Paradoxical carbon dioxide embolism during laparoscopic hepatectomy without intracardiac shunt:A case report
2022-06-22SoeunJeonJeongMinHongHyeonJeongLeeYesulKimHyunjongKangBooyoungHwangDowonLeeYounghoonJung
lNTRODUCTlON
Laparoscopic surgery is an alternative to conventional laparotomy and is widely used because of its advantages including less postoperative pain,earlier recovery after surgery,and reduced postoperative complications such as infection or incisional hernia[1].In particular,laparoscopic hepatectomy has recently become popular because it leads to less bleeding than open hepatectomy.However,laparoscopic hepatectomy requires low central venous pressure,high pneumoperitoneum pressure,and Pringle maneuvers,all of which increase the likelihood of COembolism[2].Therefore,COembolism occurs more frequently in laparoscopic hepatectomy than in general laparoscopic surgery.Most COembolisms during laparoscopic surgery are microembolisms and may be self-resolving without any symptoms or clinical signs due to the high solubility of COin blood.However,severe COembolism may cause hypotension,cyanosis,arrhythmia,cardiovascular collapse,neurologic deficits,or even arrest[3].In particular,paradoxical COembolisms are highly likely to cause neurological deficits[4].
We describe a case of paradoxical COembolism found using transesophageal echocardiography(TEE)during laparoscopic hepatectomy even though the patient did not have an intracardiac shunt.
CASE PRESENTATlON
Chief complaints
A 71-year-old man(height,169.4 cm;weight,80.5 kg)presented with sudden hypoxia,hypotension,and decreased end-tidal carbon dioxide(EtCO)during laparoscopic left hemi-hepatectomy.
History of present illness
The patient was diagnosed with hepatocellular carcinoma and was admitted to our hospital for laparoscopic left hemi-hepatectomy.Preoperative ECG,chest radiography,and laboratory findings were within the normal range except renal function test results[blood urea nitrogen(BUN): 20.4 mg/dL,creatinine: 1.44 mg/dL,and glomerular filtration rate:(GFR)48.2 mL/min/1.73 m].Preoperative transthoracic echocardiography(TTE)revealed degenerative moderate/severe aortic stenosis[aortic valve peak velocity: 3.2 m/s,peak pressure gradient(PG),41 mmHg;mean PG,20 mmHg].For further evaluation,TEE was performed,and the aortic valve area on three dimensional multiplanar reconstruction planimetry was 1.13 cm.The biventricular and other valves were normal or had mild degenerative changes.
Glycopyrrolate 0.2 mg was administered as premedication.In the operating room,standard monitoring[ECG,pulse oximetry(SpO),noninvasive blood pressure,end-tidal CO(EtCO),and esophageal stethoscope temperature],bispectral index(BIS),train of four,pleth variability index(PVI),and urine output monitoring were performed,and the patient’s initial(pre-induction)heart rate(HR),SpO,systolic blood pressure(SBP),diastolic blood pressure(DBP),EtCO,and respiratory rate(RR)were 68 beats/min,99%,186 mmHg,89 mmHg,36 mmHg,and 16 breaths/min,respectively.The vital signs,administered drugs,and arterial blood gas analysis(ABGA)values during surgery are shown in Figure 1.The operation was performed under general anesthesia.Before induction,arterial catheterization of the left radial artery was performed under local anesthesia for real-time blood pressure monitoring.Anesthesia was induced using propofol(70 mg),remifentanil[4.0 ng/mL;effect-site concentration(Ce),target-controlled