Efficacy of bone grafts in jaw cystic lesions:A systematic review
2022-06-22JinWangQiuYunYaoHuiYongZhu
lNTRODUCTlON
Jaw cysts are a common benign disease of the maxillofacial region,and odontogenic cysts represent the majority of cases[1].The most common types of cystic lesions include radicular cysts,dentigerous cysts(follicular cysts),and keratocystic odontogenic tumors(keratocysts),collectively accounting for more than 80% of odontogenic cysts[2].These cysts usually appear as defects in the epithelial lining in the mandible or maxilla and gradually increase in volume but do not invade surrounding bone or damage nerves[3].However,bone defects can lead to pathological bone fracture,loss of teeth,infection,and other symptoms[4].
There are three main treatments for bone cysts: cystectomy,decompression followed by cystectomy,and cystectomy followed by bone grafting[5].The most common treatment is cystectomy.During surgery,the whole cyst is removed,and the surface of the bone containing the cyst is scraped if required.Peripheral ostectomy is required to remove any daughter cysts in keratocystic odontogenic tumors.Spontaneous bone healing also repairs bone defects[6].For larger defects,some studies have shown that decompression before enucleation has a good effect[7].
Decompression and cystectomy are not always sufficient to achieve complete bone regeneration,and the healing process can be lengthy.Therefore,the cavities are often filled with bone grafts or other bone regeneration materials to improve outcomes in the treatment of jaw cysts.Some researchers suggest that when the size of the defect reaches 1-2 cm or 50% of the circumference of the bone,filling materials are needed[8].Nevertheless,there are quite a few reports of complete spontaneous bone healing of large jaw cysts[9].Defects as large as 10 cm can achieve complete spontaneous bone healing when given one year according to reports[6].The indications for bone grafts in jaw cystic lesions and the need for bone grafting after enucleation remain controversial[10,11].
The wolf also figures prominently in other parts of British folklore18, such as the traditional children s game, What s the Time, Mr. Wolf? Return to place in story.
Therefore,in this review,we performed a systematic search and analysis focusing on the efficacy of bone grafts compared to spontaneous healing in the treatment of jaw cystic lesions,providing guidance for further research and clinical work.Randomized clinical trials,controlled clinical trials,and beforeand-after studies were included.
MATERlALS AND METHODS
Study design
This systematic review focuses on the bone regeneration rate after bone grafting compared to spontaneous healing in the treatment of jaw cystic lesions.
Literature search
Relevant studies were sought using Medline,Cochrane Library,and Embase.The period was restricted to the last ten years.The following key words and MeSH terms were used for the searches: jaw cyst,cystic lesion,odontogenic cyst,periapical cyst,dentigerous cyst,follicular cyst,keratocyst,treatment,surgery,bone graft,enucleation,cystectomy,and bone regeneration.The article type was restricted to case reports,clinical trials,clinical studies,observational studies and randomized controlled trials.Searches were performed according to PRISMA systematic review guidelines[12].Literature searches and study screenings were performed by two researchers independently.
Eligibility criteria
Bone grafting failure can occur when preoperative infection exists,the third mandibular molar is located in the cyst cavity,non-autogenous and autogenous bone grafts are used in combination,or the patient has perilesional osteosclerosis[46].Notably,researchers have opposite opinions on the incidence of postoperative infection after bone grafting[47,48].
Studies were excluded according to the following criteria:(1)No assessment of bone regeneration;and(2)No uniform follow-up time.
15. Robbers: Robbers . . . may symbolize37 the rebellion of the young against authority and parental38 (especially paternal) power . . . (Biederman 286).
Study selection
Two articles grouped cases according to clinical characteristics and analyzed factors that affect bone healing.The location of the defect in the mandible represents another important factor,and better bone regeneration was noted in the mandible compared with the maxilla[16].On the other hand,follow-up time and initial size were evidently relevant factors,whereas histological lesion type and patient age were recognized as nonrelevant factors[17].However,the sample size was small in both articles.
