How to examine anastomotic integrity intraoperatively in totally laparoscopic radical gastrectomy? Methylene blue testing prevents technical defect-related anastomotic leaks
2022-06-08ChunDengYangLiuZhenYuZhangHengDuoQiZhiGuoXuZhaoXiaoJunLi
Chun Deng, Yang Liu, Zhen-Yu Zhang, Heng-Duo Qi, Zhi Guo, Xu Zhao, Xiao-Jun Li
Chun Deng, Yang Liu, Zhen-Yu Zhang, Heng-Duo Qi, Zhi Guo, Xu Zhao, Xiao-Jun Li, Department of General Surgery, Shaanxi Provincial People's Hospital, Xi'an 710068, Shaanxi Province,China
Abstract BACKGROUND Intraoperative methylene blue testing (IMBT), air leak testing, or endoscopy is used to assess the anastomotic integrity of esophagojejunostomy during open total gastrectomy for gastric cancer. Totally laparoscopic radical gastrectomy has been widely used to treat gastric cancer in the last few decades. However, reports on testing anastomotic integrity in totally laparoscopic radical gastrectomy are limited.AIM To explore the effects of IMBT on the incidence of postoperative anastomotic leaks(PALs) and identify the risk factors for PALs in totally laparoscopic radical gastrectomy.METHODS From January 2017 to December 2019, patients who underwent totally laparoscopic radical gastrectomy at the Shaanxi Provincial People's Hospital were retrospectively analyzed. According to whether or not they experienced an IMBT,the patients were divided into an IMBT group and a control group. If the IMBT was positive, an intraoperative suture was required to reinforce the anastomosis.The difference in the incidence of PALs was compared, and the risk factors were investigated.RESULTS This study consisted of 513 patients, 211 in the IMBT group and 302 in the control group. Positive IMBT was shown in seven patients (3.3%) in the IMBT group, and no PAL occurred in these patients after suture reinforcement. Multivariate analysis showed that risk factors for predicting positive IMBT were body mass index (BMI) > 25 kg/m2 (hazard ratio [HR] = 8.357, P = 0.009), operation time > 4 h (HR = 55.881, P= 0.002), and insufficient surgical experience (HR = 15.286, P = 0.010). Moreover, 15 patients (2.9%)developed PALs in 513 patients, and the rates of PALs were significantly lower in the IMBT group than in the control group [2 of 211 patients (0.9%) vs 13 of 302 patients (4.3%), P = 0.0026]. Further analysis demonstrated that preoperative complications (HR = 13.128, P = 0.017), totally laparoscopic total gastrectomy (HR = 9.075, P = 0.043), and neoadjuvant chemotherapy (HR = 7.150, P =0.008) were independent risk factors for PALs.CONCLUSION IMBT is an effective method to evaluate the integrity of anastomosis during totally laparoscopic radical gastrectomy, thus preventing technical defect-related anastomotic leaks. Preoperative complications, totally laparoscopic total gastrectomy, and neoadjuvant chemotherapy are independent risk factors for PALs.
Key Words: Anastomotic leak; Gastric neoplasms; Totally laparoscopic radical gastrectomy; Methylene blue;Risk factors
lNTRODUCTlON
Gastric cancer is one of the most common cancers worldwide, ranking fifth in incidence and third in mortality[1]. Totally laparoscopic radical gastrectomy has been widely used to treat gastric cancer[2-4].Postoperative anastomotic leak (PAL) is a severe complication, and occurs in 1.7%-5.7% of patients with gastric cancer[5-7]. These complications could prolong hospital stay, increase medical expenses, cause poor quality of life, and subsequently worsen the long-term survival of patients[8-10].
It is well known that the defects of intraoperative anastomotic techniques are closely related to PALs[11-13]. Therefore, some PALs might be avoided if insufficiently integral anastomoses were immediately reinforced. Intraoperative methylene blue testing (IMBT), intraoperative air leak test, or intraoperative endoscopy has been used to assess the anastomotic integrity of esophagojejunostomy during open total gastrectomy for gastric cancer[6,14-15]. However, to the best of our knowledge, no study has assessed the integrity of anastomosis during totally laparoscopic radical gastrectomy. Compared with open surgery, totally laparoscopic radical gastrectomy has the disadvantages of two-dimensional images,poor hand-eye coordination, limited operating space, fulcrum effect, and lack of haptic feedback[16-17].Furthermore, according to the ERAS guidelines, abdominal drains should not routinely be placed after gastrectomy, which requires high-quality anastomosis[18-19]. Thus, a reliable anastomosis leak test is vital during totally laparoscopic radical gastrectomy.
