Evaluating the accuracy of American Society for Gastrointestinal Endoscopy guidelines in patients with acute gallstone pancreatitis with choledocholithiasis
2022-06-11SupisaraTintaraIshaniShahWilliamYakahAwaisAhmedCristinaSorrentoCinthanaKandasamyStevenFreedmanDarshanKothariSunilSheth
Supisara Tintara, Ishani Shah, William Yakah,Awais Ahmed, Cristina S Sorrento, Cinthana Kandasamy,Steven D Freedman,Darshan J Kothari, Sunil G Sheth
Abstract
Key Words: American Society for Gastrointestinal Endoscopy guidelines; Choledocholithiasis; Acute gallstone pancreatitis; Endoscopic retrograde cholangiopancreatography; Magnetic resonance cholangiopancreatography
INTRODUCTION
Acute gallstone pancreatitis (AGP) is the most common cause of acute pancreatitis (AP) in the United States[1 ]. Patients with AGP may also present with choledocholithiasis as the occurrence of common bile duct (CBD) stones is present in up to 15 % of patients with gallstones[2 ]. The diagnosis of choledocholithiasis is challenging and requires a high degree of suspicion as it often cannot be made conclusively without invasive procedures like endoscopic retrograde cholangiopancreatography (ERCP)[3 ]. In 2010 , the American Society for Gastrointestinal Endoscopy (ASGE) suggested a management algorithm based on probability for choledocholithiasis to assist in risk stratifying patients[4 ]. These guidelines stratify patients into those with high, intermediate, and low risk based on clinical criteria,liver tests, and abdominal ultrasound. High risk (> 50 % probability of choledocholithiasis) is defined as the presence of any very strong predictor (clinical ascending cholangitis, CBD stone seen on ultrasound,and/or total bilirubin > 4 mg/dL) or the presence of both strong predictors (CBD dilated more than 6 mm and bilirubin 1 .8 -4 mg/dL). Intermediate risk (10 %-50 % probability of choledocholithiasis) is defined as presence of age > 55 , clinical gallstone pancreatitis, any other abnormal liver test. Finally, low risk patients do not have any of these features[4 ].
These guidelines aim to provide evidence-based recommendations with the goal of optimizing the efficacy and safety of patient care by minimizing the morbidity and cost from unnecessary invasive biliary evaluation. Furthermore, they recommend imaging [i.e.magnetic resonance cholangiopancreatography (MRCP) or endoscopic ultrasound (EUS)] for patients with intermediate risk and ERCP for patients with high probability of choledocholithiasis[4 ].
In 2019 , the ASGE guidelines were updated using more specific criteria to categorize individuals at high-risk for choledocholithiasis[5 ]. These updated criteria propose that high-risk patients are those with elevated total bilirubin > 4 mg/dL and dilated CBD. The presence of only elevated total bilirubin >4 or total bilirubin 1 .8 -4 with dilated CBD are no longer in the criteria for the high-risk group. These guidelines still recommend ERCP for those with high risk and imaging (MRCP or EUS) for those with intermediate risk for choledocholithiasis[6 ]. Additionally, clinical gallstone pancreatitis was removed as one of the criteria for assigning intermediate risk[6 ].
Neither ASGE guideline has been studied in AGP to determine the probability of having choledocholithiasis. Thus, our study aimed to determine the true incidence of choledocholithiasis in patients with AGP and determine compliance with the guidelines at our institution and assess outcomes when guidelines were not adhered to. In our patient population of AGP, we also evaluated the performance and diagnostic accuracy of 2019 vs 2010 ASGE criteria for suspected choledocholithiasis in patients with AGP.
MATERIALS AND METHODS
Data source, patient selection and study design
This retrospective observational cohort study was approved by Beth Israel Deaconess Medical Center institutional review board. This manuscript adheres to the applicable STROBE reporting guidelines for cohort studies.
We performed a review of all adult (age > 18 ) patients with a discharge diagnosis of AP who were admitted to our tertiary center between January 1 , 2008 and December 31 , 2018 . The diagnosis of AP was confirmed by a review of the electronic medical record to ensure all patients met the 2012 Revised Atlanta Criteria for the diagnosis of AP (at least two of the following three criteria: epigastric pain,elevation of serum lipase level > three times the upper limit of normal, and/or evidence of pancreatitis on cross-sectional imaging)[7 ]. Patients with chronic pancreatitis or known pancreatic malignancy were excluded from the study. AGP was defined as the presence of gallstones on imaging or with cholestatic pattern of liver injury in the absence of another cause. Patients who directly went to surgery for cholecystectomy without having either MRCP or ERCP were excluded.
Several parameters including demographic, clinical, laboratory, and radiologic data of the study population were collected. The severity of AP was defined based on the 2012 Revised Atlanta Criteria with mild defined as AP without any local or systemic complications, moderately severe as AP with transient (< 48 h) end-organ failure with or without local complications), and severe as AP with persistent (> 48 h) end-organ damage with or without local complications)[7 ]. The severity of AP in each patient was also characterized based on the bedside index for severity of AP (BISAP) score[8 ,9 ].
Study groups and outcomes of interest
Our cohort of interest was divided based on their risk for choledocholithiasis. These included: low,intermediate or high risk based on the 2010 ASGE guidelines. Since the guidelines defined AGP as at least intermediate risk, no patients were in the low risk category, thus leaving only two groups. We then compared demographic characteristics, comorbidities, and outcomes between the two groups.