Yes, ma am. It s too much to expect an ordinary mother to give up all six sculptures she made from a 60 foot tall crane that a total stranger left in her back yard.
The Prince had no wish to take such an insignificant17 bundle with him; but he didn t like to hurt Puddocky s feelings by refusing it, so he took up the little packet, put it in his pocket, and bade the little toad farewell
Quality assessment
The quality of uncontrolled studies was evaluated using the ROBINS-I(“Risk Of Bias In Nonrandomized Studies - of Interventions”)tool[13],whereas randomized comparative studies were evaluated with RoB 2[14].
Data extraction and analysis
The following information from the included articles was summarized and analyzed: study type,treatment,number of patients,cyst type,diameter(largest),follow-up time,assessment methods,bone regeneration rate,and factors related to effectiveness.Risk of bias across studies was assessed according to the above information.The data were analyzed based on previous research.The defect was assumed to be spherical if calculation of values was needed.The bone regeneration rate data were grouped and compared between the cystectomy-alone group and the bone grafting group.
RESULTS
Study characteristics
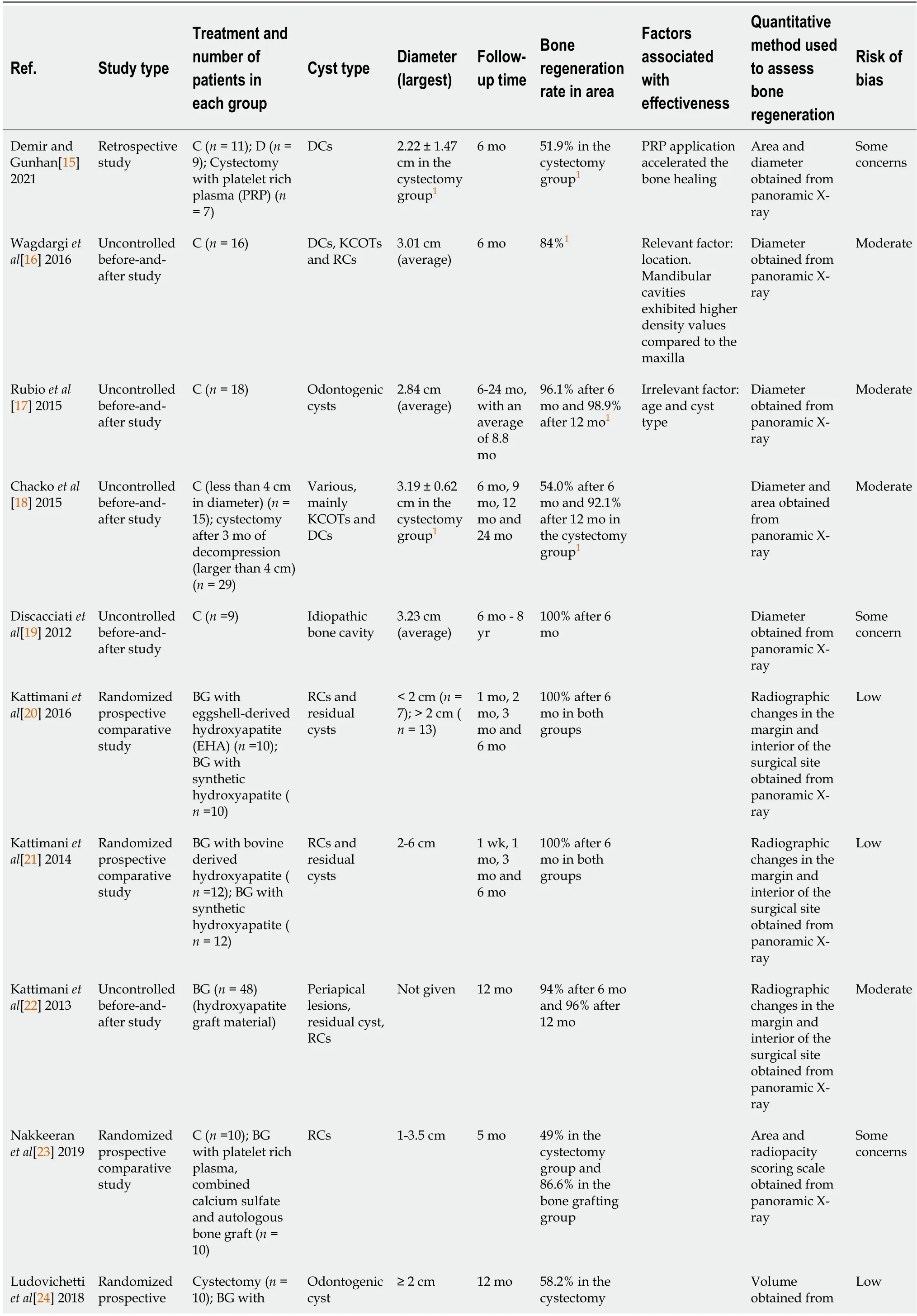
As shown in the flow diagram in Figure 1,10 of the 117 articles met the inclusion criteria.These studies included many types of jaw cysts,such as radicular cysts,keratocysts,and dentigerous cysts.Five studies reported spontaneous bone healing after enucleation[15-19],three studies investigated the efficacy of various bone grafts[20-22],and two randomized comparative studies focused on the comparison between spontaneous healing and bone grafting[23,24].The article type,treatment,bone regeneration rate,quantitative assessment method of bone regeneration and overall quality of each study are summarized in Table 1.
As her father wished to give her to another, the prince was rejected; but as they both loved each other with all their hearts, they would not give each other up, and Maid Maleen said to her father, I can and will take no other for my husband


Bias across studies and data processing
