Role of endoscopic ultrasound in esophageal cancer
2022-05-18MarkRadlinskiVanessaShami
INTRODUCTION
The role of endoscopic ultrasound in esophageal cancer
There will be an estimated 19260 new cases of esophageal cancer (ECA) in the United States in 2021,which accounts for 1.0% of all new cancer cases.The lifetime risk for development of ECA in the United States is 1 in 125 for men and 1 in 417 for women[1].Mortality from the disease is significant,with an estimated 15530 deaths in 2021,accounting for 2.6% of all cancer related deaths.When evaluating the data from 2011-2017,the 5-year survival rate was found to be 19.9%[2].The associated survival rate depends on the stage of the cancer when it is first diagnosed.At the time of diagnosis,a significant subset of patients has either locally advanced or metastatic disease,with 34% of patients having regional spread and 39% of patients having distant or metastatic spread.Unfortunately,only 10% of patients present with localized disease.Five-year survival rates,as expected,vary based on disease extent found on index evaluation.The 5-year survival rate for localized disease is 46.4%,regional disease is 25.6%,and distant/metastatic disease is 5.2%.
The workup for esophageal and esophagogastric junction cancers requires accurate staging as treatment protocols are stage dependent.Upper gastrointestinal endoscopy is essential for the initial evaluation of an esophageal mass.Endoscopy with biopsies is often sufficient to establish the diagnosis of ECA,but in the rare instances that biopsies are nondiagnostic,endoscopic ultrasound (EUS),with fine needle aspiration (FNA) of the esophageal wall,can be utilized for tissue diagnosis[3].Currently,ECA staging as defined by the American Joint Committee on Cancer staging system utilizes tumor-nodemetastasis subclassifications,otherwise known as TNM.The TNM classifications refer to the primary tumor (T stage),regional lymph node status (N stage),and presence or absence of metastatic disease (M classification)[4].After the initial diagnosis of cancer is made,the National Comprehensive Cancer Network recommends obtaining a computed tomography (CT) of the chest/abdomen/pelvis to assess for metastatic disease (this can also help to define local extent of disease and nodal involvement albeit not as well as EUS in most cases).If there is no overt evidence of M1 disease on cross sectional imaging,then both EUS and positron emission tomography (PET) are indicated at this time for further evaluation[5].The primary strength of EUS as part of this algorithm is in the ability to establish the extent of locoregional involvement in patients without overt metastatic disease.
Since treatment options for ECA are stage dependent,EUS plays an important role by providing accurate T and N staging.Specifically,EUS helps differentiate patients that should undergo neoadjuvant chemotherapy from patients that would benefit from primary surgical resection.
Importance of esophagogastroduodenoscopy examination
In general,the endoscopic report during the workup for ECA should include several components,including the anatomic landmarks,location of the lesion in question,circumferential extent of the cancer,and the general mucosal appearance.The importance of accurately describing the location of the tumor cannot be overemphasized,as many of the cancers labeled as esophageal are in fact either junctional or primary cardiac/gastric.This distinction is primarily determined by where the bulk of the tumor is.The endoscopist needs carefully to examine and document if the cancer involves the cardia or crosses the junction and how long (in cm) it extends proximal to the esophagogastric junction.Additionally,it is important to look for “skip” lesions (submucosal proximal extension of the cancer) so that the surgeons are aware of the extent of the cancer proximally (Figure 1).Similarly,it is important to document if there is Barrett’s esophagus that extends proximal to the cancer,since ideally this will also be resected if the patient is appropriate for surgery.Additionally,the most stenotic part of the tumor should be documented so that the endoscopist is aware and proceeds with appropriate caution when passing a larger diameter,often oblique viewing,echoendoscope.

EUS AND STAGING
T-Staging
Standard echoendoscopes operate at a frequency of 7.5-12 mHz.EUS can be performed using a radial or linear platform.Radial EUS images at a plane that is perpendicular to the long access of the scope,so the echo ultrasonographer can get a circumferential or 360 view of the ECA.These images are similar to interpreting axial CT slices (Figure 2A).Linear EUS,on the other hand,images parallel to the long access of the scope,and while T-staging is sometimes more challenging,use of this scope allows for performance of FNA or fine needle biopsy (FNB) if needed (Figure 2B).While choice of platform is typically operator dependent,it is common practice that endoscopists start with radial EUS because of the circumferential view.This can be switched to a linear EUS if something is found that needs FNA,such as a lymph node or liver lesion.