infusion(TCI)based on the Minto Model],and atracurium(25 mg).After anesthesia induction,a central line was cautiously placedthe right internal jugular vein.To prevent hypotension,phenylephrine infusion was administered at 0.5 µg/kg/min.Anesthesia was maintained with 4-6 vol% desflurane,and continuous infusion of remifentanil(0.1-4.0 ng/mL).Atracurium(4 µg/kg/min)was infused to induce muscle relaxation during surgery.Volume-controlled ventilation with the following parameters was adopted: tidal volume,425 mL;respiratory rate,12-14 breaths/min,inspiratory-to-expiratory time(I:E)ratio 1:2;and FiO0.5,without positive end-expiratory pressure(PEEP).Intraoperative fluid was restricted to lower central venous pressure(CVP)during surgery,and intermittent boluses of fluid were administered to maintain urine output(0.5 mL/kg/h).When the patient was draped,hydrocortisone(100 mg)was administeredslow intravenous injection.After three trocars were inserted,the patient was placed in the reverse Trendelenburg position with a left tilt,and COwas insufflated to a pressure of 17 mmHg.During the surgical procedure,hypotension(SBP/DBP,90/45 mmHg)was observed despite continuous phenylephrine infusion;therefore,norepinephrine infusion was administered at 0.1-0.2 µg/kg/min and phenylephrine was tapered.After administration of norepinephrine,the patient’s vital signs remained stable.During ligation of the left hepatic vein,the inferior vena cava(IVC)was accidentally torn.The patient’s SpOsuddenly dropped from 97% to 85%.His blood pressure decreased to 89/40 mmHg(SBP/DBP).The EtCOdropped from 30 to 24 mmHg.A “mill-wheel” murmur was auscultated over the precordium.
History of past illness
He had a history of hypertension,diabetes,and stage 3a chronic kidney disease.He was taking aspirin,lercanidipine,gemigliptin,insulin glargine,kalimate(polystyrene sulfonate calcium),and renamezin(spherical adsorptive carbon).
Jeon S and Hong JM designed the study;Jeon S,Hong JM,and Lee HJ drafted the manuscript;Kim Y,Kang H,and Jung Y collected data and pictures;Jeon S,Hong JM,Lee HJ,Hwang B,and Lee D reviewed the literature and edited the manuscript;all authors agreed to be accountable for all aspects of the work,and all authors issued final approval for the version to be submitted.
Personal and family history
There was no remarkable personal and family history.
Physical examination
The “mill-wheel” murmur was auscultated over precordium at the same time as sudden hypoxia,hypotension,and decrease in EtCO(from 30 mmHg to 24 mmHg,Figure 1).
Well pleased with what he had done, he went to bed again to his wife. So soon as Little Thumb heard the Ogre snore, he waked his brothers, and bade them all put on their clothes presently and follow him. They stole down softly into the garden, and got over the wall. They kept running about all night, and trembled all the while, without knowing which way they went.
Although our patient fortunately did not exhibit any neurological deficit after surgery,previous reports have indicated that paradoxical gas embolism may cause neurological deficits such as cerebral infarction[4].Considering this point,it is important to quickly identify paradoxical COembolisms and to pay attention to complications such as neurological deficits after surgery.
Laboratory examinations
When paradoxical COembolism occurred,ABGA was performed and revealed a pH of 7.112,PCOof 78.8mmHg,and POof 73.3 mmHg.
