Factors that affect heart rate variability following acute resistance exercise:A systematic review and meta-analysis
2022-06-09SjithMrsinghArchchigeJcooRuioArisPedroAlcrzLindChung
Sjith U.Mrsingh-Archchige,Jcoo ´A.Ruio-Aris,Pedro E.Alcrz,c,Lind H.Chung,c,*
a UCAM Research Center for High Performance Sport,Catholic University of Murcia,Murcia 30107,Spain
b LFE Research Group,Department of Health and Human Performance,Faculty of Physical Activity and Sport Science-INEF,Universidad Polit´ecnica de Madrid,Madrid 28040,Spain
c Faculty of Sport,Catholic University of Murcia,Murcia 30107,Spain
Received 23 June 2020;revised 19 September 2020;accepted 28 September 2020
Available online 24 November 2020
2095-2546/© 2022 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.
(http://creativecommons.org/licenses/by-nc-nd/4.0/)
Abstract Background:There is controversial evidence regarding the effect of acute resistance exercise(ARE)on heart rate variability(HRV)parameters,which indicates the activities of the cardiac autonomic nervous system.The aim of this study was to perform a systematic review and meta-analysis of the literature on the effect of ARE on HRV parameters and identify its possible moderating factors. Methods:The PubMed-Medline,Web of Science,SPORTDiscus,and Cochrane Library databases were searched.The Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)declaration was followed,and the methodological quality of the studies was evaluated.The level of significance was set at p ≤0.05.Twenty-six studies met the inclusion criteria.Main effect analyses between pre-and post-test interventions demonstrated an increase in normalized units low frequency(p <0.001;standardized mean difference(SMD)=0.78;95%confidence interval(95%CI):0.46-1.11)and low frequency/high frequency ratio(p <0.001;SMD=0.82;95%CI:0.64-0.99)and a decrease in standard deviation of the normal-to-normal(NN)interval(p <0.001;SMD=-0.58;95%CI:-0.85 to-0.30),root mean square of the successive differences(p <0.001;SMD=-1.01;95%CI:-1.29 to-0.74),and normalized units high frequency(p <0.001;SMD:-1.08;95%CI:-1.43 to-0.73)following ARE in healthy individuals range:15±1 to 48±2 years;mean±SD). Results:There were differences between the subgroups in the number of sets used in an exercise(p=0.05)for root mean square of the successive differences,as well as for exercise intensity(p=0.01)and rest between sets(p=0.05)for normalized units high frequency.Interestingly,there were differences between the subgroups in training volume for root mean square of the successive differences(p=0.01),normalized units high frequency(p=0.003)and normalized units low frequency(p=0.02). Conclusion:Overall,there was a withdrawal of cardiac parasympathetic and activation of cardiac sympathetic modulations following ARE,and these changes were greater with higher training volume ~30 min after ARE in healthy individuals.Furthermore, the number of sets, intensity,and rest between sets affected HRV parameters.However, gender, body mass index, and training status did not influence the changes in HRV parameters as a response to ARE.
Keywords: Cardiac;Parasympathetic;Sympathetic
1.Introduction
Resistance training plays an integral role in competitive athletes’ training programs and is also widely used by recreationally active individuals to enhance their physical qualities(e.g., muscle strength, power output, and speed) and body composition (bone mass and muscle mass).More important,resistance training is used to reduce the risk of injury occurrence.1,2According to the National Strength and Conditioning Association (NSCA), resistance training entails a wide range of resistive loads and a variety of training modalities to optimize the effects of training and improve sports performance and overall health.3Physiological adaptation requires an adequate exercise stimulus to achieve training and performance goals.Furthermore, proper recovery from such training stressis necessary because the body may be exposed to continuous training-induced fatigue, which could lead to non-functional overreaching or overtraining and, ultimately, to fatigue syndrome.4In a highly competitive environment, the most efficient and optimal recovery time is one of the major objectives of sports coaches and fitness trainers since it allows more time for improving an athlete’s performance(i.e.,more training sessions,better training adaptations and less risk of injuries).To address the recovery status, recent studies have shown that heart rate variability (HRV) parameters, such as root mean square of the successive differences (RMSSD), normalized units low frequency (LFnu), normalized units high frequency (HFnu), and low frequency/high frequency(LF/HF) ratio, could be used as a physiological monitoring tool for recovery5-8and standard deviation of the normal-to-normal (NN) interval (SDNN) to understand the overall autonomic modulation.7
HRV is the physiological variation in the time interval between heart beats.9The time between successive heartbeats is never constant and can vary slightly even when the heart rate appears stable.10Previous studies have reported that acute resistance exercise (ARE) increases the cardiac sympathetic modulation while decreasing the cardiac parasympathetic modulation.11-16During post-exercise recovery, the early phase of post-exercise is characterized by sympathetic predominance,and the cardiac parasympathetic stimulation is the predominant autonomic activity.17Changes in cardiac sympathetic and parasympathetic modulation can be monitored by examining HRV parameters.18-20Thus,adjusting the protocol of the ARE session according to the recovery status of the cardiac autonomic modulation(i.e.,HRV)could be advantageous in optimizing the microcycle periodization,thereby increasing training adaptation and performance and, most importantly,avoiding injuries and overtraining.
The parameters of HRV are altered following an ARE session, and the magnitude of change may depend on the characteristics of the resistance training protocol, such as the number of repetitions, sets, rest time between sets, amount of exercise per workout,intensity(based on 1 repetition maximum(1RM))and volume.In a review by Kingsley and Figueroa21that examined 10 studies published before 2014,cardiac parasympathetic modulation decreases (i.e., ↓HFnu) and cardiac sympathetic modulation increases(i.e.,↑LFnu and ↑LF/HF ratio)following a resistance training session in healthy young men and women.Since then, several experimental studies have examined the effect of ARE on HRV.14,22-39However, there are some discrepancies in the findings since some studies show the opposite effect on HRV parameters following an ARE session.14,32,39,40Furthermore, it is unclear what the magnitude of the ARE has on HRV parameters.Additionally, to our knowledge, no study has investigated (i.e., meta-analyses) the possible moderating factors of ARE that affect HRV parameters.
The overall goal of this systematic review and meta-analysis was to understand how an ARE session affects the HRV characteristics and identify the possible moderating factors that contribute to the cardiac autonomic activity during post-exercise recovery.Moreover,findings from this systematic review and meta-analysis may benefit the scientific community in better understanding how an ARE session affects the cardiac autonomic modulation,as well as in providing a monitoring tool for fitness trainers and coaches with regards to determining the athlete’s recovery level.Therefore,the objectives of the present study were to (1) systematically review and conduct a meta-analysis of the studies that have investigated ARE on HRV parameters and(2)determine the factors that could affect the recovery process of cardiac autonomic modulation following an ARE session.
2.Methods
The recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) declaration41were followed during this methodological process.
2.1.Data sources
A comprehensive literature search was performed using PubMed—Medline, Web of Science, SPORTDiscus, and Cochrane Library electronic databases,from inception through November 30, 2019.The keywords and categorical searches were (1) “heart rate variability” OR “HRV” OR “vagal” OR“autonomic function” and (2) “resistance training” OR“strength training”OR“weight training”OR“power training”OR “weightlifting” OR “full body” OR “circuit*” OR“neuromuscular training” OR “bodyweight training”.Second,the Boolean operator AND was used to combine categories(1)and (2).Additional records were identified while reviewing the reference lists of the books written in the relevant area.