Our primary outcomes of interest were the proportion of patients in the intermediate risk group undergoing MRCP first and the proportion of patients in the high risk group undergoing ERCP directly without preceding imaging. Secondary outcomes of interest included outcome differences based on if guidelines were not adhered to. We then evaluated the diagnostic accuracy of the 2019 in comparison to the 2010 ASGE criteria for patients with suspected choledocholithiasis. Additionally, we calculated the sensitivity and specificity of the 2010 and 2019 ASGE guidelines for patients categorized as high risk and intermediate risk for choledocholithiasis. Evidence of choledocholithiasis on ERCP was used as the gold standard for true positives.
Statistical analysis
All data analysis was performed using R software (version 3 .6 .1 , R Core Team 2018 a) within RStudio(version 1 .1463 , RStudio, Inc) via the tidyverse (Wickham, 2017 ) package. Continuous variables were presented as means with range and standard deviation. These were analyzed using thet-test or Wilcoxon rank sum test, as appropriate. Categorical variables were presented as frequencies (%) and analyzed using the Pearsonχ2test or Fisher’s exact test, as deemed appropriate. Univariate analyses comparing several characteristics and outcomes between the two groups were performed. A significantPvalue was assigned at 0 .05 . To determine concordance between the 2019 and 2010 guidelines, Kappa coefficients were calculated to measure the degree of agreement between pairs of variables.
RESULTS
Patient characteristics
In our cohort, 882 patients with AP were hospitalized of which 235 patients had AGP. Seventy-nine patients were excluded as they went directly to surgery for cholecystectomy without prior MRCP or ERCP. These 79 patients had mild AP with resolution of abdominal pain and rapid normalization of liver enzymes suggesting that CBD stones had likely already passed. Moreover, these patients had abdominal ultrasound that showed normal size CBD. Thus, these patients directly underwent cholecystectomy without preceding ERCP or MRCP.
Of the remaining 156 patients, 79 patients were categorized as intermediate risk (Tables 1 and 2 ) and 77 patients were high risk (Tables 3 and 4 ) for choledocholithiasis according to the 2010 ASGE guidelines.
Baseline characteristics and demographics are summarized in Table 5 . When comparing demographics between the intermediate risk and high risk groups, there was no difference in age,gender, race, Charlson Comorbidity Index, severity of pancreatitis and baseline BISAP. Patients in the high risk group had a higher BMI than those in the intermediate group (29 .0 vs 29 .6 , P = 0 .05 ). While most of the baseline laboratory data were similar in both groups, total bilirubin was significantly higher in the high risk group (4 .04 mg/dL vs 1 .32 mg/dL, P < 0 .01 ). Further, alanine aminotransferase and alkaline phosphatase were higher in the high risk groups and approached significance (335 IU/L vs 241 IU/L,P= 0 .06 and 196 IU/L vs 156 IU/L, P = 0 .07 , respectively) (Table 5 ).
Intermediate risk
Seventy-nine patients were assigned to have intermediate risk of choledocholithiasis based on the 2010 ASGE criteria. In this group, 45 were older than 55 years-old, 73 had abnormal liver tests and 22 had dilated CBD or total bilirubin of 1 .8 -4 .0 mg/dL (Table 1 ). Thirty-three patients met all 4 criteria for intermediate risk group, while 45 patients met 3 criteria, 1 patient met 2 criteria and no patients metonly 1 criterion (Table 2 ).

Table 1 Patients categorized as intermediate risk for choledocholithiasis, n = 79
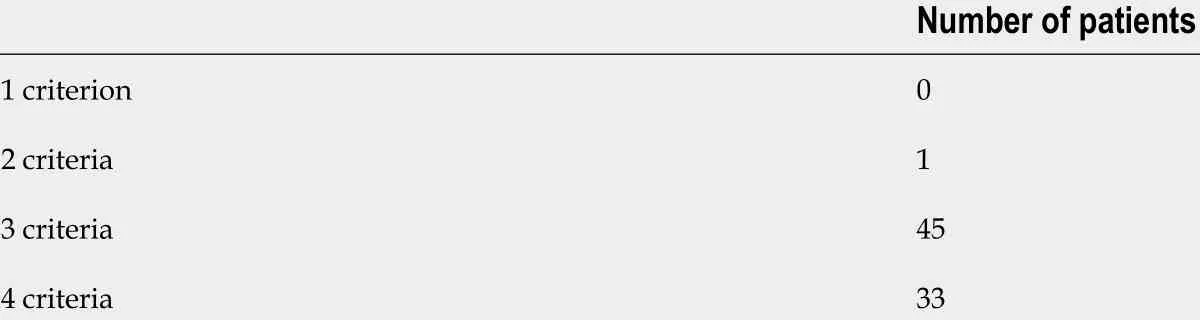
Table 2 Number of criteria met for patients categorized as intermediate risk for choledocholithiasis, n = 79

Table 3 Patients categorized as high risk for choledocholithiasis, n = 77
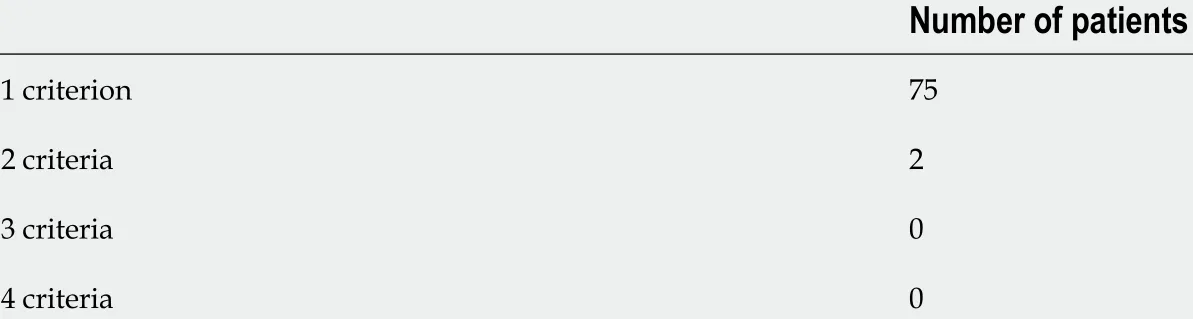
Table 4 Number of criteria met for patients categorized as high risk for choledocholithiasis, n = 77
Among 79 intermediate risk patients, 54 (68 %) underwent MRCP first whereas 25 patients (32 %) went directly to ERCP (Figure 1 ). For the 54 patients with intermediate risk who had MRCP first, 18 patients had evidence of choledocholithiasis prompting ERCP, while 36 patients had imaging that did not show choledocholithiasis. Of the 18 patients undergoing ERCP after MRCP, 11 patients had choledocholithiasis, whereas 7 patients had normal examinations. There were no complications from ERCP noted in this group.