The paralysed girl sits in the warm sunshine and can see thewood and the lake; the world had become so large, so beautiful, andonly through a single word from the kind mistress of the mansion
Imaging examinations
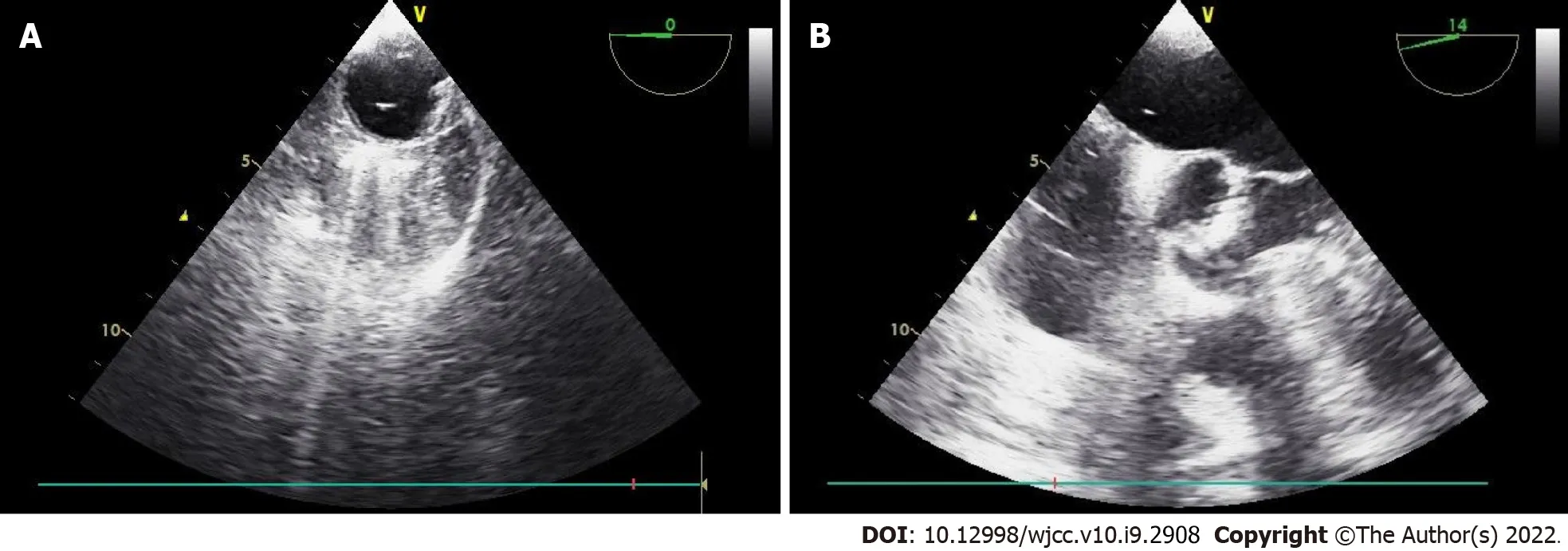
Given the clinical signs,we suspected that COgas had entered the injured vessel.However,since the patient also had moderate aortic valve stenosis,TEE was immediately performed for accurate differentiation and diagnosis.TEE revealed that gas bubbles were scattered in the right side of the heart,and a few were detected in the left atrium,left ventricle,and ascending aorta(Figure 2).Intracardiac shunts,such as a patent foramen ovale(PFO)or ventricular septal defect(VSD),were not observed.

FlNAL DlAGNOSlS
The patient was diagnosed with paradoxical COembolism developed during laparoscopic hepatectomy.
TREATMENT
Fluid resuscitation for blood loss due to the torn IVC was initiated.To correct the sudden onset hypoxia,the infused oxygen concentration was increased immediately from 50% to 100% with 5 cmHO of PEEP,and hyperventilation was maintained to wash out CO.To correct the hypotension,the infusion of norepinephrine was increased to maintain systolic blood pressure above 90 mmHg.Immediately after confirming paradoxical COembolism using TEE,we informed the surgeon of the situation,and the surgeon then reduced the insufflation pressure from 17 mmHg to 14 mmHg.After the torn IVC was repaired laparoscopically and the bleeding was controlled,the size of the gas bubble on TEE reduced,and the patient’s hemodynamic state stabilized.No more air was observed on the TEE performed 30 min later(Figure 3).The norepinephrine infusion was gradually tapered.The SpOincreased to 99%,and FiOreduced to 0.5.At the end of the operation,the ABGA revealed a pH of 7.282,PCOof 50.5 mmHg,and POof 111.1 mmHg.The total anesthesia time and operation time were 290 min and 265 min,respectively.The estimated blood loss was 1000 mL,and the total intraoperative urine output was 560 mL.Crystalloid(1700 mL),5% albumin(250 mL),and packed red blood cells(1 unit)were administered during the operation.