2.2.Selection criteria
The eligibility criteria were pre-established by the authors.The inclusion criteria of articles included the following: (1)the study examined ARE on HRV after 1 training session, (2)study participants were healthy individuals or athletes (males or females), (3) the study gave a detailed explanation of the resistance training protocol,(4)the study provided information on outcomes both at baseline and following intervention, (5)the study reported data that was recorded between 8 and 30 min after the intervention, and (6) the study included at least 1 ARE training intervention group.Research studies were excluded for any of the following reasons: (1) the study had a sample population with pathologies, (2) the study was not an original investigation published in a peer-reviewed journal, (3) the study did not specify the test battery to be evaluated, (4) the study did not provide relevant data in the published article or if the corresponding author did not provide the data after being contacted, or (5) the study had methodological issues that may have led to potential risk of carryover effects due to inadequate recovery period(≤24 h).
2.3.Study selection,data extraction,and outcomes
Two of the authors(SUMA and JARA)conducted the electronic database search and selection of included studies according to the previously established criteria.Any disagreements regarding the inclusion/exclusion of articles were discussed and resolved by consensus.The following data were extractedfrom the selected articles:authors,number of participants,subject characteristics,exercise protocol,and outcomes of selected HRV parameters,including SDNN,RMSSD,HFnu,LFnu,and LF/HF ratio, since these are the most examined HRV parameters in other studies.42-45RMSSD and HFnu indicate the level of cardiac parasympathetic modulation,42,45while LFnu provides the degree of cardiac sympathetic modulation.43,45The LF/HF ratio presents the extent of sympathovagal balance,and SDNN represents overall autonomic modulation.45Thus, an increase in cardiac sympathetic modulation corresponds to an increase in LFnu and LF/HF ratio,while the dominance of cardiac parasympathetic modulation is shown by an increase in RMSSD and HFnu parameters.
2.4.Data synthesis
Data on the mean ± SD and sample size (n) were recorded from the included articles by one author(SUMA)and confirmed by a second author (JARA).The corresponding author of each included article was contacted if necessary data were not available in the published version.When studies reported 2 or more subgroups, the subgroups were combined into a single group in accordance with the Cochrane Handbook for Systematic Reviews of Interventions.46For studies that include pre-and post-intervention measurements,SD and n values were uploaded to the Review Manager software (RevMan 5.3; Cochrane Collaboration,Oxford,UK).In addition,mean,SD,and n values of the studies that included experimental and control groups were also uploaded.For each study, the mean difference (MD), change in SD and 95% confidence intervals (95%CIs) were calculated between pre- and post-intervention (i.e., differences within groups)and between experimental and control groups.
2.5.Meta-analyses
Meta-analyses were conducted on the changes in each outcome using Review Manager software.Since SDNN,RMSSD,LFnu, HFnu, and LF/HF ratio data were measured using different time durations (i.e., time period of collected data) or were presented using different units (e.g., natural logarithm or milliseconds squared), the MDs were standardized by dividing the values by their corresponding SDs and were weighted according to the inverse variance method.The standardized MD(SMD)in SDNN,RMSSD,LFnu,HFnu,and LF/HF ratio data for each study was pooled with a random-effects model.46The data analysis focused on the magnitude of the effects obtained.
2.6.Heterogeneity and risk of bias
The statistical heterogeneity between studies was evaluated using the Cochrane χ2test (I2).I2values of <30%,30%-60%,and >60%were considered as low,moderate,and high levels of heterogeneity, respectively.A p value of ≤0.05 from the χ2test suggested the presence of heterogeneity,47which was likely due to the methodological diversity of the studies.Methodological quality was evaluated using the Study Quality Assessment Tools developed by the National Heart,Lung, and Blood Institute.48The tool for Quality Assessment of Controlled Intervention Studies was used for studies that included control groups, and the tool for Quality Assessment for Pre-Post Studies with No Control Group was used for studies that included only an experimental group.Publication bias was evaluated by analyzing the funnel plot asymmetry test.
2.7.Subgroup analyses
In our study,we decided to perform subgroup analyses using categorical variables and continuous variables without conducting meta-regression analysis for continuous variables.The reason for representing continuous variables as categorical variables for the subgroup analyses was to match the way these variables are presented by organizations like the NSCA.For example,the NSCA generally provides recommendations for training protocols (e.g.,high intensity >85%1RM,low intensity <65%1RM).Thus,we believe that it is important to analyze the data in ways similar to practical scenarios in order to reduce the gap between the scientific evidence and practical application in resistance training sessions in the field or gym.Therefore, we performed subgroup analyses while considering the way resistance training sessions are practiced in the field,as well as the way they are presented in the NSCA guidelines.1,49,50
Subjects characteristics(gender,body mass index(BMI),and training status) and training characteristics (training intensity(% 1RM),number of repetitions,sets,rest between sets,amount of exercise per workout and training volume (number of repetitions×sets×exercises)) were assessed by subgroup analysis to examine their effect on selected HRV parameters.For BMI,≤24.9 kg/m2(healthy weight)or >24.9 kg/m2(overweight)were considered as cut-off values,based on guidelines from the Centers for Disease Control and Prevention.51For gender, male and female were used for grouping trials.For resistance training variables, the cut-off values for grouping trials were determined by considering the way resistance training sessions are conducted in the field and the NSCA guidelines.1,49,50High (>85% 1RM),moderate (>65%-85% 1RM), and low (≤65% 1RM) values were used as cut-off points for training intensity.1,49,50Bodyweight as an intensity level was not included in the subgroup analysis.For the number of repetitions,<6,6-10,and >10 repetitions were used as cut-off values.For the number of sets,cut-off values were set at <3,exactly 3,and >3 sets;and for the amount of exercise, <6, exactly 6, and >6 exercises per workout were used as cut-off values.For resting time between sets, <2 min,exactly 2 min,and >2 min were used as cut-off points.Regarding training volume (calculated as the number of repetitions×sets×exercises), cut-off points were set at <108 (low),108 to <180 (medium), and ≥180 (high).Changes in possible moderating factors were expressed and analyzed as the difference between post- and pre-intervention values.Subgroup analyses were performed using Review Manager software.
3.Results
3.1.Study selection
From the initial electronic database search and other sources, 1449 records were identified.After removal ofduplicates, 1076 titles and abstracts were evaluated, and 1003 were excluded.Thus, the full text of 73 articles was assessed to determine eligibility for the inclusion of studies,and 2 additional studies were screened as a result of reviewing the reference lists.From these studies, 49 articles were excluded because they did not meet the inclusion criteria.After review, a total of 26 studies were included in the systematic review and meta-analysis.14-16,22-31,34-40,52-57All included articles were published between 2006 and 2019(Fig.1).