Of the 25 intermediate risk patients who directly underwent ERCP, 18 patients had choledocholithiasis whereas 7 patients had a normal ERCP (Figure 1 ). Notably, one of these patients with a normal ERCP developed post ERCP pancreatitis. Patients undergoing MRCP first in this group had a significantly longer length of stay (LOS, 5 .0 vs 4 .0 d, P = 0 .02 ). They also had higher incidence of pancreatic necrosis (33 % vs 8 %, P = 0 .03 ) and higher rate of 1 -year readmission (52 % vs 20 %, P = 0 .02 )(Table 6 ). There were multiple causes of readmissions in our cohort such as diverticulitis, autonomic dysfunction, pneumonia and urinary tract infection. The 1 -year readmission rates for recurrence of acute gallstone pancreatitis or choledocholithiasis were 9 % for patients who had MRCP first and 8 % for those who directly underwent ERCP, likely because some of them refused or did not undergo cholecystectomy.
High risk
Seventy-seven patients were assigned to have high risk of choledocholithiasis based on the 2010 ASGEcriteria. In this group, 1 patient was suspected to have cholangitis, 38 patients had total bilirubin > 4 .0 mg/dL, 12 patients had CBD stone on imaging, and 31 patients had dilated CBD with total bilirubin 1 .8 -4 .0 mg/dL (Table 3 ). Seventy-five patients met 1 criterion for high risk group and 2 patients met 2 criteria. No patient met 3 or more criteria (Table 4 ).
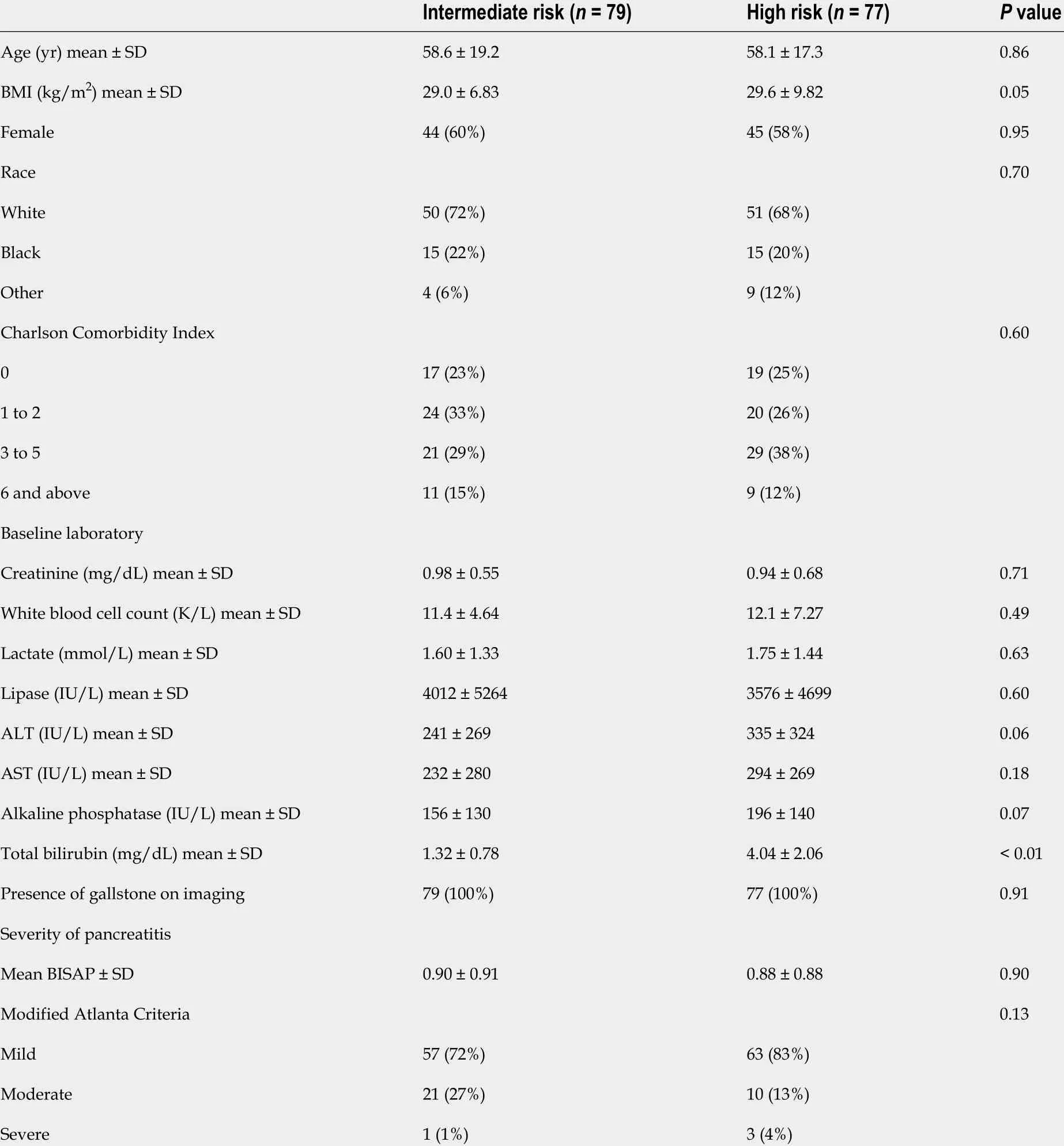
Table 5 Demographics of gallstone pancreatitis patients with intermediate and high risk for choledocholithiasis