In this study, we used IMBT to check the anastomotic integrity of esophagojejunostomy or gastrojejunostomy during totally laparoscopic radical gastrectomy. This is the first study to assess the anastomotic integrity during totally laparoscopic radical gastrectomy. We aimed to explore the effects of IMBT on the incidence and risk factors for PALs.
MATERlALS AND METHODS
Patients
We performed a retrospective review of patients who underwent totally laparoscopic radical gastrectomy from January 2017 to December 2019. In our department, some surgeons think that IMBT is useful, while others are skeptical regarding its effects. Thus, two groups were formed: An IMBT group and a control group. Staging of the tumor was performed following the eighth edition of the AJCC Guidelines for gastric cancer[20]. This study was approved by the Ethics Committee of Shaanxi Provincial People's Hospital.
The inclusion criteria were: (1) Patients who underwent totally laparoscopic radical gastrectomy for gastric cancer and adenocarcinoma of the gastroesophageal junction from January 2017 to December 2019; (2) Gastric cancer or adenocarcinoma of the gastroesophageal junction diagnosedviaendoscopy and pathological identification; and (3) Patients whose surgical and demographic data were complete and reliable. The exclusion criteria were: (1) Patients who underwent totally laparoscopic distal gastrectomy that used Billroth-I anastomosis; (2) Those who were converted to open surgery; (3) Those who were found to have distant metastases intraoperatively; (4) Those who did not undergo radical resection; and (5) Those who gave up treatment or were transferred to another hospital.
Surgical methods and postoperative management
All surgeries were performed laparoscopically. Totally laparoscopic total gastrectomy was reconstructedviaan overlap anastomosis[21], and totally laparoscopic distal gastrectomy was reconstructedviaa Billroth-II anastomosis[22]. Lymph node dissection was performed according to the Japanese Gastric Cancer Treatment Guidelines 2014 (ver. 4)[23]. This study used a 45-mm linear stapler(Johnson Company, United States) for the overlap anastomosis and a 60-mm linear stapler (Johnson Company, United States) for the Billroth-II anastomosis. In our department, we preferred the Billroth II anastomosis and Roux-en-Y esophagojejunostomy rather than the Billroth I anastomosis. A Billroth I anastomosis needs to preserve a large residual stomach, leading to insufficient tumor margins and significant anastomotic tension when the tumor location is relatively high and the diameter is large. In China, most gastric cancer cases are found in advanced stages, and the diameter of the tumor is often large compared to Japan and Korea[24-26]. In addition, Billroth I anastomosis has a greater risk of remnant gastritis and reflux esophagitis[27-28].
Postoperative management was conducted according to the Japanese Gastric Cancer Treatment Guidelines (ver.4)[23]: The nasogastric tube was removed on postoperative day 1, and the abdominal drainage tube removed on postoperative day 5 without symptoms or inflammatory reactions.Abdominal CT, gastrointestinal tract angiography, or endoscopy was performed when an anastomotic leak was suspected.
Methylene blue testing technique
For the patients that underwent totally laparoscopic total gastrectomy, we performed IMBT as follows(Figure 1A): After the digestive tract reconstruction (Figure 2A and A’), the nasogastric tube (18F) was delivered 5 cm from the distal end of the anastomotic stoma, gauze was wrapped around the anastomosis, and then the jejunum was clamped using an intestinal clamp 5 cm distal to the anastomosis. Next, normal saline was injected through the nasogastric tube to rinse and observe whether continuous bright red liquid flowed out of the nasogastric tube when pumping back. If the liquid was detected, we looked for and stopped the bleeding and then flushed repeatedly until the clear liquid was pumped back out. Next, we dissolved 2 mL (20 mg) of methylene blue into 50 mL of normal saline and injected it through the nasogastric tube in order to make the methylene blue liquid disperse evenly around the anastomosis (Figure 2B and B’). Finally, we observed whether the gauze around the anastomosis was stained blue; if there was blue staining (Figure 3), we identified the leak according to the blue-stained site, sutured it, and then changed the gauze and repeated the process.