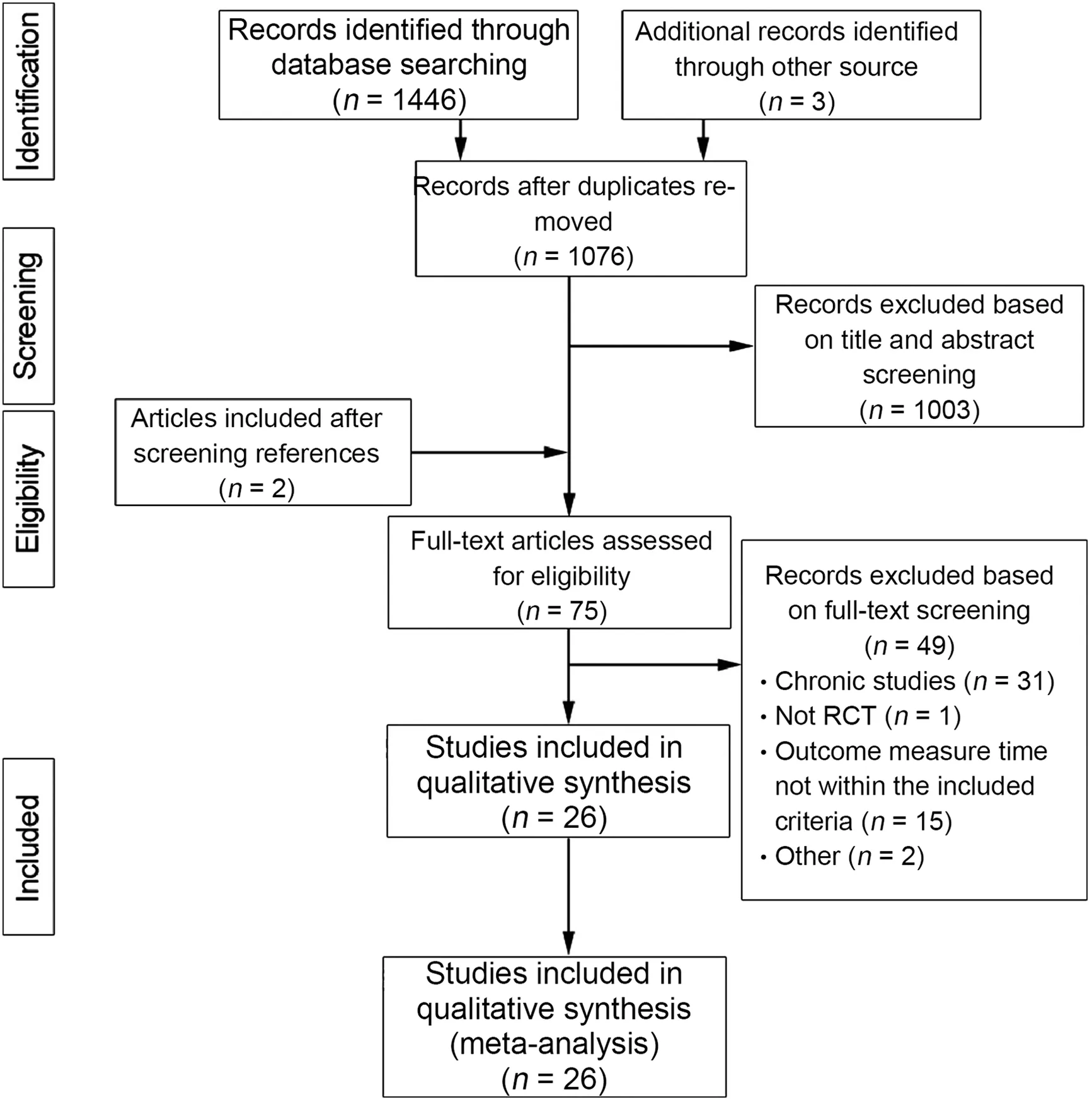
Fig.1.Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA) flow diagram regarding article selection for each stage of the systemic eligibility process.RT=resistance training.
3.2.Characteristics of the interventions
Subjects were healthy and physically active,and the majority were resistance-exercise-trained individuals.Their age ranged between 15 ± 1 and 48 ± 2 years (mean ± SD).The samples included both males and females.BMI(SD)ranged from 20.0±1.0 kg/m2to 27.5 ± 2.1 kg/m2, although some studies did not report BMI values.The sample sizes in the included studies ranged from 8 to 34 subjects.Among the included studies,there were a total of 412 subjects for this systematic review and meta-analysis.
The amount of exercise performed during the resistance training sessions ranged from 1 to 8 exercises.The intensity of the resistance exercises performed ranged from bodyweight to 100% 1RM.Among these studies,13 study groups performed at low intensity (≤65% 1RM), 25 performed at moderate intensity (>65%-85% 1RM), and 3 performed at high intensity (>85%) (Table 1).With regards to measuring HRV parameters, most of the studies used Polar HR monitors and ECG monitors,with participants in a supine or seated position for 5-15 min.Additionally,most of the studies identified and corrected for or excluded the abnormalities (ectopic/artifacts)of beat-to-beat interval data before analyzing the HRV parameters.HRV measurement and data analyzing methods used in the included studies are presented in Supplementary Table 1.
3.3.Heterogeneity and risk of bias assessment
Except for SDNN (I2=47%, p=0.06), heterogeneity was present for changes in RMSSD (I2=71%, p <0.001), LFnu(I2=83%, p <0.001), HFnu (I2=85%, p <0.001), and LF/HF ratio (I2=40%, p=0.03) parameters among the pre-post intervention studies.Regarding control group interventions,heterogeneity was detected in LFnu (I2=86%, p <0.001),HFnu (I2=80%, p <0.001), and LF/HF ratio (I2=78%, p <0.001),but not in RMSSD(I2=26%,p=0.24).
The quality of the studies,according to the National Heart,Lung, and Blood Institute Study Quality Assessment Tools,48was high for the pre-post interventions (8.18 ± 0.53, out of a possible 12 points) and experimental-control interventions(9.56 ± 0.53, out of a possible 14 points) (see Supplementary Table 2,which illustrates the results of study quality).A funnel plot asymmetry test was used to determine publication bias.Visual interpretation of the funnel plot asymmetry tests(SMD values between pre-post tests and control-experimental tests)showed that SDNN, RMSSD, LFnu, HFnu and LF/HF ratio variables were asymmetrical,suggesting the presence of publication bias) (see Supplementary Figs.1-9, which illustrate the results of the funnel plot asymmetry tests).