In this group, 64 patients (83 %) had ERCP without preceding imaging, of which, 53 patients had findings consistent with choledocholithiasis (27 patients with stones and 26 patients with sludge) while 10 had a normal examination (Figure 2 ). In comparison, 13 patients in this group (17 %) underwent MRCP before ERCP, all of which showed evidence of stone disease. Furthermore, all of these patients ultimately had an ERCP, of which 8 patients had evidence of choledocholithiasis and 5 had normal examination (Figure 2 ). Two of the 13 patients who underwent imaging first due to altered luminal anatomy and body habitus. For the remaining 11 patients, there was no identifiable reason for not directly proceeding to ERCP.
As with the intermediate group, for the high risk group, the MRCP-first group had longer LOS compared to ERCP-first group which approached significance (4 .28 vs 3 .00 days, P = 0 .08 ). There were no significant differences in outcomes such as readmission rate, 1 -year mortality between the two groups (Table 6 ).
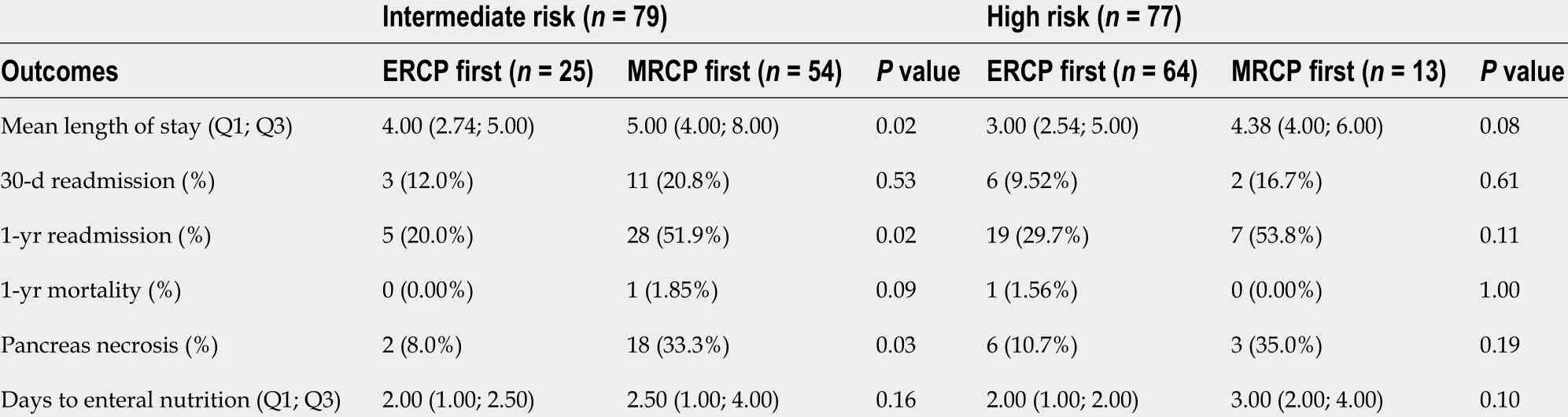
Table 6 Outcomes of patients with intermediate and high risk for choledocholithiasis
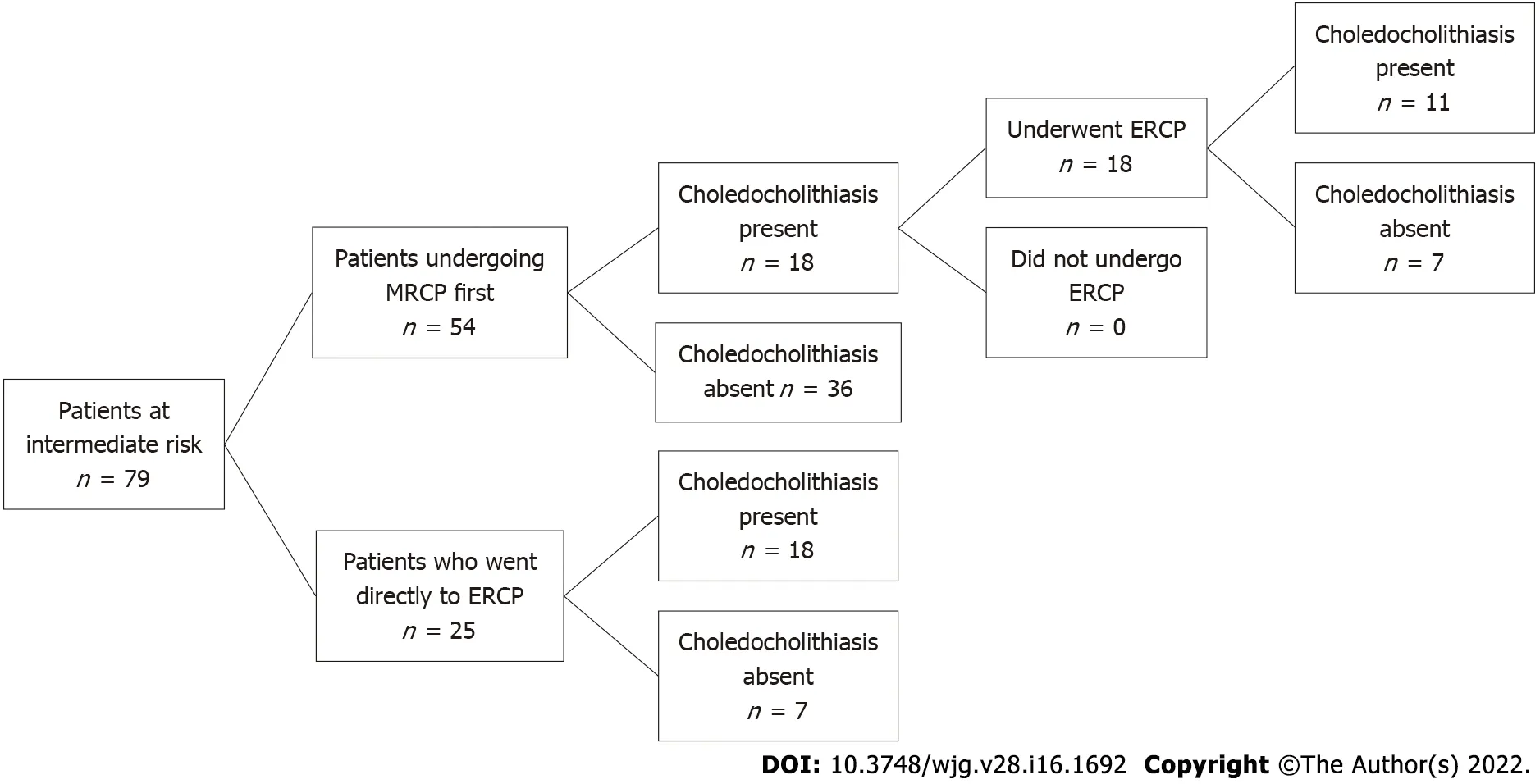
Figure 1 Patients at intermediate risk for choledocholithiasis. MRCP: Magnetic resonance cholangiopancreatography; ERCP: Endoscopic retrograde cholangiopancreatography.
Incidence of confirmed choledocholithiasis in patients with AGP
Our cohort also demonstrated that of all 156 patients with AGP, 90 (58 %) were found to have choledocholithiasis on ERCP. When stratified by assigned choledocholithiasis risk based on the 2010 ASGE guidelines, 61 of 77 patients in the high risk group (79 %) and 29 of 79 patients in the intermediate risk group (37 %) were found to have choledocholithiasis (Figure 3 ).