For the patients who underwent totally laparoscopic distal gastrectomy, IMBT was performed as follows (Figure 1B): The nasogastric tube (18F) was indwelled 5 cm from the distal end of the anastomotic stoma after the digestive tract reconstruction (Figure 2C and C’). Next, we wrapped the anastomosis with gauze, and closed it with clamps 5 cm distal to the anastomosis. Then, the anastomosis was flushed with normal saline through the nasogastric tube; the needle was pumped back to observe whether there was bright red liquid flowing out of the nasogastric tube. If red liquid was present, we looked for and stopped the bleeding. The flushing was repeated until the clear liquid was extracted from the nasogastric tube. Next, 5 mL (50 mg) of methylene blue was dissolved into 500 mL of normal saline and injected through the nasogastric tube in order to evenly distribute the methylene blue liquid around the anastomosis (Figure 2D and D’). Finally, if blue liquid was present, we repeated the above procedures.
Definitions
We defined preoperative complications as one or more of the following: Anemia, malnutrition, diabetes,or pulmonary dysfunction. The World Health Organization's definition of anemia was used to define anemia: Hb concentration of < 12 g/dL in women and < 13 g/dL in men[29]. Malnutrition was defined by the European Society of Clinical Nutrition and Metabolism (ESPEN) criteria[30], which suggested two methods used to diagnose malnutrition: Method one: Body mass index (BMI) < 18.5 kg/m2; method two: Unintentional weight loss combined with a low age-related BMI (< 20 kg/m2in subjects < 70 years or < 22 kg/m2in those ≥ 70 years) or low fat-free mass index (FFMI) (< 17 kg/m2in men and < 15 kg/m2in women). Positive IMBT was defined as the visualization of methylene blue on the gauze surrounding the anastomosis. PAL was defined as meeting one of the following criteria: (1) Gastrointestinal contents or bile-like fluid drained from the abdominal drainage tube; (2) Gastrointestinal radiography showed leakage of the contrast medium from the drainage tube; (3) Methylene blue was extracted from the abdominal drainage tube after the oral administration of methylene blue; (4) Abdominal CT examination showed that the gastrointestinal wall was incomplete, revealing gas and fluid leaks around the anastomosis; and (5) Anastomotic leaks were found under endoscopy after surgery.
Statistical analysis
Analyses were performed with statistic software SPSS for Windows Version 25.0 (SPSS Inc., Chicago,Illinois, United States). Measurement data are expressed as the mean ± SD (normal distribution) or median (non-normal distribution). Count data are expressed as cases (rate). Univariate analysis was performed by the Chi-square test or a Fisher’s exact test when appropriate. Variables withP< 0.05 in the univariate analysis were included in multivariate analysis, which was conducted using the logistic regression model.P< 0.05 was considered statistically significant.
RESULTS
From January 2017 to December 2019, a total of 513 patients that underwent totally laparoscopic radical gastrectomy were analyzed retrospectively (211 patients in the IMBT group and 302 patients in thecontrol group). Complete data of the intraoperative and postoperative findings are shown in Figure 4.The baseline data of the patients in the two groups are consistent, as shown in Table 1.
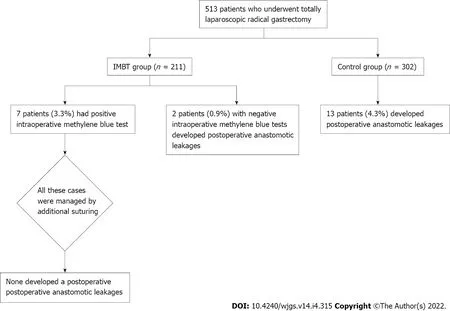
Figure 4 Schematic representation of study protocol and results. IMBT: Intraoperative methylene blue testing.
Risk factors for positive IMBT
Seven patients (3.3%) had positive IMBT in the IMBT group, as detailed in Table 2. These cases were managed by additional suturing, none had a PAL, and the mean postoperative hospital stay was 10.3 ±1.1 d. Univariate analysis showed that surgeons with insufficient surgical experience (< 50 cases of totally laparoscopic radical gastrectomy) were associated with a higher rate of positive IMBT (14.3%vs2.1%,P= 0.021). Other risk factors included operation time > 4 h, neoadjuvant chemotherapy, and a body mass index (BMI) > 25 kg/m2(P= 0.008, 0.033, and 0.021, respectively), as shown in Tables 3 and 4. Multivariate analysis identified BMI > 25 kg/m2, operation time > 4 h, and insufficient surgical experience as independent risk factors for positive IMBT (P= 0.009, 0.002, and 0.010, respectively), as detailed in Table 5.

