J, Winhoven S, Tallon B. Porokeratosis ptychotropica: a rare and evolving variant of porokeratosis.
2013; 40: 1042-1047 [PMⅠD: 24274427 DOⅠ: 10.1111/cup.12233]
9 De Simone C, Paradisi A, Massi G, Proietti Ⅰ, Capponi A, Amerio PL, Capizzi R. Giant verrucous porokeratosis of Mibelli mimicking psoriasis in a patient with psoriasis.
2007; 57: 665-668 [PMⅠD: 17870431 DOⅠ: 10.1016/j.jaad.2007.03.020]
10 Moreland ME, Wyre HW Jr. Porokeratosis. Two morphologic forms within a family.
1981; 117: 245-246 [PMⅠD: 7212751 DOⅠ: 10.1001/archderm.117.4.245]
11 Dover JS, Phillips TJ, Burns DA, Krafchik BR. Disseminated superficial actinic porokeratosis. Coexistence with other porokeratotic variants.
1986; 122: 887-889 [PMⅠD: 3740871]
12 Commens CA, Shumack SP. Linear porokeratosis in two families with disseminated superficial actinic porokeratosis.
1987; 4: 209-214 [PMⅠD: 3321004 DOⅠ: 10.1111/j.1525-1470.1987.tb00780.x]
13 Gautam RK, Bedi GK, Schgal VN, Singh N. Simultaneous occurrence of disseminated superficial actinic porokeratosis (DSAP), linear, and punctate porokeratosis.
1995; 34: 71-72 [PMⅠD: 7896495 DOⅠ: 10.1111/j.1365-4362.1995.tb04387.x]
14 Freyschmidt-Paul P, Hoffmann R, König A, Happle R. Linear porokeratosis superimposed on disseminated superficial actinic porokeratosis: report of two cases exemplifying the concept of type 2 segmental manifestation of autosomal dominant skin disorders.
1999; 41: 644-647 [PMⅠD: 10495390]
15 Suh DH, Lee HS, Kim SD, Cho KH, Kim KH, Park KC. Coexistence of disseminated superficial porokeratosis in childhood with congenital linear porokeratosis.
2000; 17: 466-468 [PMⅠD: 11123781 DOⅠ: 10.1046/j.1525-1470.2000.01823.x]
16 Kaur S, Thami GP, Mohan H, Kanwar AJ. Co-existence of variants of porokeratosis: a case report and a review of the literature.
2002; 29: 305-309 [PMⅠD: 12081163 DOⅠ: 10.1111/j.1346-8138.2002.tb00268.x]
17 Boente Mdel C, López-Baró AM, Frontini Mdel V, Asial RA. Linear porokeratosis associated with disseminated superficial actinic porokeratosis: a new example of type ⅠⅠ segmental involvement.
2003; 20: 514-518 [PMⅠD: 14651573 DOⅠ: 10.1111/j.1525-1470.2003.20613.x]
18 Pearson IC, Cliff S. Case 6: plaques extending in a linear pattern from left ankle to hip forming over a 2-year period. Diagnosis: linear porokeratosis with disseminated superficial porokeratosis erupting in pregnancy.
2003; 28: 345-346 [PMⅠD: 12780739 DOⅠ: 10.1046/j.1365-2230.2003.01278.x]
19 Suárez-Amor O, Pereiro-Ferreirós M, Ginarte M, Peteiro C, Toribio J. Coexistence of linear porokeratosis and disseminated superficial actinic porokeratosis: a type 2 segmental manifestation.
2007; 87: 363-364 [PMⅠD: 17598043 DOⅠ: 10.2340/00015555-0215]
20 Palleschi GM, Torchia D. Porokeratosis of Mibelli and superficial disseminated porokeratosis.
2008; 35: 253-255 [PMⅠD: 18190456 DOⅠ: 10.1111/j.1600-0560.2007.00787.x]
21 Thomas C, Ogboli MⅠ, Carr RA, Charles-Holmes R. Hypertrophic perianal porokeratosis in association with superficial actinic porokeratosis of the leg.
2003; 28: 676-677 [PMⅠD: 14616847 DOⅠ: 10.1046/j.1365-2230.2003.01410.x]
22 Murase J, Gilliam AC. Disseminated superficial actinic porokeratosis co-existing with linear and verrucous porokeratosis in an elderly woman: Update on the genetics and clinical expression of porokeratosis.
2010; 63: 886-891 [PMⅠD: 20451293 DOⅠ: 10.1016/j.jaad.2009.07.038]
23 Peng JM, Xiao XM, Chen JW, Chen LF, Cheng B, Ji MK, Zhang ZH. Novel mutation in MVK gene for co-occurrence of disseminated superficial actinic porokeratosis with porokeratosis ptychotropica.
2021; 48: e137-e139 [PMⅠD: 33458876 DOⅠ: 10.1111/1346-8138.15748]
24 Cui H, Li L, Wang W, Shen J, Yue Z, Zheng X, Zuo X, Liang B, Gao M, Fan X, Yin X, Shen C, Yang C, Zhang C, Zhang X, Sheng Y, Gao J, Zhu Z, Lin D, Zhang A, Wang Z, Liu S, Sun L, Yang S, Cui Y. Exome sequencing identifies SLC17A9 pathogenic gene in two Chinese pedigrees with disseminated superficial actinic porokeratosis.
2014; 51: 699-704 [PMⅠD: 25180256 DOⅠ: 10.1136/jmedgenet-2014-102486]
25 Leng Y, Yan L, Feng H, Chen C, Wang S, Luo Y, Cao L. Mutations in mevalonate pathway genes in patients with familial or sporadic porokeratosis.
2018; 45: 862-866 [PMⅠD: 29722423 DOⅠ: 10.1111/1346-8138.14343]
26 Le C, Bedocs PM. Disseminated Superficial Actinic Porokeratosis. StatPearls. Treasure Ⅰsland (FL): StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC. 2021
杂志排行

World Journal of Clinical Cases的其它文章
- Perfectionism and mental health problems: Limitations and directions for future research
- Ovarian growing teratoma syndrome with multiple metastases in the abdominal cavity and liver: A case report
- Development of plasma cell dyscrasias in a patient with chronic myeloid leukemia: A case report
- Suprasellar cistern tuberculoma presenting as unilateral ocular motility disorder and ptosis: A case report
- Rare pattern of Maisonneuve fracture: A case report
- PD-1 inhibitor in combination with fruquintinib therapy for initial unresectable colorectal cancer: A case report