Comparison to the 2 019 ASGE guidelines
Our cohort of patients was admitted to the hospital between 2008 and 2018 , thus the 2010 ASGE guideline were used in the above analysis. We then applied the 2019 criteria to this group to see how results may have changed. There was moderate agreement between the classifications by the 2010 and 2019 guidelines (kappa = 0 .46 , 95 %CI: 0 .34 -0 .58 ). When the 2019 ASGE guidelines were applied to our 79 patients with intermediate risk for choledocholithiasis, all of these patients were still assigned intermediate risk. Among the 77 patients in the high risk group, when the updated 2019 ASGE guidelines were applied instead of the original 2010 guidelines, 42 patients were still deemed to be high risk and 35 patients were downgraded to intermediate risk. In the high risk group, 34 of 42 who still remained high risk went directly to ERCP of which showed 28 patients had a confirmatory findings of choledocholithiasis and 5 patients had a normal examination (Figure 4 ).
Thirty-five patients who were originally assigned high risk were then reclassified as intermediate risk(Figure 4 ). For these 35 patients, 26 patients had ERCP findings consistent with choledocholithiasis and 9 patients had a normal examination. In further review of those patients with a normal ERCP, 5 patients had a bilirubin of > 4 mg/dL and 4 patients had a dilated CBD and a bilirubin of 1 .8 to 4 mg/dL. Hence,based on the 2019 criteria, 9 out of 35 patients who were downgraded to intermediate risk had an unnecessary ERCP with normal findings (without a preceding MRCP).