In the included studies,researchers chose before-and-after size and volume as the main indicators,but the studies adopted different methods to assess bone regeneration.Panoramic X-rays were applied in nine studies,of which six reported the change in the diameter or area of defects.The other three studies used the radiographic changes in the margin and interior of the surgical site to indicate the level of bone regeneration after grafting.In the last study,researchers calculated the volume of defects through cone beam computed tomography(CBCT)scans and reported the volume reduction rate[24].In addition to size,Nakkeeran[23]also used a radiopacity scoring scale to further assess bone healing.
Heterogeneity was also noted regarding the size of the initial defect and the follow-up time.Averages were given in five studies,but the other four studies only provided a range and one study gave no information about the initial defect size.Therefore,statistical analysis of the efficacy of bone regeneration rate of bone grafting and cystectomy was not available.For a more direct comparison,we performed calculations and chose the bone regeneration rate in the area as the indicator for comparison.Errors occurred during calculations since the actual defect was usually irregular.
Main findings
In the included articles,over 80% of bone healing occurred within 12 mo after bone grafting,regardless of the type of grafting material.In the three studies which evaluated the efficacy of bone grafting,over 90% of bone regeneration occurred in 6 mo[20-22].Meanwhile,in the two randomized comparative trials,bone grafting after cystectomy showed significant superiority over cystectomy alone,with bone regeneration rates of greater than 80% and 90% after 5 mo and 12 mo,respectively[23,24].
However,the bone regeneration rate after cystectomy showed great variation,ranging from 50% to 100% after 6 mo.In three studies,the bone regeneration rate reached over 90% after 12 mo[17-19].The averages of initial defect diameter were all larger than 2 cm when only cystectomy was conducted.In the study which reported complete healing after 6 mo,the patients were all under 18 years old and diagnosed with idiopathic bone cavities[19].In the other six studies,including the two comparative trials,the age of patients ranged from adolescence to middle age.
Due to the high heterogeneity across studies,we could not confirm the efficacy of bone grafting compared with spontaneous healing.Bone grafting may have some advantage in early bone regeneration within 6 mo,but spontaneous healing could achieve satisfactory results in 1-2 years.In addition,since it was difficult for us to compare the initial size of defects due to the high heterogeneity,we could not analyze the relationship between bone regeneration rate and initial size.