OUTCOME AND FOLLOW-UP
The patient was transferred to the surgical intensive care unit for close monitoring and ventilator care under sedation.Bedside TTE confirmed that definite CObubbles had disappeared.Brain computed tomography was performed on postoperative day(POD)1 to exclude embolic stroke,and it revealed no abnormalities.Ventilator weaning and extubation were performed on POD2 and the patient was transferred from the intensive care unit to the general ward on POD3 without any cardiovascular or neurologic complications.The postoperative laboratory examination results on POD3 were within normal range,except for ALT,59 U/L;BUN/Cr,46.2/1.31 mg/dL;GFR,53.8 mL/min/1.73 m;PT,14.1 s;and INR,1.25.This study was approved by the Institutional Review Board of Pusan National University Hospital,Republic of Korea(ID: 2105-009-102).
DlSCUSSlON
Gas embolism during laparoscopic surgery is reported as a rare complication,with an overall incidence of 0.014%-0.6%[3,5].However,in cases of clinically significant COembolism,mortality is reported to be 28%[6].COembolism is mainly caused by incorrect insertion of a Veress needle,and surgical sites with many venous channels or the generation of pressure gradients for gas entry into circulation also increase the risk of COembolism during laparoscopic surgery[7].Particularly,the risk may increase in patients with primary biliary cirrhosis by upregulated angiogenesis or with unanticipated anatomical variations such as patent paraumbilical veins[8,9].The incidence of gas embolism is further increased in laparoscopic hepatectomy(1.2%-4.6%)[10].Laparoscopic hepatectomy,which has recently become a popular surgical method,is performed as it is associated with less bleeding,less postoperative pain,and faster recovery.Low CVP,high-pressure pneumoperitoneum,and the Pringle maneuver are required for successful laparoscopic hepatectomy.However,these methods are believed to be associated with an increased risk of COembolism.High-pressure pneumoperitoneum with low CVP creates a pressure gradient,which increases the likelihood of COembolism.The Pringle maneuver is a method of controlling bleeding by inhibiting blood flow through the portal vein and hepatic artery.When this maneuver is implemented,the intrahepatic pressure becomes equal to the CVP,which may contribute to the increased risk of COembolism[2,10].
When the mother and daughter heard who Jurgen was, and howinnocently he had suffered, they looked at him in a still morefriendly way; and pretty Clara s eyes had a look of especialinterest as she listened to his story. Jurgen found a happy home inOld Skjagen. It did his heart good, for it had been sorely tried. Hehad drunk the bitter goblet of love which softens or hardens theheart, according to circumstances. Jurgen s heart was still soft- itwas young, and therefore it was a good thing that Miss Clara was going in three weeks time to Christiansand in Norway, in her father s ship, to visit an aunt and to stay there the whole winter.On the Sunday before she went away they all went to church, to the
Clinical Research Grant from Pusan National University Hospital in 2020.
Clinical manifestations of COembolism include hypotension,tachycardia,arrhythmia,dyspnea,cyanosis,and cardiovascular collapse[3].COembolism can be caused by unintended placement of a Veress needle or trocar into a blood vessel.Additionally,COentering injured blood vessels or surgical sites during surgery may lead to embolism.The CObubbles can move to the vena cava and right ventricle(RV),which may limit venous return and cause RV outflow obstruction[14].The “mill-wheel” murmur,which is described as loud,harsh,splashing,or machine-like sound,can be auscultated when a large amount of gas is entrapped.Moreover,a sudden decrease in EtCOis also a clinical sign of gas embolism,which is caused by an obstruction of the pulmonary circulation[15].In this case,hypoxia,hypotension,decreased EtCO,and mill-wheel murmur occurred after IVC injury;therefore,we suspected COembolism and confirmed it using TEE.Furthermore,we confirmed that paradoxical COembolism had occurred when TEE was used.
The authors declare that they have no conflicts of interest.