Table 1(Continued)
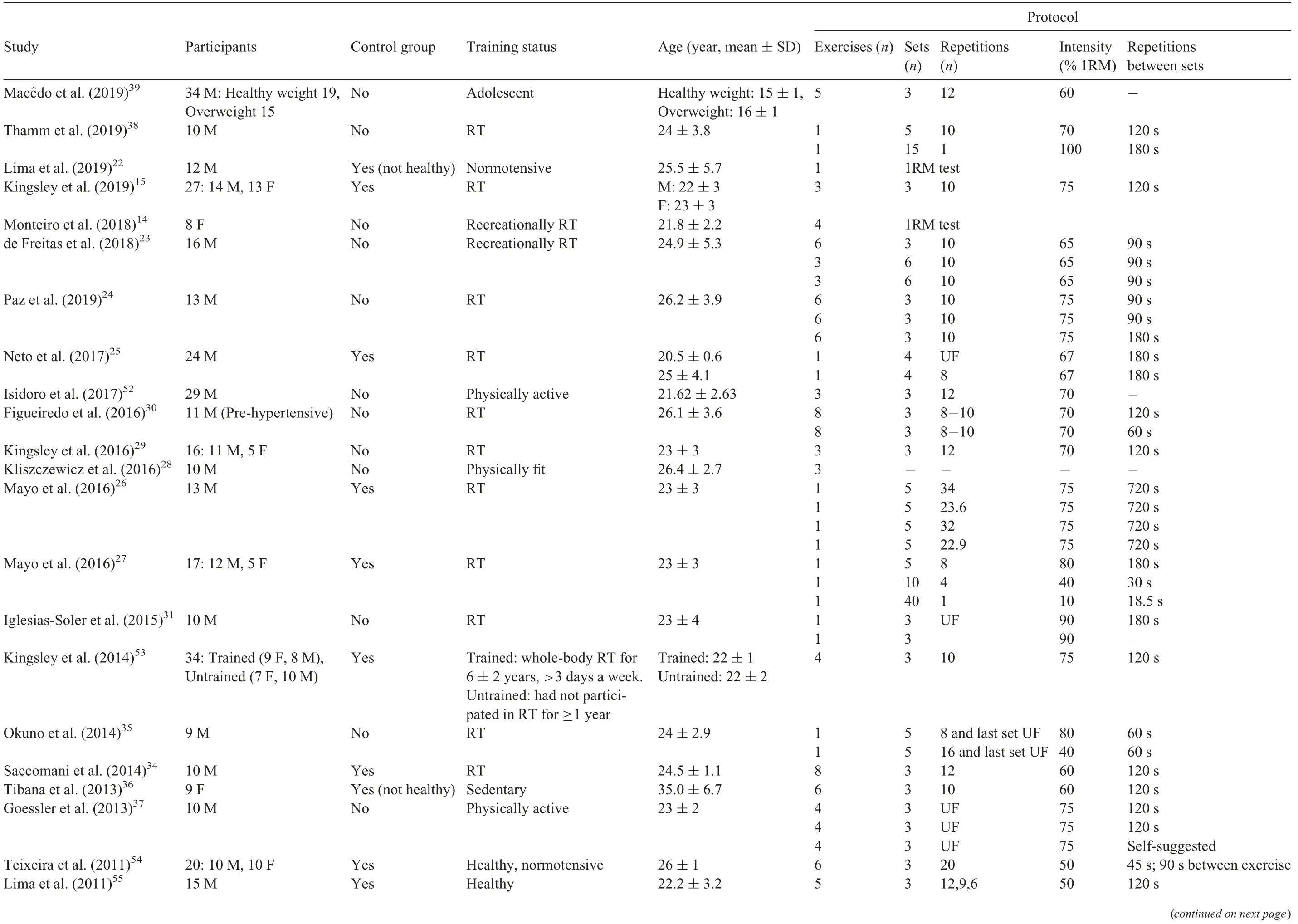
Table 1Characteristics of the ARE sessions for each study.
3.4.Main effects analysis
3.4.1.RMSSD
There were 18 effect size calculations from 15 studies(mean age=23.5 years;199 males,42 females)that showed a decrease in RMSSD(p <0.001;SMD=-1.01;95%CI:-1.29 to-0.74)of ~30 min(8-30 min)after the ARE session compared to pretest values.There were 6 effect size calculations from 4 studies(mean age=22.3 years;64 males,58 females)that demonstrated a decrease in RMSSD (p < 0.001; SMD=-0.75;95%CI: -1.01 to -0.49) post ~30 min (8-30 min) for ARE session compared to control groups(Fig.2).
3.4.2.HFnu
There was a decrease in HFnu (p <0.001; SMD=-1.08;95%CI:-1.43 to-0.73)in 23 effect size calculations from 20 studies(mean age=24.6 years;251 males,52 females)following ARE compared to baseline.When compared to a control group, the ARE group also decreased HFnu (p <0.001;SMD=-1.06;95%CI:-1.52 to-0.60)~30 min(8-30 min)after the ARE session (Fig.3) in 8 effect size calculations from 6 studies(mean age=23.2 years;74 males,35 females).
3.4.3.LFnu
A total of 20 studies(mean age=24.6 years;250 males;57 females), with 22 effect size calculations, showed an increase in LFnu(p <0.001;SMD=0.78;95%CI: 0.46-1.11)after an ARE session compared to pre-intervention.Similarly,6 studies(mean age=23.2 years; 73 males, 40 females), with 7 effectsize calculations, showed an increase in LFnu (p <0.001;SMD=1.00; 95%CI: 0.43-1.56) in the ARE group compared to the control group(Fig.4).
3.4.4.LF/HF ratio
In the 21 effect size calculations in 19 studies (mean age=25.4 years;235 males,66 females),there was an increase in LF/HF ratio (p <0.001; SMD=0.82; 95%CI: 0.64-0.99)~30 min(8-30 min)after ARE compared to baseline.A total of 10 effect size calculations from 8 studies (mean age=22.9 years; 93 males, 53 females) also showed an increase in LF/HF ratio (p <0.001; SMD=1.02; 95%CI: 0.62-1.43) in the ARE group compared to the control group(Fig.5).
3.4.5.SDNN
A total of 7 studies (mean age=22.4 years; 103 males, 33 females),with 9 effect size calculations,showed a decrease in SDNN (p <0.001; SMD=-0.58; 95%CI: -0.85 to -0.30)after an ARE session compared to pre-intervention (Fig.6).However, the main effect analysis was not conducted for the ARE group compared with the control group due to the limited number of studies(only 1 study).
3.5.Subgroup analysis
3.5.1.RMSSD
For the subject characteristics, there was no difference in effect between subgroups based on gender (p=0.12), BMI(p=0.44), or training status (p=0.48).With respect to resistance training variables, the number of sets (p=0.05) and training volume (p=0.01) showed a difference in effect between subgroups.Moreover, the SMD data showed that 3 sets and higher training volume had the greatest effect on RMSSD, whereas <3 sets and lower training volume had the least effect when comparing subgroups following resistance exercises.However, no other variables (exercises (p=0.07),intensity (p=0.41), repetitions (p=0.39), and rest (p=0.31))indicated a difference in effect between subgroups(Table 2).
3.5.2.HFnu
For the subject characteristics, there was no difference in effect between subgroups for gender (p=0.75), BMI(p=0.74), or training status (p=0.15).Regarding resistance training variables, intensity (p=0.01), rest between sets(p=0.05), and training volume (p=0.003) showed a difference in effect between subgroups.Furthermore, SMD data revealed that low intensity, <2 min of rest and higher training volume had the greatest effect on HFnu, whereas high intensity, 2 min of rest and lower training volume had the least effect compared to subgroups following ARE.However, there was no difference in effect between subgroups for all the other variables (repetitions (p=0.10),sets (p=0.93), and exercises (p=0.37)) (Table 2).