The articles obtained from the search were imported into Endnote X9 for further selection.During the first stage,articles were screened by title and abstract.Then,full texts were evaluated to identify articles that met the criteria.Study selection was performed by two reviewers independently.
DlSCUSSlON
Apart from defect size,controversies have been noted regarding the histological type of lesions,and their age and location[16,41].One study included in this review reported better bone regeneration in the mandible compared with the maxilla[16].This conclusion also concurred with previous studies on decompression[42,43].
The efficacy of bone grafting compared to spontaneous healing in jaw cystic lesions
Bone regeneration occurs spontaneously in a suitable environment that includes good blood supply and mesenchymal cells.However,due to the lack of mechanical support,defects of a critical size cannot heal completely[8,25].Under these conditions,external materials are needed to help bone regeneration[26].
As soon as Beauty was alone she hastened to fill the boxes with all the rare and precious things she saw about her, and only when she was tired of heaping things into them did they seem to be full
said the Great, Huge Bear, in his great, rough, gruff voice. And when the Middle Bear looked at his, he saw that the spoon was standing in it, too. They were wooden spoons; if they had been silver ones, Goldilocks would have put them in her pocket.18
Many types of bone grafts,including autografts such as iliac bone,xenografts,and other materials facilitating bone regeneration,have been used with good results[27].Bovine-derived hydroxyapatite and synthetic hydroxyapatite help achieve maximum bone healing within 6 mo[21].Other materials,such as plasma-rich gels,have also been proven to be effective[28].
“Now, how would you like a chance to earn a few easy straws like the rest of us? I still have the name I picked tonight in my pocket, and I haven’t looked at it yet. Why don’t we switch, just for the last day? It will be our secret.”
Based on previous literature and analysis described above,we noted that the superiority of bone grafting is unclear.High heterogeneity and lack of relevant studies made meta-analysis difficult.This finding corresponds with the conclusion in two previous systematic reviews.Ettl[10]summarized the application of different bone grafts in jaw cysts and concluded that the use of bone grafts remains “state of the art”.Buchbender[29]conducted a literature search up to 2016,but they also failed to propose treatment recommendations.In a retrospective 3D analysis of bone regeneration after cystectomy with or without iliac bone grafting,which was excluded from our research because of nonuniform follow-up time,filling therapy did not affect bone regeneration significantly.
On the other hand,the role of grafts in promoting bone formation was verified.In randomized trials in which variables were controlled,bone grafting showed a definite advantage over cystectomy within one year[23,24].Other investigations on bone grafting showed complete bone healing three months after grafting,indicating the role of grafting in early bone formation[20,22].
The efficacy of bone grafts is difficult to define due to a shortage of literature.There are several clinical trials studying the usefulness of bone grafts in jaw lesions,but the results have not yet been published[30,31].In addition,research involving defects smaller than 2 cm or follow-up times greater than 12 mo is lacking.
Factors associated with effective bone formation and treatment considerations for jaw cystic lesions
Reconstructive therapy is recommended for critical-size defects that are likely to persist,recur,or cause infection or bone fracture[8,32].However,due to the complex morphology of the jaw,the different types of cysts and the influence of teeth or inflammation,the indications for bone grafts are difficult to specify in maxillofacial bone[33,34].In addition,these confounding factors are difficult to control in research,accounting for the high heterogeneity across the articles we included.
According to our research and previous systematic reviews focusing on the effect of bone grafting after enucleation,the superiority of bone grafts is still not evident[10,11].On the other hand,the role of bone grafting in accelerating bone regeneration is absolute,making it suitable for rapid recovery of bone quality.Therefore,we proposed to analyze each case independently according to the basic biological factors for bone regeneration.The following are some considerations when treating jaw cystic lesions.