The same thing happened on the third day when the prince tried to get past: the lindorm said, with a threatening voice, that before the prince could get a bride he himself must find a mate
The wind was blowing fiercely across the land, and the clouds flying across the sky looked as gloomy as if it were night; the leaves were being blown from the trees; the water was foaming26 and seething27 and dashing upon the shore, and in the distance he saw the ships in great distress28, dancing and tossing on the waves
We confirmed paradoxical COembolism using immediate TEE.TEE,the most sensitive diagnostic tool,can detect a much smaller amount of gas,as little as 0.2 mL/kg,than can be detected using EtCO[15,16].COembolism is usually diagnosed with clinical symptoms alone when TEE cannot be used.Therefore,most reported cases of COembolism are accompanied by serious symptoms,such as hemodynamic deterioration.However,although not reported,it is assumed that many cases of COembolism occurred without symptoms and then disappeared without being recognized by anesthesiologists and surgeons.Derouin reported that the incidence of COembolism was 69% during laparoscopic cholecystectomy when TEE was pre-inserted[21].Furthermore,Kim reported that venous air embolism was observed in all patients during laparoscopic hysterectomy,and 37.5% of these emboli were present in significant amounts[22].However,neither study showed any hemodynamic instability.Therefore,it is not sufficient to diagnose COembolism based on symptoms alone.Moreover,it is difficult to identify paradoxical COembolism,as in this case,only based on clinical symptoms without the use of TEE.In particular,cases in which the absence of an intracardiac shunt is confirmed by preoperative examination are more likely to be excluded.TEE can also diagnose COembolism quickly and accurately,so it can differentiate it from other causes of hemodynamic deterioration.The patient in this case had moderate-to-severe aortic stenosis.Because symptoms such as hypotension,hypoxia,and decreased EtCOmay also occur due to aortic stenosis,it is difficult to make an accurate diagnosis based on clinical symptoms alone.Therefore,if COembolism is suspected or if it is necessary to differentiate it from other causes,we recommend quick identification using TEE.Kim[22]described that although most venous air embolism is asymptomatic,caution is needed because fatal air embolism can occur in patients with cardiopulmonary disease or intracardiac shunt.Therefore,pre-insertion of TEE may be helpful for these patients.
When COembolism is suspected,the anesthesiologist should promptly inform the surgeon,and the COinsufflation should be stopped to prevent additional gas entrainment.Hyperventilation with 100% oxygen was used to eliminate CO.Further,PEEP can be applied to prevent additional gas entrapment.A Trendelenburg or left lateral decubitus position is helpful in preventing the progression of COembolism[3].COaspiration through the central venous catheter may also be considered.In this case,the surgeon did not switch to open surgery and only reduced the peritoneum pressure and sutured the damaged vessel.This is because it was judged that if the pneumoperitoneum was stopped and there was a conversion to open surgery,the bleeding could become more severe and the vital signs would worsen during the conversion.Although the Trendelenburg position is helpful,the position was not changed to ensure optimal viewing of the surgical field during laparoscopic repair in this case.Therefore,communication with the surgeon is essential for such a complex surgery,and a dedicated and well-trained team is important.
Six years after high school graduation, Marc called and asked if he could move home for a couple of months. He had spent those years well, graduating Phi Beta Kappa magna cum laude from college, completing two congressional internships in Washington, D.C., winning the Jesse Marvin Unruh Fellowship4 to the California State Legislature, and finally, becoming a legislative5 assistant in Sacramento. Other than short vacation visits, however, he had lived away from home. With his younger sister leaving for college, I was especially thrilled to have Marc coming home.
Herein,we report a case of paradoxical COembolism during laparoscopic hepatectomy.Anesthesiologists should be aware that COembolism can occur during laparoscopic surgery,particularly during laparoscopic hepatectomy.Additionally,paradoxical embolism should be considered even in the absence of an intracardiac shunt.Therefore,TEE is important to quickly confirm the presence and extent of COembolism and to prevent complications.