3.5.3.LFnu
Regarding the subject characteristics, there was no difference in effect between subgroups for gender (p=0.63),BMI (p=0.37), or training status (p=0.45).Except for training volume (p=0.02), all the other resistance training variables (intensity (p=0.15), sets (p=0.90), exercises(p=0.17), repetitions (p=0.46), and rest (p=0.41)) show no difference in effect between subgroups following resistance exercises.SMD data for training volume showed that a higher training volume had a greater effect and that a lower training volume had a lesser effect on LFnu compared to other subgroups following resistance exercises(Table 2).
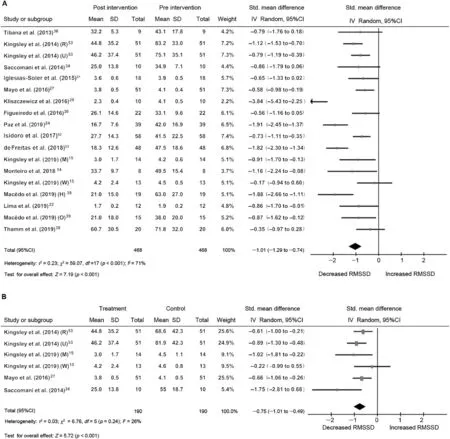
Fig.2.Forest plots for the acute effects of RT on RMSSD.(A)Acute effects of RT sessions on RMSSD pre-vs.post-intervention.(B)Acute effects of RT sessions on RMSSD control group vs.treatment group.Squares represent the SMD for each trial.Diamonds represent the pooled SMD across trials.95%CI = 95% confidence interval;df=degrees of freedom;H=healthy weight;IV=inverse variance;M=men;O=overweight;R=resistance trained;RMSSD=root mean square of the successive differences;RT=resistance training;SMD=standardized mean difference;Std.=standard;U=untrained;W=women.
3.5.4.LF/HF ratio
Concerning the subject characteristics (gender (p=0.65),BMI (p=0.77), and training status (p=0.55)) and resistance training variables (intensity (p=0.24), repetitions (p=0.82),sets(p=0.56),exercises(p=0.51),rest(p=0.99),and volume(p=0.62)), there was no difference in effect between subgroups(Table 2).
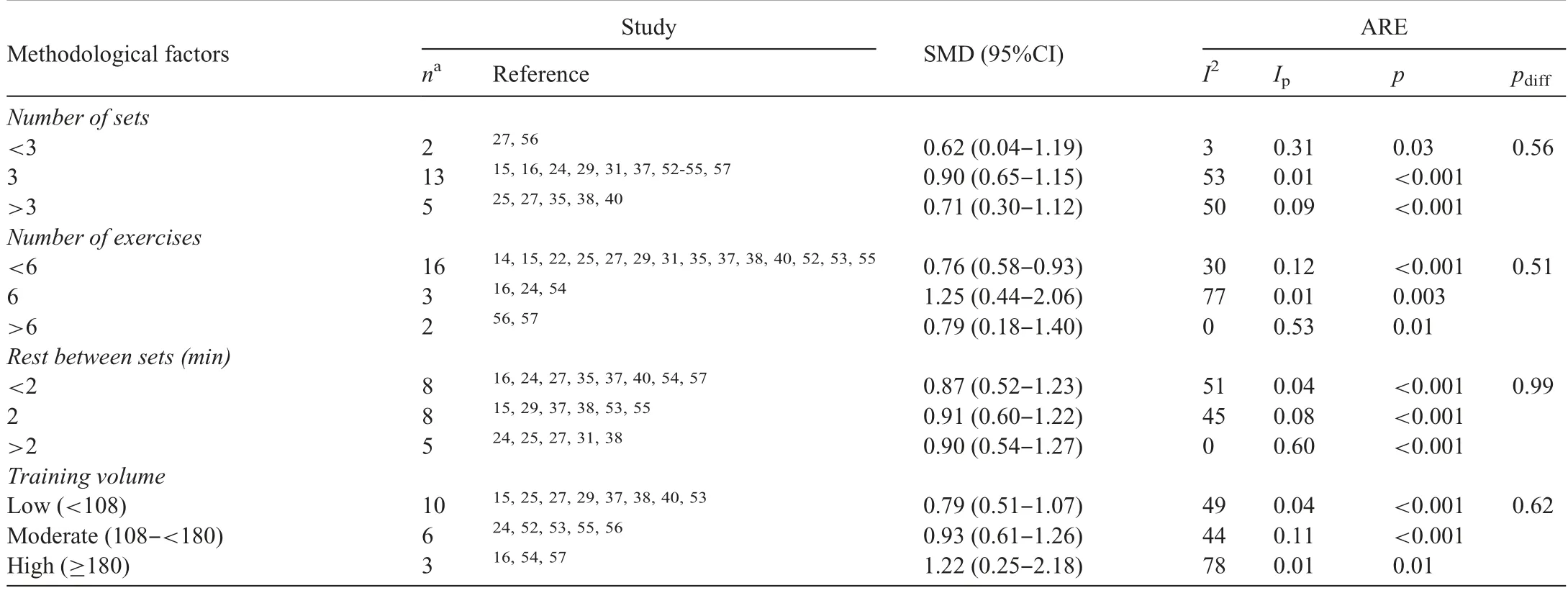
Table 2(Continued)
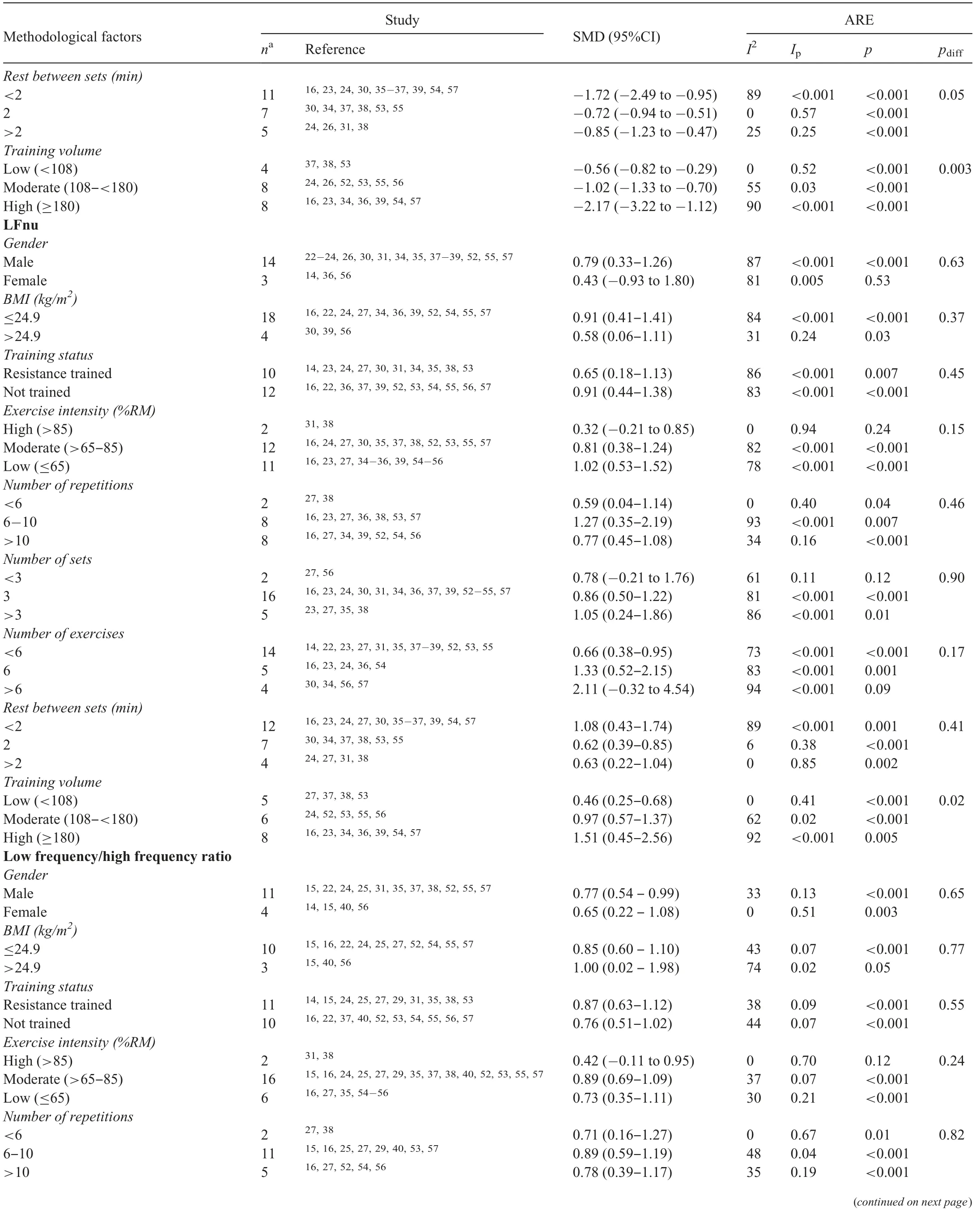
Table 2(Continued)
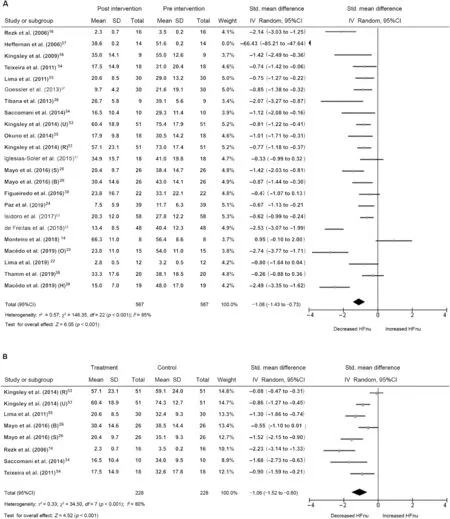