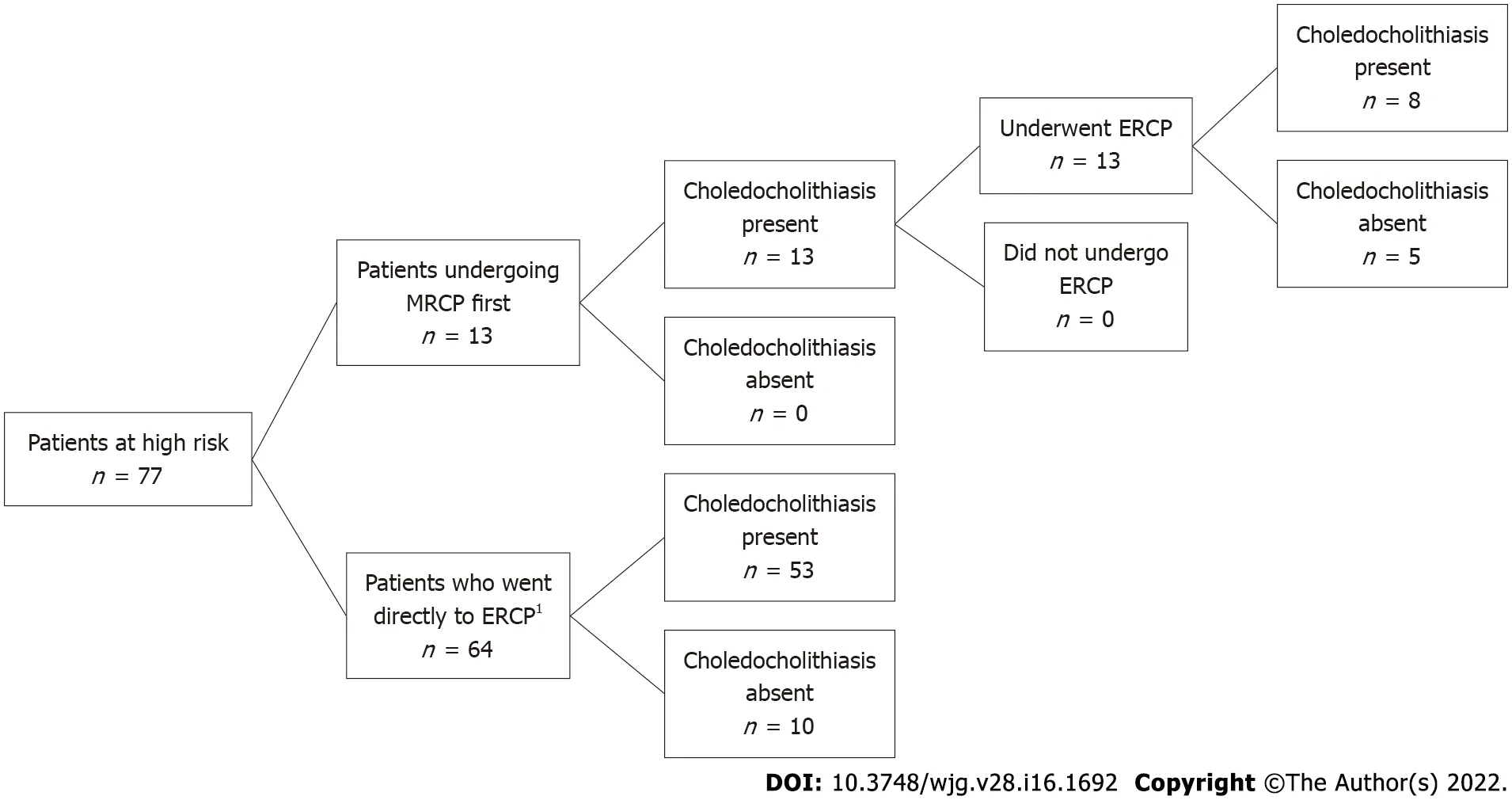
Figure 2 Patients categorized as high risk by American Society for Gastrointestinal Endoscopy guidelines. MRCP: Magnetic resonance cholangiopancreatography; ERCP: Endoscopic retrograde cholangiopancreatography. 1 One patient’s procedure could not be completed due to failure of bile duct cannulization.
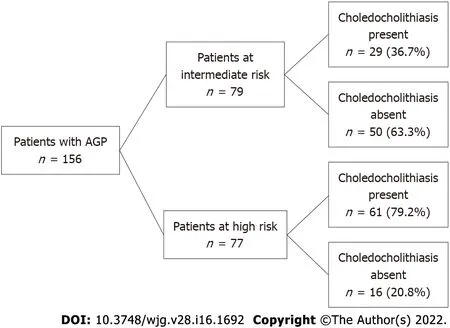
Figure 3 Patients with choledocholithiasis. AGP: Acute gallstone pancreatitis.
Finally, the sensitivity and specificity of the 2010 and 2019 ASGE guidelines in assessing choledocholithiasis were calculated (Tables 7 -10 ). In our cohort of patients with AGP, the 2010 ASGE criteria for predicting high risk for choledocholithiasis had a sensitivity of 67 .8 % and specificity of 75 .8 %. On the other hand, the 2019 ASGE criteria for predicting high risk for choledocholithiasis had a sensitivity of 38 .2 % and specificity of 89 .4 %.
DISCUSSION
AGP is the most common cause of AP in the United States accounting for approximately one-third of all cases[1 ]. Furthermore, given the potential for comorbid choledocholithiasis, patients with AGP should be evaluated for CBD stone disease[2 ]. In our cohort of patients with AGP, 37 % of patients with intermediate risk and 79 .2 % of patients with high risk for choledocholithiasis based on the 2010 ASGEguidelines had documented CBD stone disease. When combined, our data demonstrated that the true incidence of choledocholithiasis in patients with AGP is 58 %. The overall high prevalence of concurrent choledocholithiasis in patients with AGP may help explain the relatively high risk of recurrent pancreatitis in patients with AGP[10 ].