Table 2 Characteristics of positive intraoperative methylene blue testing

Table 3 Clinicopathological characteristics of the patients according to the results of intraoperative methylene blue testing and postoperative anastomotic leaks
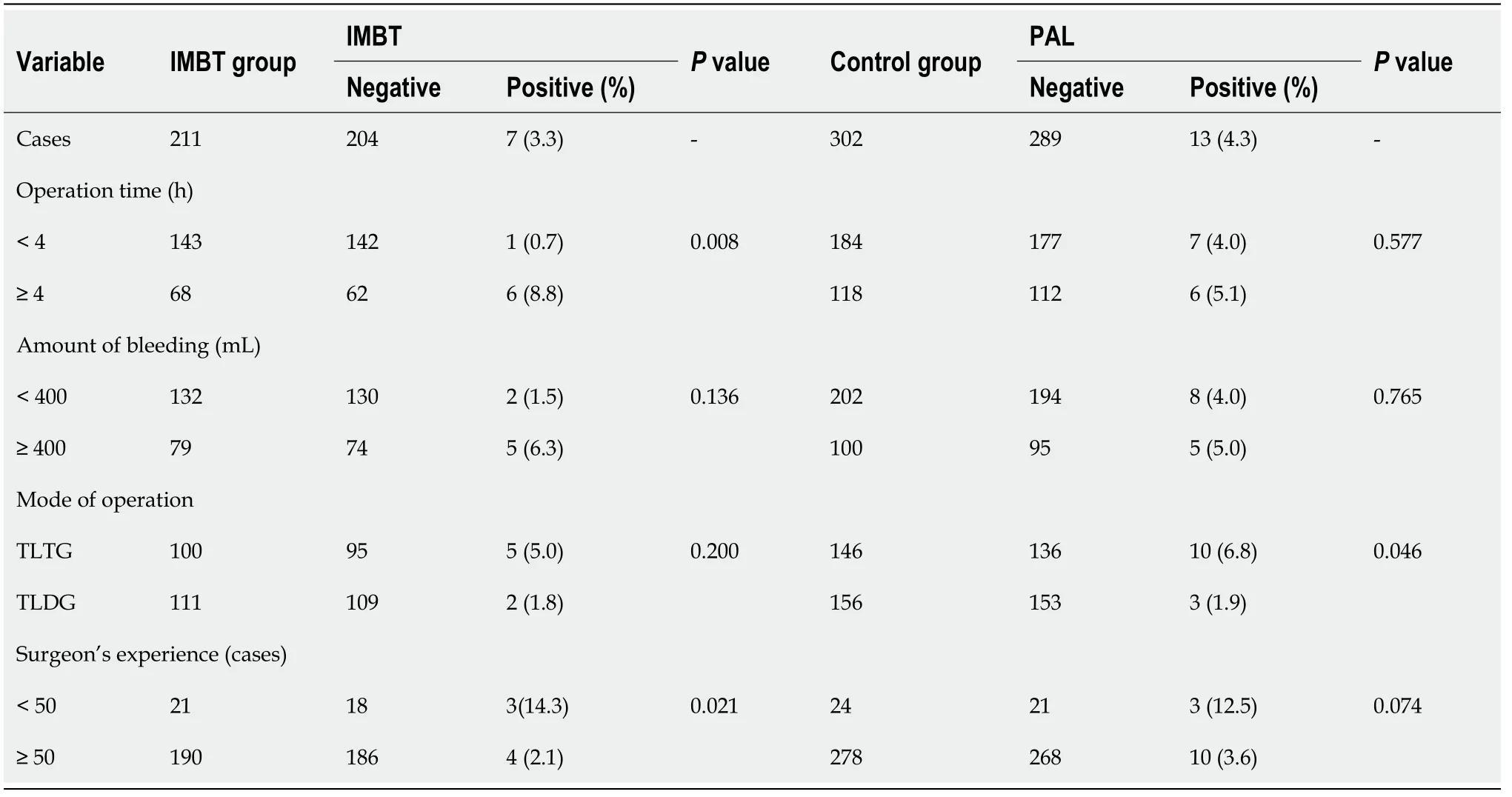
Table 4 Surgical variables according to the results of intraoperative methylene blue testing and postoperative anastomotic leaks
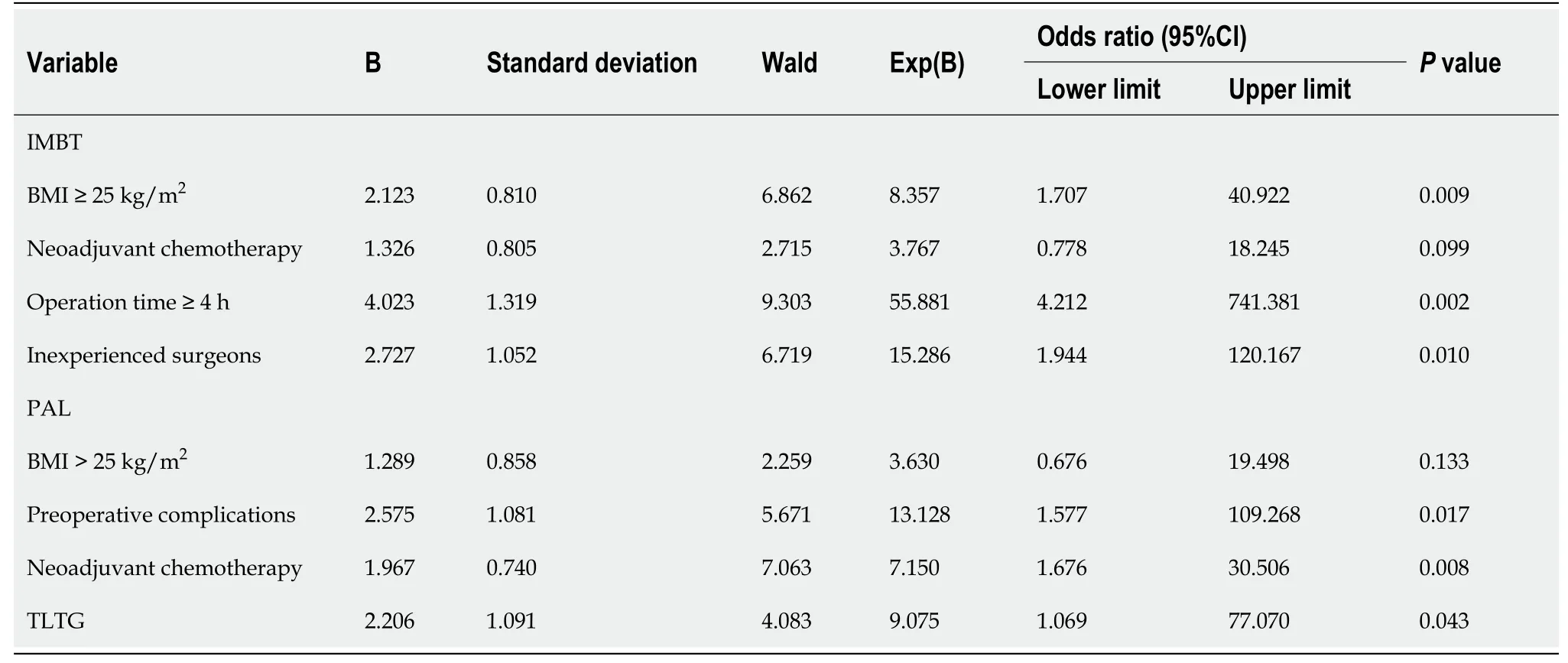
Table 5 Risk factors for positive intraoperative methylene blue testing and postoperative anastomotic leaks analyzed by multivariate analysis
Comparison of incidence of PALs
PAL occurred in 15 (2.9%) patients, including 2 in the IMBT group and 13 in the control group. The rate of PALs was significantly lower in the IMBT group than in the control group [2 of 211 patients (0.9%)vs13 of 302 patients (4.3%),P= 0.0026].