Fig.3.Forest plots for the acute effects of RT on HFnu.(A)Acute effects of RT sessions on HFnu pre-vs.post-intervention.(B)Acute effects of RT sessions on HFnu control group vs.treatment group.Squares represent the SMD for each trial.Diamonds represent the pooled SMD across trials.95%CI = 95% confidence interval;B=bench press;df=degrees of freedom;H=healthy weight;IV=inverse variance;M=men;O=overweight;R=resistance trained;S=parallel squat;HFnu=normalized units high frequency;RT=resistance training;SMD=standardized mean difference;Std.=standard;U=untrained;W=women.

Fig.4.Forest plots for the acute effects of RT on LFnu.(A)Acute effects of RT sessions on LFnu pre-vs.post-intervention.(B)Acute effects of RT sessions on LFnu control group vs.treatment group.Squares represent the SMD for each trial.Diamonds represent the pooled SMD across trials.95%CI = 95% confidence interval;df=degrees of freedom;H=healthy weight;IV=inverse variance;M=men;O=overweight;R=resistance trained;LFnu=normalized units low frequency;RT=resistance training;SMD=standardized mean difference;Std.=standard;U=untrained;W=women.
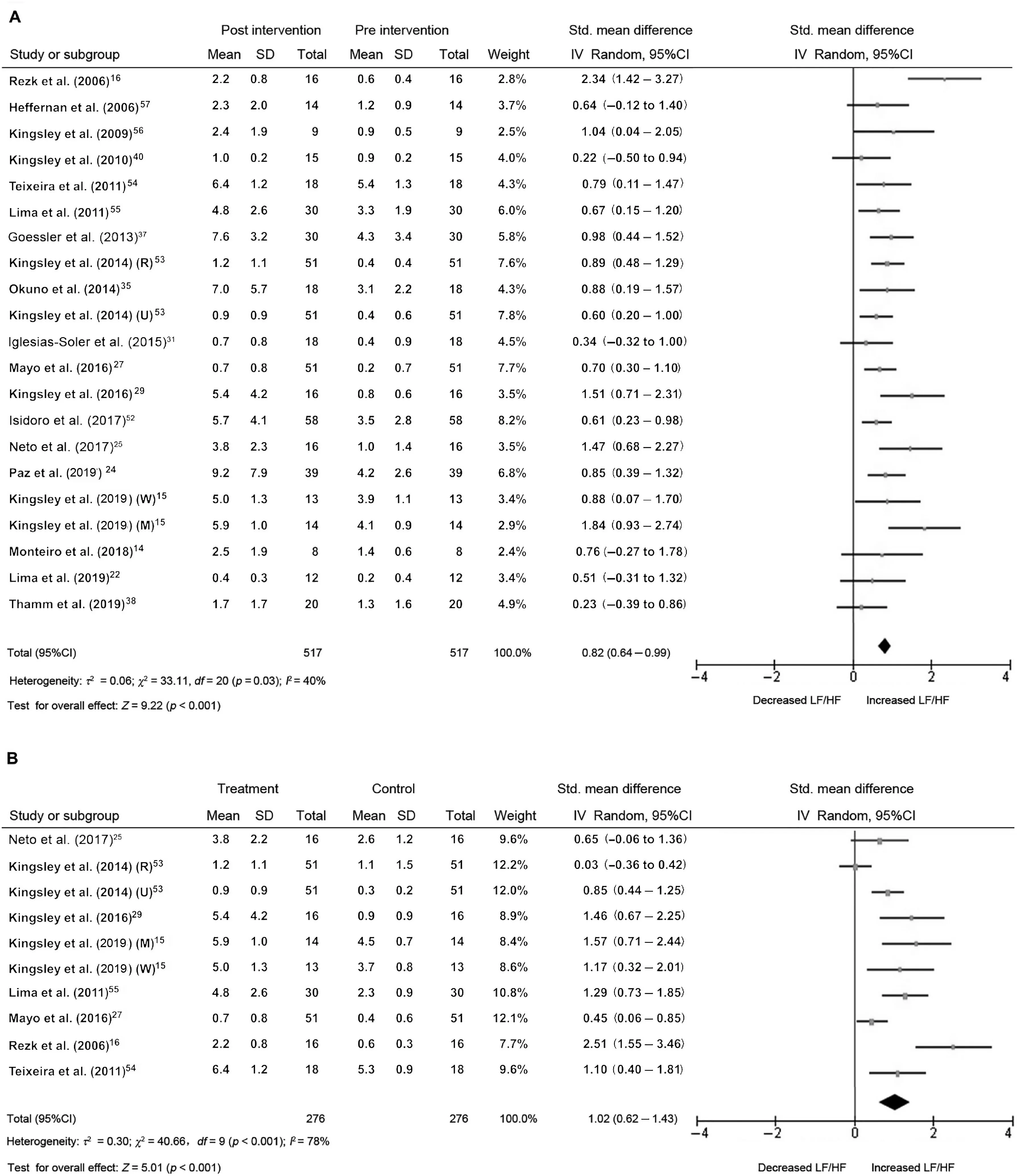
Fig.5.Forest plots for the acute effects of RT on LF/HF ratio.(A) Acute effects of RT sessions on LF/HF ratio pre- vs.post-intervention.(B) Acute effects of RT sessions on LF/HF ratio control group vs.treatment group.Squares represent the SMD for each trial.Diamonds represent the pooled across trials.95%CI=95% confidence interval; df = degrees of freedom; H = healthy weight; IV = inverse variance; M = men; R = resistance trained; LF/HF=low frequency/high frequency;RT=resistance training;SMD=standardized mean difference;Std.=standard;U=untrained;W=women.