Some researchers have proposed that preservation of the periosteum and bone wall,adequate blood supply,and a solid basis for bone regeneration are the most significant criteria for bone healing[35,36].The preservation of periosteum during cystectomy is essential for bone regeneration[37].With the existence of bone plates,spontaneous healing occurred regardless of cyst type,initial size,or age[17].In general,after enucleation,jaw cystic lesions are characterized as intrabony cavities.The surrounding bone walls usually maintain the contour of bone and provide solid support for blood clots,which can create a suitable physical environment for bone regeneration.Therefore,bone grafts can maximize the effect when the contour of bone needs to be reconstructed;for example,when the height or width of bone is lost[38].Similarly,bone grafts can be applied when the periosteum is lost,which can occur during surgery and cause a lack of osteogenesis-related cells and molecules.
To my dearest wife, by the time you are reading this, I m sure I m no longer around, I bought this policy for you, though the amount is only $100k, I hope it will be able to help me continue my promise that I have made when we got married, I might not be around anymore, I want this amount of money to continue taking care of you, just like the way I will if I could have live longer. I want you to know I will always be around, by your side. I love you.
One first-year student from Guangdong who received 500 yuan as a donation, said, I don t want others to know I am a poor student. If I have to do that, I would rather not accept the donation.
Defect size is also a consideration.A large cavity increases the risk of infection and hematoma[6].Some researchers suggest that when the size of the defect reaches 1-2 cm or 50% of the circumference of the bone,complete healing cannot happen spontaneously[8].However,we learn from previous studies that jaw bone has high regenerative capacity.Ihanassessed bone defects smaller than 3 cm and reported 97% bone density for the surrounding healthy bone after 12 mo[39].For lesions exceeding 4 cm,the reduction of residual defects was over 90% after 24 mo[40].On the other hand,the thickness and structure of the mandible and maxillary limit the size of cysts to a certain degree.In recent years,decompression has been applied for large cysts which may cause fracture.Therefore,cysts before enucleation were usually less than 4 cm in diameter.When deciding on the best treatment for jaw cysts,defect size should be considered in combination with other factors,such as the position of the defect,the conduction of decompression,and the systematic health condition.
Cystectomy is the basic treatment for bone cysts and may be combined with decompression[5].After cystectomy,spontaneous bone healing occurs to repair the bone defect[6].However,decompression and enucleation are not always sufficient to achieve complete bone regeneration,and the process of healing can be long.The extended healing time increases the risks of bone fracture and infection.
In particular,unlike defects in other bones,jaw defects often require complete healing within a certain time period to offer good bone conditions for implantation and tooth construction[44].Under this condition,bone grafting has an obvious advantage with regard to short-term efficacy[26,45].
We took turns joining the Christmas party in the waiting room. Each nurse took his or her lunch break with the family, choosing to spend his or her off?duty time with these people whose laughter and delightful15 chatter16 became quite contagious17.
Studies were included according to the following criteria:(1)Published in English;(2)Maxillofacial bone cystic lesions treated by cystectomy or bone grafting;(3)Published within the time range(last ten years: 2011.12.1-2021.12.1);(4)Randomized clinical trials,controlled clinical trials,and before-and-after studies;(5)Sample size greater than 5 in each treatment group;and(6)Radiology assessment of bone regeneration pre- and post-contrast.
Another source of uncertainty is the difference in experimental design.Most articles are retrospective before-and-after studies;thus,the follow-up time differs across studies.However,in defects,bone regeneration changes over time.Therefore,it is impossible to perform precise estimations and metaanalyses.In addition,not all research teams performed group analysis based on the initial size of defects,creating more limitations to analysis.Other variables,such as histology type and age,were also not controlled for.A randomized clinical trial,which is rare,is the ideal method to investigate the efficacy of bone grafts.Further studies with better variable control and experimental design are needed to investigate these issues.