Table 7 Sensitivity and specificity of 2010 American Society for Gastrointestinal Endoscopy guidelines for predicting high risk of choledocholithiasis in patients with acute gallstone pancreatitis

Table 8 Sensitivity and specificity of 2010 American Society for Gastrointestinal Endoscopy guidelines for predicting intermediate risk of choledocholithiasis in patients with acute gallstone pancreatitis

Table 9 Sensitivity and specificity of 2019 American Society for Gastrointestinal Endoscopy guidelines for predicting high risk of choledocholithiasis in patients with acute gallstone pancreatitis

Table 10 Sensitivity and specificity of 2019 American Society for Gastrointestinal Endoscopy guidelines for predicting intermediate risk of choledocholithiasis in patients with acute gallstone pancreatitis
The ASGE published guidelines in 2010 which proposed a risk stratification system to clarify how to best manage patients with suspected choledocholithiasis, categorizing patients into low, intermediate and high risk[4 ].
In this scheme, patients at high risk are recommended to undergo ERCP directly without further imaging and those at intermediate risk should have additional imaging with MRCP or EUS. Those at low risk require no further evaluation. In this study, we aimed to apply these guidelines to patients admitted with AGP to a single tertiary care center over 10 years and determine what effect deviation had on outcomes.

Figure 4 Patients at high risk based on 2010 American Society for Gastrointestinal Endoscopy guidelines now re-stratified based on 2019 guidelines. MRCP: Magnetic resonance cholangiopancreatography; ERCP: Endoscopic retrograde cholangiopancreatography. 1 One patient’s procedure could not be completed due to failure of bile duct cannulization.
In our cohort of 156 patients, approximately one-half of patients were either classified as intermediate or high risk. Since all patients in our cohort had AGP and the presence of AGP was a criteria for at least intermediate risk for choledocholithiasis according to the 2010 ASGE guidelines, no patients in our cohort were considered low risk for choledocholithiasis. After applying the guidelines to these groups,76 % of patients (54 patients in the intermediate group and 64 patients in the high risk group) were managed in accordance to the ASGE recommendations and 24 % of patients (25 patients in the intermediate group and 13 patients in the high risk group) deviated from the guidelines. Specifically in the intermediate group, 7 patients who had an ERCP first had a normal examination suggesting that an inappropriate procedure was performed and importantly, one of these patients suffered from post-ERCP pancreatitis. These 7 intermediate risk patents who directly underwent ERCP and had normal findings did not receive EUS or MRCP. Thus, it may be prudent to consider EUS to evaluate for choledocholithiasis to prevent unnecessary ERCPs. Furthermore, all 13 of the patients in the high risk group who underwent MRCP prior to ERCP had a positive finding, suggesting an unnecessary test (i.e.MRCP) was performed first. Importantly, patients who underwent MRCP prior to ERCP were found to have longer hospital lengths of stay and delays in initiation of enteral feeding.
The ASGE guidelines provide evidence-based recommendations with the goal of optimizing the efficacy and safety of patient care. Additionally, a study has shown that adherence to ASGE guidelines also result in cost-saving from unnecessary imaging studies[3 ]. Accordingly, patients with intermediate risk (10 %-50 %) should undergo additional imaging because the risk of choledocholithiasis is too low to warrant proceeding directly to ERCP[6 ]. MRCP is often preferred in patients with pancreatitis who have intermediate risk for choledocholithiasis because it has high sensitivity in detecting CBD stones without procedural risks[11 ]. While ERCP is highly sensitive and specific in diagnosis and effective in therapeutic management of choledocholithiasis[12 ], the procedure also has a number of associated risks such as post-ERCP pancreatitis and post-endoscopic sphincterotomy bleeding[13 ,14 ]. One of the intermediate risk patients in our cohort who went directly to ERCP which showed normal findings developed worsening of pancreatitis thought to be related to post ERCP AP. This highlights that unnecessary invasive procedure and adverse outcome could have been prevented by adhering to the guidelines.
In 2019 , the ASGE updated guidelines on management of choledocholithiasis, which further finetuned the criteria needed for the high risk group[6 ]. Specifically, patients now required the presence of a bilirubin greater than 4 mg/dL and imaging with a dilated CBD to qualify as high risk and thus those patients with a total bilirubin of 1 .8 -4 .0 mg/dL with CBD dilation on imaging were downgraded to intermediate risk. The impetus for these changes were largely driven by studies that demonstrated that up to 30 % of patients had ERCPs without evidence of CBD stones[15 ,16 ]. In our study, we found that approximately 26 % (9 /35 ) of patients categorized as high risk by 2019 criteria had a normal ERCP.
Since the cohort we studied was prior to the update, the 2010 guidelines were used in the initial analysis. In our subsequent analysis we aimed to determine concordance in categorization between the 2010 and 2019 guidelines. After applying the 2019 guidelines, we found that all patients in the intermediate group remained the intermediate group, whereas there was less concordance in the high risk group which was largely due to the group of patients who had lower total bilirubin levels.Importantly, using the newer guidelines, 9 patients may have been spared an ERCP. We also found that while the 2010 ASGE guidelines in predicting high risk for choledocholithiasis had a specificity of 75 .8 %,using the 2019 ASGE guidelines led to an improved specificity of 89 .4 %. This demonstrated that the use of the revised guidelines in assessing risk for choledocholithiasis in AGP patients can lead to a decrease in unnecessary invasive and costly procedures. Moreover, although AGP was removed from the intermediate risk criteria, all patients in our intermediate cohort remained intermediate suggesting that AGP implicitly increases the risk to the intermediate level for choledocholithiasis. This was verified in our cohort where 58 % of patients with AGP were confirmed to have choledocholithiasis. Thus, clinicians should remain vigilant for concurrent choledocholithiasis in patients admitted with AGP.