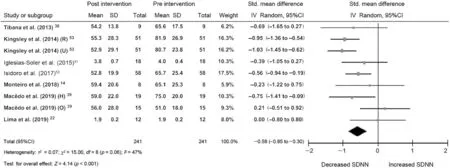
Fig.6.Forest plots for the acute effects of RT on SDNN.Acute effects of RT sessions on SDNN pre-vs.post-intervention.Squares represent the SMD for each trial.Diamonds represent the pooled SMD across trials.95%CI=95%confidence interval;df=degrees of freedom;H=healthy weight;IV=inverse variance;M=men;R=resistance trained;RT=resistance training;SDNN=standard deviation of the NN interval;SMD=standardized mean difference;Std.=standard;U=untrained;W=women.
4.Discussion
The main aim of this meta-analysis was to provide essential information regarding the recovery status of cardiac autonomic activity following an ARE session,particularly identifying the moderating factors that affect HRV parameters.The principal findings demonstrated a significant decrease in cardiac parasympathetic modulation and an increase in cardiac sympathetic modulation following an ARE session (~30 min).Moreover,overall autonomic modulation showed a significant decrease after an ARE session.The reduction of RMSSD and HFnu parameters indicates a withdrawal of cardiac parasympathetic modulation,42,44,45and the increase in the LFnu parameter suggests the domination of cardiac sympathetic modulation44,45after an ARE session.Furthermore, an increase in the LF/HF ratio suggests a shift in sympathovagal balance towards sympathetic domination,42,44and a reduction in the SDNN value indicates a decrease in overall autonomic modulation.45Along these lines,our findings are in accordance with the review article conducted by Kingsley and Figueroa,21which examined the ARE on HRV parameters.21It is important to acknowledge that the interpretation of the LF parameter and the LF/HF ratio has been controversial.Some authors consider the LF parameter to be a cardiac sympathetic modulation marker, while others believe that it reflects both sympathetic and parasympathetic modulation.With regards to the LF/HF ratio, some authors interpret this variable as a cardiac sympathetic modulation marker, while others suggest that it is a reflection of sympathovagal balance.45Overall,our meta-analysis suggests that the early recovery phase is still predominated by cardiac sympathetic activity.
A physiological explanation for this phenomenon during the recovery phase of resistance training may be that there is a decrease in plasma volume as a result of an acute cardiovascular imbalance.16This imbalance may be a result of the blood entering into the interstitial cellular space,55which changes the sensitivity of the arterial baroreflex in order to maintain the blood pressure changes caused by a decrease in stroke volume(a consequence of an increase in heart rate after resistance exercise).16This creates a greater activation of metaboreceptors and mechanoreceptors, thus providing adequate blood flow in order to meet the metabolic demands of the active muscles.16,32,33Also, there may be an increase in peripheral vascular resistance in arterial vessels supplying visceral organs, where redistributed blood flows to the active muscles during the recovery process.16,32,33Moreover,Buchheit et al.58have suggested that the levels of fast-twitch muscle fiber recruitment, catecholamine release and accumulation of lactate,hydrogen ions and inorganic phosphate may play a role in decreasing cardiac parasympathetic modulation, thereby increasing cardiac sympathetic modulation.Thus, evaluating HRV variables can be useful in determining cardiac autonomic stress, which may be beneficial for fitness trainers or coaches to use as a monitoring tool for measuring the effect of the training load following an ARE session on the cardiac autonomic system.
Our subgroup analyses revealed that training volume is an important moderating factor for RMSSD, LFnu, and HFnu parameters.The number of sets is a moderating factor for RMSSD parameter, while exercise intensity and rest between sets are moderating factors for HFnu parameter.These aforementioned moderating factors affect the recovery process of cardiac autonomic modulation following a resistance training session.Therefore, fitness trainers and coaches could monitor and adjust the training load by measuring the changes in cardiac autonomic modulation using HRV variables such asRMSSD (training volume, number of sets per exercise) and HFnu(number of exercises,reset between sets).The following provides a more detailed discussion of each of the subgroup analyses.
4.1.Subjects characteristics
Subgroup analyses did not show a significant difference between males and females (gender) for RMSSD, HFnu, LFnu,and LF/HF ratio parameters.These findings are in line with the findings of Kingsley et al.,15who concluded that changes in HRV parameters in response to an ARE were not influenced by gender differences.The BMI subgroup analyses also demonstrated no significant effect on RMSSD, HFnu, LFnu, and LF/HF ratio parameters.Similarly, Mac^edo et al.39reported that changes in HRV parameters in response to ARE were not affected by body weight.However, Beske et al.59reported that lower cardiovagal baroreflex gain was marginally related to higher body fat percentage.When cardiovagal baroreflex sensitivity is lower, there is a weaker response to the changes in systolic blood pressure, and this does not effectively change the heart rate.60Therefore, higher body fat mass may have a minimal effect on cardiac sympathetic modulation and thus may only trigger a minimal change in heart rate.Likewise,the analyses of the training status subgroup demonstrated no significant effect on RMSSD, HFnu, LFnu, and LF/HF ratio variables.These findings are again in line with the findings of Kingsley et al.,53who concluded that changes in HRV parameters in response to the ARE were not influenced by training status.Thus, our study showed that gender, BMI, and training status do not play a role in cardiac autonomic modulation changes following an ARE sessions.Therefore, trainers and coaches may not need to specialize a resistance training session based on an individual’s gender, BMI level or training status.However, we believe that further investigations on the relationship between BMI and HRV parameters related to an ARE session are needed.
4.2.Training characteristics
4.2.1.Number of repetitions,sets,and exercises per workout
There were no significant differences among the number of repetitions subgroups for RMSSD, LFnu, HFnu, and LF/HF ratio parameters.Interestingly, a significant difference was demonstrated between subgroups for the RMSSD parameter and the number of sets and number of exercises,but this significant difference was not demonstrated for the LFnu and HFnu parameters.Additionally, SMD results showed that the RMSSD parameter was affected greatly by an ARE session that included exactly 3 sets per exercise but was not affected greatly when there were <3 sets per exercise.Our findings agree with the findings of Figueiredo et al.,33who reported a reduced cardiac sympathetic modulation response with a lower number of sets of resistance training compared to a higher number sets.Therefore, performing ≥3 sets per exercise generates a higher sympathetic stress and may delay the recovery process compared to performing <3 sets per exercise.