CONCLUSlON
Laparoscopic surgery,especially laparoscopic hepatectomy,inevitably carries the risk of COembolism,including paradoxical COembolism.Paradoxical COembolism can occur even without an intracardiac shunt,and it is difficult to diagnose based on symptoms alone.Intraoperative TEE can help quickly identify the presence and extent of COembolism,which will help with appropriate treatment and prediction of postoperative complications.
FOOTNOTES
I should like to see Rome, she said; it must be a lovelycity, or so many foreigners would not be constantly arriving there.Now, do give me a description of Rome. How does the city look when you enter in at the gate?
All these methods were used in this case.In particular,a higher pneumoperitoneum pressure(17 mmHg)was used.Typically,pressures of 12 mmHg or less are used to reduce the risk of gas embolism,and a pressure of 12-15 mmHg is used for bleeding control in some institutions[10].Chiu[11]reported that the incidence of COembolism was higher in a high insufflation pressure group than in a low pressure group.According to animal studies,intraoperative bleeding is lower when a high pneumoperitoneum pressure is used;however the risk of COembolism increases[12,13].Although the biggest cause of embolism in this case was the rapid inflow of COgas into the injured vessel,it is presumed that all these factors may have increased the effect.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Paradoxical air embolism is generally known to occur in the presence of an intracardiac shunt,such as patent foramen ovale(PFO),ventricular septal defect(VSD),and patent ductus arteriosus[16].However,in this case,no intracardiac shunt was found on preoperative or intraoperative echocardiographic examinations.Similar to our case,several reports have described paradoxical air embolism that occurred during laparoscopic surgery even though the patients did not have an intracardiac shunt[4,17-19].In these reports,the authors described three possible mechanisms.First,it may be caused by temporarily opened PFO;second,it may be caused by pulmonary vascular dilation and arteriovenous communication in patients with liver cirrhosis;and third,COembolism may be caused by the overflow of venous gas bubbles into the arterial circulation through the lung[4].In our patient,no VSD or PFO was observed during the preoperative and intraoperative TEE.Furthermore,the patient did not have liver cirrhosis.The existence of communication of pulmonary arterioles and venous cannot be completely excluded in this patient.For confirmation,the agitated saline test may be helpful.If the left side gas bubble appears after 3 to 8 heartbeats,the existence of the abnormal communication of pulmonary arterioles and venous may be suspected[20].However,considering the improvement of symptoms after repairing damaged blood vessels,we presumed that the overflow of a large amount of venous gas bubbles entering the damaged blood vessel was the main mechanism.
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
South Korea
Soeun Jeon 0000-0002-4009-6321;Jeong-Min Hong 0000-0003-3527-555X;Hyeon Jeong Lee 0000-0002-3450-865X;Yesul Kim 0000-0002-3069-3261;Hyunjong Kang 0000-0002-6108-8873;Boo-young Hwang 0000-0001-6098-0627;Dowon Lee 0000-0001-5140-2358;Young-hoon Jung 0000-0001-6802-2028.
When she saw this image she was frightened, and let her cup fall into the stream, and thought, Is it an angel, or a peri, or a man? Fear and trembling took hold of her, and she screamed as women scream
Liu JH
Grandpa filled his hours with television. He watched the news and game shows while Grandma went about her day. They made a pact—he was not to leave his chair or his bed without her assistance.
A
Liu JH
杂志排行

World Journal of Clinical Cases的其它文章
- Role of metabolites derived from gut microbiota in inflammatory bowel disease
- Roles of Wnt/β-catenin signaling pathway related microRNAs in esophageal cancer
- Associations between coagulation factor Xll,coagulation factor Xl,and stability of venous thromboembolism:A case-control study
- Nomogram to predict the risk of endoscopic removal failure with forceps/baskets for treating submandibular stones
- Animal models applied to acute-on-chronic liver failure:Are new models required to understand the human condition?
- Association between anesthesia technique and complications after hip surgery in the elderly population