Risk factors for PALs
The clinical characteristics of the patients with anastomotic leaks are shown in Table 6. The diagnosis time of PALs was 5.8 ± 2.0 d after surgery, postoperative hospital stay was 19.3 ± 3.5 d, and theabdominal drainage tube placement time was 17.3 ± 3.2 d. All 15 patients improved and were discharged from the hospital, and no one died. In the univariate analysis, patients with BMI > 25 kg/m2(8.8%vs2.4%,P= 0.025), preoperative complications (8.1%vs2.0%,P= 0.018), totally laparoscopic total gastrectomy (6.8%vs1.9%,P= 0.046), and neoadjuvant chemotherapy (9.8%vs2.9%,P= 0.028) were associated with PALs, as shown in Tables 3 and 4. Multivariate analysis showed that preoperative complications (hazard ratio [HR] = 13.128,P= 0.017), totally laparoscopic total gastrectomy (HR = 9.075,P= 0.043), and neoadjuvant chemotherapy (HR = 7.150,P= 0.008) were independent risk factors for PALs (Table 5).

Table 6 Characteristics of postoperative anastomotic leaks
DlSCUSSlON
Anastomotic leaks are among the most common and severe complications after totally laparoscopic radical gastrectomy and are the main risk factor for patients' postoperative death[8-10]. The integrity of the anastomosis, which is closely related to the anastomotic technique, is a prerequisite for tissue healing and is essential for preventing anastomotic leaks[6,12]. In totally laparoscopic radical gastrectomy, we used IMBT to check the integrity of the anastomosis. The results showed that IMBT reduces the incidence of PALs, which is consistent with the IMBT results in open total gastrectomy[14].
Several methods are available to assess the integrity of the anastomosis. An intraoperative air leak test was proposed by Kanaji to check anastomotic integrity during open radical gastrectomy[6] and showed that this test reduces the occurrence of postoperative anastomotic leaks; however, the intraoperative air leak test did not show the exact site of the leaks and only depicted the approximate area. Celiket al[14]showed a low incidence of anastomotic leaks in the methylene blue testing group (3.7%vs14.4%,P=0.007) in which methylene blue is injectedviaa nasogastric tube to check the integrity of the anastomosis during an open total gastrectomy. Some researchers[31] who performed an intraoperative endoscopic examination during laparoscopic gastric bypass surgery showed a low incidence of anastomotic leaks (0vs8%,P= 0.0412) and a low reoperation rate (0vs8%,P= 0.0412). However, it is a challenge to find gastroscopic instruments as well as an experienced endoscopist. Our study confirmed that IMBT is an important method for assessing anastomotic integrity in totally laparoscopic radical gastrectomy, which detects anastomoses and pinpoints the areas of the leaks. Furthermore, we examined the anastomosis during totally laparoscopic distal gastrectomy, whereas previous studies focused on esophagojejunalanastomotic leaks after total gastrectomy.
This study found seven IMBT-positive patients whose anastomosis was reinforced with sutures, and none of them developed PALs. Our study indicated that patients with an operative time > 4 h, those with a BMI > 25 kg/m2, and insufficient surgical experience were associated with a higher risk of positive IMBT. Previous studies have shown that technically relevant factors such as prolonged operative time, excessive BMI, and inexperience of the surgeon are strongly associated with the occurrence of PALs[6,32-33]. Therefore, we recommend performing IMBT in patients with these highrisk factors.
However, two patients (0.9%) with negative IMBT developed PALs in this study, meaning that the cause of the anastomotic leaks is complex. This study found that patients with preoperative complications, totally laparoscopic total gastrectomy, and neoadjuvant chemotherapy are at a higher risk for PALs. Previous studies have indicated that anemia, malnutrition, and pulmonary insufficiency are also strongly associated with the occurrence of PALs[13,32,34], and are consistent with the results of our study. Kawamuraet al[35] showed that the rate of anastomotic leaks is significantly higher in the laparoscopic total gastrectomy group (5.0 %) than in the laparoscopic distal gastrectomy group (1.2%), which is consistent with our study. However, there is still controversy about whether neoadjuvant chemotherapy leads to PALs. Goruret al[36] reported that chemotherapy affects cell proliferation and the formation of collagenous fiber, which is a key component of anastomotic healing. Some studies reported that neoadjuvant chemotherapy does not increase the risk of PALs[37,38]. Our study suggested that neoadjuvant chemotherapy is a risk factor for PALs. We hypothesized that patients undergoing neoadjuvant chemotherapy have increased tissue toughness and adhesion within the abdominal cavity,resulting in increased surgical damage, thus leading to PALs. Therefore, we should pay close attention to patients with the above-mentioned risk factors.