SMD data also demonstrated that the RMSSD parameter may be affected by the number of exercises, with a higher effect shown for exactly 6 exercises,although this did not reach statistical significance (pdiff=0.07).Thus, performing 3 sets per exercise, and possibly 6 exercises per session, generates a greater withdrawal of cardiac parasympathetic modulation after an ARE session.It remains to be determined whether the number of exercises truly has an effect on RMSSD.
4.2.2.Rest between sets
The rest period only had an effect on the HFnu parameter.SMD data showed that HFnu was greatly affected by an AREsession that included <2 min of rest between sets but was less affected when there was exactly 2 min or >2 min of rest between sets.In line with our findings, Goessler et al.37suggested that at least 2 min of rest between sets reduces the postexercise cardiac sympathetic modulation following ARE.Therefore,having <2 min of resting time between sets generates greater withdrawal of cardiac parasympathetic modulation, and 2 min or more minutes of rest between sets creates lesser withdrawal of cardiac parasympathetic modulation,independent of the other variables of resistance training.These results indicate that having <2 min of rest between sets delays the recovery process following an ARE session compared to≥2 min of rest between sets.
4.2.3.Exercise intensity
Based on our subgroup analysis,the exercise intensity(low,moderate,or high)of an ARE session is not a moderating factor for RMSSD, LFnu, or LF/HF ratio.Figueiredo et al.32showed no differences between the level of intensity of a training session (60% 1RM, 70% 1RM, and 80% of 1RM) and RMSSD.Additionally, Rezk et al.16demonstrated no difference in LFnu or HFnu when comparing 40% 1RM and 80%1RM training sessions.This is an interesting finding given that, although ARE has an effect on cardiac sympathetic and cardiac parasympathetic modulation, the different intensity levels did not make a significant contribution to cardiac autonomic modulation; thus, they worked independently of other covariables related to resistance training.However, in our study, only the HFnu parameter showed a significant difference between exercise intensity subgroups.Surprisingly, our SMD results showed that low exercise intensity had the greatest effect and high exercise intensity had the least effect on the HFnu parameter.One possible explanation for the difference shown between the HFnu and RMSSD parameters (both of which represent cardiac parasympathetic modulation) is that the included studies in each subgroup was different but the tendency of the findings was the same: a lower intensity had a higher effect.This may be a consequence of having a longer training duration of lower intensity.Another explanation may be that respiration control influences HFnu during HRV measurements.21,42Also, in our review, included studies in which lower exercise intensities were performed used a higher training volume and included studies in which higher exercise intensities were performed used a lower training volume.All these factors should be taken into consideration when interpreting the outcomes of our meta-analysis.Furthermore, our results indicated that there is a direct relationship between higher training volume and greater cardiac sympathetic activation and withdrawal of cardiac parasympathetic modulation.
4.2.4.Training volume
There was a significant difference between subgroups based on training volumes in the RMSSD,LFnu,and HFnu parameters.Our finding is consistent with the findings of Figueiredo et al.,33who suggested that higher training volume increases the recruitment of additional motor units,thus minimizing the likelihood of muscular failure during the concentric phase of lifting(concentric failure)and triggering a progressive activation of the cardiac sympathetic modulation.61Moreover, our SMD results revealed that higher training volume had a greater effect and lower training volume had the lesser effect on RMSSD,HFnu,and LFnu parameters.
Our results indicated that higher training volume produces a greater activation of cardiac sympathetic modulation and withdrawal of cardiac parasympathetic modulation.In other words,when the human body experiences a higher level of resistance training volume,the magnitude of activation of cardiac sympathetic modulation and withdrawal of cardiac parasympathetic modulation is higher than it is with lower training volume.On the other hand, previous studies have reported that a low volume of high-intensity resistance training greatly improves strength, muscle size,62,63force production and rate of force development64compared to a high volume of moderate- or low-intensity resistance training.Thus,our meta-analysis suggests that a low training volume of high-intensity ARE would enable athletes to have the optimal training load or stimulus without creating a large change in cardiac autonomic modulation, thus allowing for an early recovery without ultimately sacrificing training adaptation and performance.
We acknowledge that there are a few limitations in our meta-analysis.First, only a limited number of studies were included due to the lack of research on ARE interventions that had HRV parameters as an outcome variable.In fact, only 26 studies(with a total of 412 participants)met the inclusion criteria for our systematic review and meta-analysis,and of these studies, only 21 reported on the LFnu and HFnu parameters,only 19 included results for the LF/HF ratio parameter, only 15 reported on the RMSSD parameter and only 7 reported SDNN parameter results.Second,some of the included studies had a small sample size(range:8-34),which may have negatively impacted our findings.Third, there was a presence of heterogeneity in several moderating factors,and this should be taken into consideration when interpreting the outcomes of our meta-analysis.Fourth, different methodological procedures,equipment and software were used to measure HRV parameters in the different studies.
5.Conclusion
This systematic review and meta-analysis demonstrated that there is a decrease of overall autonomic modulation, withdrawal of cardiac parasympathetic modulation and activation of cardiac sympathetic modulation following an ARE session(after ~30 min) in healthy individuals.Importantly, there is a greater effect of training volume on the activation of cardiac sympathetic modulation and withdrawal of cardiac parasympathetic modulation ~30 min after resistance exercises in healthy individuals.Furthermore, the number of sets, the intensity of exercise, and amount of rest between sets play an important role in the ARE on HRV parameters.However, gender, BMI and training status do not significantly influence the changes in HRV parameters as a response to ARE.With regards to the practical application of our findings, we would recommend that fitness trainers and coaches consider HRV evaluations asaids to programming their athletes’ training sessions, depending on the stress goals they want to apply.Based on our metaanalysis,the variables related to resistance training modify the stress applied to the cardiac autonomic system.Thus,ARE sessions that comprise ≥3 sets,<2 min of rest between sets,and 6 exercises at low intensity would lead to greater stress on the cardiac sympathetic system.This information can help coaches and trainers optimize training sessions and improve the recovery process.
Acknowledgment
We would like to thank all authors of included studies who responded to our requests for additional information for our meta-analysis.
Authors’contributions
All authors participated in the study design and provided critical input regarding the manuscript draft; SUMA performed the methodology,analyzed and interpreted the findings and drafted the manuscript;JARA contributed to article selection, helped with the risk-of-bias assessment, confirmed the extracted data, and helped with the interpretation of the findings.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary materials associated with this article can be found in the online version at doi:10.1016/j.jshs.2020.11.008.
杂志排行

Journal of Sport and Health Science的其它文章
- The secrets to running economy
- Metabolic and performance responses of male runners wearing 3 types of footwear:Nike Vaporfly 4%,Saucony Endorphin racing flats,and their own shoes
- Longitudinal bending stiffness does not affect running economy in Nike Vaporfly Shoes
- Can changes in midsole bending stiffness of shoes affect the onset of joint work redistribution during a prolonged run?
- Metabolic cost of level,uphill,and downhill running in highly cushioned shoes with carbon-fiber plates
- Systematic reduction of leg muscle activity throughout a standard assessment of running footwear