Limitations and future research directions
The differences in the methods used for bone regeneration assessment were the most significant limitation in this review.Due to the incompleteness of data from each study,errors occurred during speculation and conversion in terms of diameter,area and volume.Theoretically,the reduction of defect volume is the most accurate indicator for bone regeneration.However,CBCT and other techniques were not widely applied in the studies.In addition,when bone grafts are used,the volume of the defect,which is determined using CBCT or X-rays,can be interfered by graft density.To address the limitations of CBCT,some other criteria have been suggested.Kattimani[22]proposed criteria based on the outline of bone defects and bone density changes,but the criteria were slightly different from those proposed by Nakkeeran.Therefore,general and well-recognized criteria for bone healing should be agreed upon and applied in future studies.
In summary,bone grafts can be applied only after taking into consideration the following factors:(1)Whether the periosteum is lost or the contour of bone is detracted by the cyst;(2)Whether the cyst is relatively large;(3)Whether rapid bone formation or implantation is emergent;and(4)Whether any factors associated with failure are present,for example,infection before surgery.
CONCLUSlON
The results of this systematic review show that the advantage of bone grafting after cystectomy for bone regeneration is not proven in jaw cystic lesions.However,combined with previous studies,this review also strengthens the idea that bone grafts accelerate the process of healing and significantly increase bone quality.There is a need for future studies with better assessment methods,variable control and strict randomized design.
ARTlCLE HlGHLlGHTS
Research background
Bone grafts have been widely applied in orthopedic surgery,but their efficacy in relation to bone regeneration in jaw cystic lesions remains unclear.
Research motivation
To identify whether bone grafts are beneficial for bone regeneration in jaw cystic lesions and when bone grafts should be used.
We didn t tolerate bigotry15 on the field, either. Any difference in race, creed16 and class immediately dissolved in the common aim of a team win. Divisiveness only weakens a team. It has no place in a huddle17, on or off the field.
Research objectives
To study the level of bone regeneration after bone grafting compared to spontaneous healing in the treatment of jaw cystic lesions.
Research methods
A literature search was performed in Medline,Cochrane Library and Embase to identify related articles published in English in the last ten years.Articles without assessment of bone regeneration or uniform follow-up time were excluded.Case reports,clinical trials,clinical studies,observational studies and randomized controlled trials were included.
The first part might be left out, but it gives us a few particulars, and these are useful We were staying in the country at a gentleman s seat, where it happened that the master was absent for a few days
Research results
Ten studies were included.Over 90% of bone regeneration occurred within 6 mo after bone grafting.The bone regeneration rate after cystectomy ranged from 50% to 100% after 6 mo,but reached over 90%after 12 mo.
Research conclusions
Bone grafts accelerate the process of healing and significantly increase bone quality,but the long-term superiority of bone grafting compared with spontaneous healing after cystectomy is unclear.
Research perspectives
There is a need for future studies with better assessment methods,variable control and strict randomized design,as well as longer follow-up time.
ACKNOWLEDGEMENTS
This work was supported by the investigator-initiated trial "The observation of bone healing after filling with bone grafts of cystic lesions in jaws: a single-center prospective study" at First Affiliated Hospital,School of Medicine,Zhejiang University.
FOOTNOTES
Wang J and Zhu HY designed the research;Wang J and Yao QY performed the literature research and data analysis;Wang J performed the drafting of paper;Zhu HY made the final approval;all authors have read and approved the final manuscript.
All the authors declare that they have no competing interests.
The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Jin Wang 0000-0003-3402-6658;Qiu-Yun Yao 0000-0002-7785-4608;Hui-Yong Zhu 0000-0003-0883-5355.
Ma YJ
Webster JR
Ma YJ
杂志排行

World Journal of Clinical Cases的其它文章
- Malignant struma ovarii with papillary carcinoma combined with retroperitoneal lymph node metastasis:A case report
- Upper gastrointestinal bleeding from a Mallory-Weiss tear associated with transesophageal echocardiography during successful cardiopulmonary resuscitation:A case report
- lpsilateral hemifacial microsomia with dextrocardia and pulmonary hypoplasia:A case report
- Esophageal myoepithelial carcinoma:Four case reports
- Turner syndrome with primary myelofibrosis,cirrhosis and ovarian cystic mass:A case report
- Acute coronary artery stent thrombosis caused by a spasm:A case report