We recognize that our study also has several limitations. First, this is a retrospective cohort study which has a potential for selection bias. The smaller size and retrospective nature of this study may limit the assessment of the degree of adherence to the ASGE guidelines. As the decision to proceed with MRCP or ERCP were at the discretion of the physician on service, the detailed reasoning behind selecting each modality was not always apparent in the medical record. Our results may not be generalizable to all medical settings as this study was done at a single tertiary care center at an academic institution located in a large metropolitan city. Further work is needed to determine the influencing factors driving deviation from the guidelines.
CONCLUSION
In the study cohort, we demonstrated that more than half of patients with AGP have choledocholithiasis. We also found that approximately two thirds of patients in the intermediate group and 83 % of patients in the high risk group followed ASGE guidelines for management of choledocholithiasis in the setting of AGP. There was associated longer LOS for patients undergoing MRCP in both groups.Importantly, one patient who had a normal ERCP in the intermediate group without preceding MRCP suffered from post ERCP AP, highlighting the risk of unnecessary procedures. Further work is needed to determine the influencing factors driving deviation from the guidelines.
ARTICLE HIGHLIGHTS

Research results
Among 79 intermediate risk patients according to the 2010 ASGE guidelines, 54 (68 %) underwent MRCP first whereas 25 patients (32 %) went directly to ERCP. Of the 25 intermediate risk patients who directly underwent ERCP, 18 patients had stone disease. One patient with a normal ERCP developed post ERCP pancreatitis. In the high risk group, 64 patients (83 %) had ERCP without preceding imaging. When the updated 2019 ASGE guidelines were applied instead of the original 2010 guidelines, there was moderate agreement between the 2010 and 2019 guidelines (kappa = 0 .46 , 95 %CI: 0 .34 -0 .58 ). Based on the 2019 criteria, 9 /35 patients who were downgraded to intermediate risk had an unnecessary ERCP with normal findings (without a preceding MRCP).
Research conclusions
In the study cohort, we demonstrated that more than half of patients with AGP have choledocholithiasis. We also found that approximately two thirds of patients in the intermediate group and 83 % of patients in the high risk group followed ASGE guidelines for management of choledocholithiasis in the setting of AGP. Importantly, one patient who had a normal ERCP in the intermediate group without preceding MRCP suffered from post ERCP pancreatitis, highlighting the risk of unnecessary procedures.We also found that while the 2010 ASGE guidelines in predicting high risk for choledocholithiasis had a specificity of 75 .8 %, using the 2019 ASGE guidelines led to an improved specificity of 89 .4 %.
Research perspectives
Further work is needed to determine the influencing factors driving deviation from the guidelines.
ACKNOWLEDGEMENTS
The authors would like to thank the Harvard Catalyst Biostatistics Consulting Program at Beth Israel Deaconess Medical Center for reviewing statistical methods and reporting of results.
FOOTNOTES
Author contributions:Tintara S, Shah I, Ahmed A, Freedman SD, Kothari DJ and Sheth SG contributed to the study design and coordination; Tintara S contributed to the acquisition and interpretation of data, and primarily drafting the manuscript; Shah I assisted in drafting the manuscript; Yakah W contributed to the acquisition and interpretation of data and statistical analysis; Ahmed A, Sorrento CS and Kandasamy C contributed to the acquisition of data;Freedman SD contributed to revision of manuscript for intellectual content; Kothari DJ and Sheth SG contributed to the interpretation and analysis of data, revision of manuscript for intellectual content, and study supervision; All authors have approved the final draft submitted.
Institutional review board statement:This retrospective observational cohort study was approved by Beth Israel Deaconess Medical Center institutional review board.
Informed consent statement:Informed written consent was obtained fromthe patient for publication of this report and any accompanying images.
Conflict-of-interest statement:The authors of this study have no relevant conflict of interests to declare.
Data sharing statement:Statistical code, and dataset available from the corresponding author at ssheth@bidmc.harvard.edu. This retrospective observational cohort study was approved by the Beth Israel Deaconess Medical Center institutional review board which did not require individual patient consent for retrospective chart review.
STROBE statement:This manuscript adheres to the applicable Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cohort studies.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4 .0 ) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4 .0 /
Country/Territory of origin:United States
ORCID number:Supisara Tintara 0000 -0002 -9427 -2845 ; Ishani Shah 0000 -0003 -2916 -1089 ; William Yakah 0000 -0003 -3264 -5404 ; Awais Ahmed 0000 -0001 -7254 -5921 ; Cristina S Sorrento 0000 -0002 -1111 -5271 ; Cinthana Kandasamy 0000 -0002 -4235 -6932 ; Steven D Freedman 0000 -0003 -1255 -9701 ; Darshan J Kothari 0000 -0002 -6835 -218 X; Sunil G Sheth 0000 -0003 -0602 -8509 .
S-Editor:Zhang H
L-Editor:A
P-Editor:Zhang H
杂志排行

World Journal of Gastroenterology的其它文章
- Comment on “Artificial intelligence in gastroenterology: A state-of-the-art review”
- Viral hepatitis: A global burden needs future directions for the management
- Aspartate transferase-to-platelet ratio index-plus: A new simplified model for predicting the risk of mortality among patients with COVID-19
- Small nucleolar RNA host gene 3 functions as a novel biomarker in liver cancer and other tumour progression
- Noninvasive imaging of hepatic dysfunction: A state-of-the-art review
- Risk of venous thromboembolism in children and adolescents with inflammatory bowel disease: A systematic review and meta-analysis