This study has its limitations. First, it is a single-center retrospective study, which needs to be further confirmed by a multicenter, randomized controlled study with a larger sample size. Second, our study did not compare the IMBT, intraoperative air leak test, and intraoperative endoscopy. Finally, the methylene blue testing could not prevent PALs caused by non-technical factors.
CONCLUSlON
In summary, IMBT can find technical defects within an anastomosis, and suturing can reduce the incidence of anastomotic leaks after totally laparoscopic radical gastrectomy. Independent risk factors associated with PALs include preoperative complications, totally laparoscopic total gastrectomy, and neoadjuvant chemotherapy.
ARTlCLE HlGHLlGHTS
Research background
We hypothesized that intraoperative methylene blue testing (IMBT) could reduce the incidence of postoperative anastomotic leaks (PALs) in totally laparoscopic radical gastrectomy.
Research motivation
IMBT, air leak testing, or endoscopy is used to assess the anastomotic integrity of esophagojejunostomy during open total gastrectomy for gastric cancer. To the best of our konwledge, this is the first study to assess the anastomotic integrity during totally laparoscopic radical gastrectomy.
Research objectives
To explore the effects of IMBT on the incidence of PALs and identify the risk factors for PALs in totally laparoscopic radical gastrectomy.
Research methods
The difference in the incidence of PALs was compared between the IMBT group and the control group.Logistic regression analysis was used to clarify the risk factor for positive IMBT and PALs.
Research results
Positive IMBT was shown in 7 patients (3.3%) in the IMBT group, and no PAL occurred in these patients after suture reinforcement. Moreover, 15 patients (2.9%) developed PALs, and the rate of PALs was significantly lower in the IMBT group than in the control group [2 of 211 patients (0.9%) vs 13 of 302 patients (4.3%), P = 0.0026]. Further analysis demonstrated that preoperative complications (hazard ratio[HR] = 13.128, P = 0.017), totally laparoscopic total gastrectomy (HR = 9.075, P = 0.043), and neoadjuvant chemotherapy (HR = 7.150, P = 0.008) were independent risk factors for PALs.
Research conclusions
IMBT can find technical defects within an anastomosis, and suturing can reduce the incidence of PALs in totally laparoscopic radical gastrectomy. Independent risk factors associated with PAL include preoperative complications, totally laparoscopic total gastrectomy, and neoadjuvant chemotherapy.
Research perspectives
Randomized controlled trials are expected to be conducted to measure the effects of IMBT.
ACKNOWLEDGEMENTS
We thank Zhu JF for his review of our statistics.
FOOTNOTES
Author contributions:Deng C designed and performed the research and wrote the paper; Liu Y, Zhang ZY, and Qi HD designed the research and supervised the report; Guo Z and Zhao X provided clinical advice; Li XJ designed and performed the research and supervised the report.
lnstitutional review board statement:This study was reviewed and approved by the Ethics Committee of the Shaanxi Provincial People's Hospital.
lnformed consent statement:Patients were not required to give informed consent to the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent.
Conflict-of-interest statement:We have no financial relationships to disclose.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Chun Deng 0000-0002-6517-9924; Yang Liu 0000-0003-1047-7454; Zhen-Yu Zhang 0000-0002-9891-6716;Heng-Duo Qi 0000-0002-2093-4711; Xu Zhao 0000-0002-5407-2400; Xiao-Jun Li 0000-0002-3355-6529.
S-Editor:Wu YXJ
L-Editor:Wang TQ
P-Editor:Wu YXJ
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- lmaging of acute appendicitis: Advances
- Laparoscopic-assisted endoscopic full-thickness resection of a large gastric schwannoma: A case report
- Surgical timing for primary encapsulating peritoneal sclerosis: A case report and review of literature
- Subacute liver and respiratory failure after segmental hepatectomy for complicated hepatolithiasis with secondary biliary cirrhosis: A case report
- Clinical outcomes of endoscopic resection of superficial nonampullary duodenal epithelial tumors: A 10-year retrospective,single-center study
- Laparoscopic-assisted vs open transhiatal gastrectomy for Siewert type ll adenocarcinoma of the esophagogastric junction: A retrospective cohort study