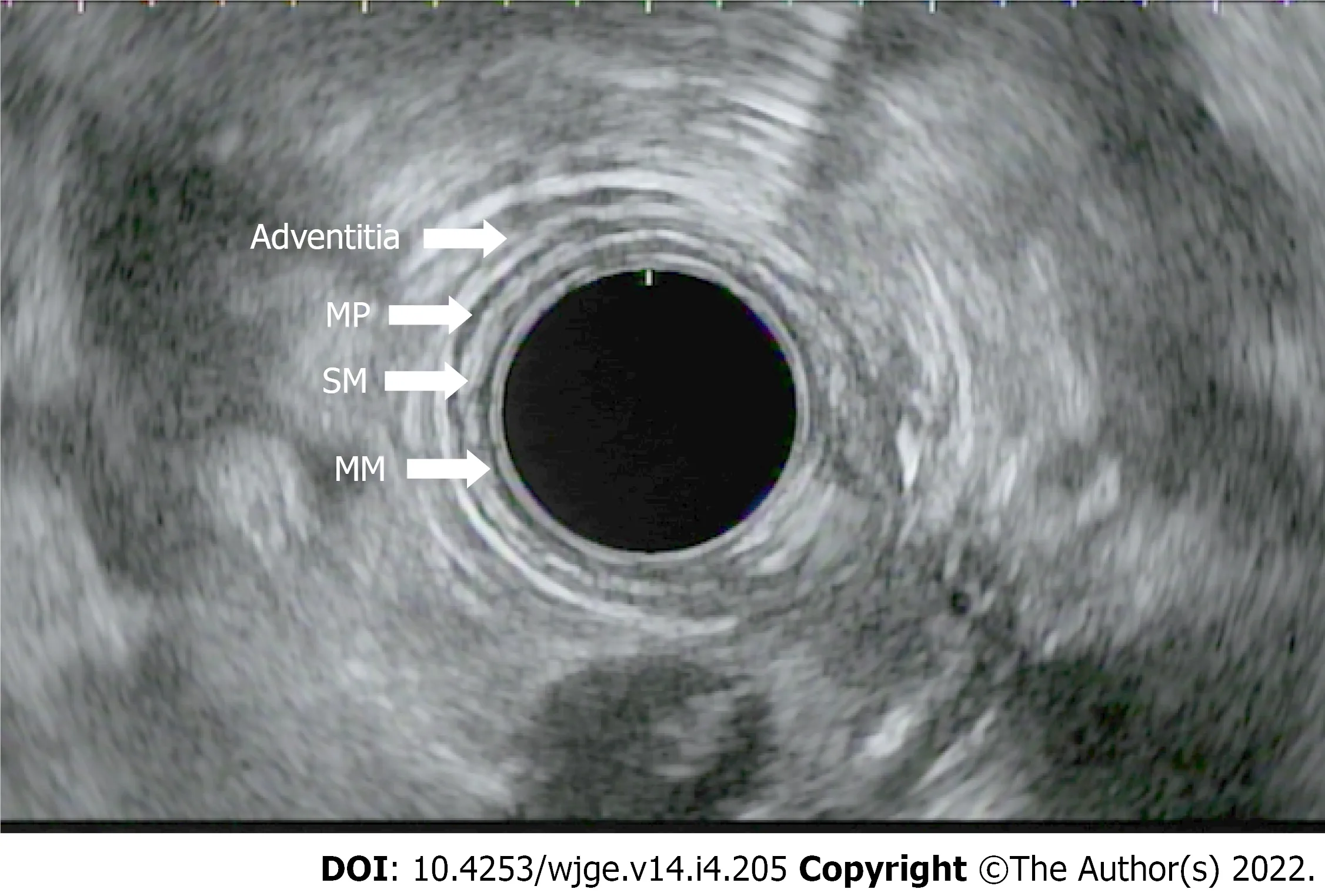
After identifying the distal and proximal extent of the cancer,the T-stage is determined.T staging refers to the depth of tumor invasion with respect to the extent of esophageal wall layer involvement.The esophageal wall is comprised of the mucosa,submucosa,muscularis propria,and adventitia.The mucosal wall layer is further subdivided into the epithelium,lamina propria,and muscularis mucosae.A basement membrane separates the muscularis mucosae from the submucosa.EUS helps to define the esophagus as a five layered structure with the first layer (hyperechoic) representing the superficial mucosa,the second (hypoechoic) representing the deep mucosa,the third (hyperechoic) representing the submucosa,the fourth (hypoechoic) the muscularis propria,and the fifth (hyperechoic) the adventitia (Figure 3).When reporting the T stage,the endosonographic report should also include the maximal wall thickness of the cancer.
In his book The Great Lili, Carlton Jackson records that Nazi19 propaganda minister Josegh Goebbels detested20 “Lili.” He wanted morale-boosters like “Bombs on England”. He ordered the original master copy of Lale Andersen s recording17 destroyed. When Stalingrad fell in January 1943, after 300,000 German soldiers had been killed, Goebbels banned the song entirely21, saying that “a dance of death roamed throughout its bard22.”
Both authors have written and reviewed the manuscript in its entirety.
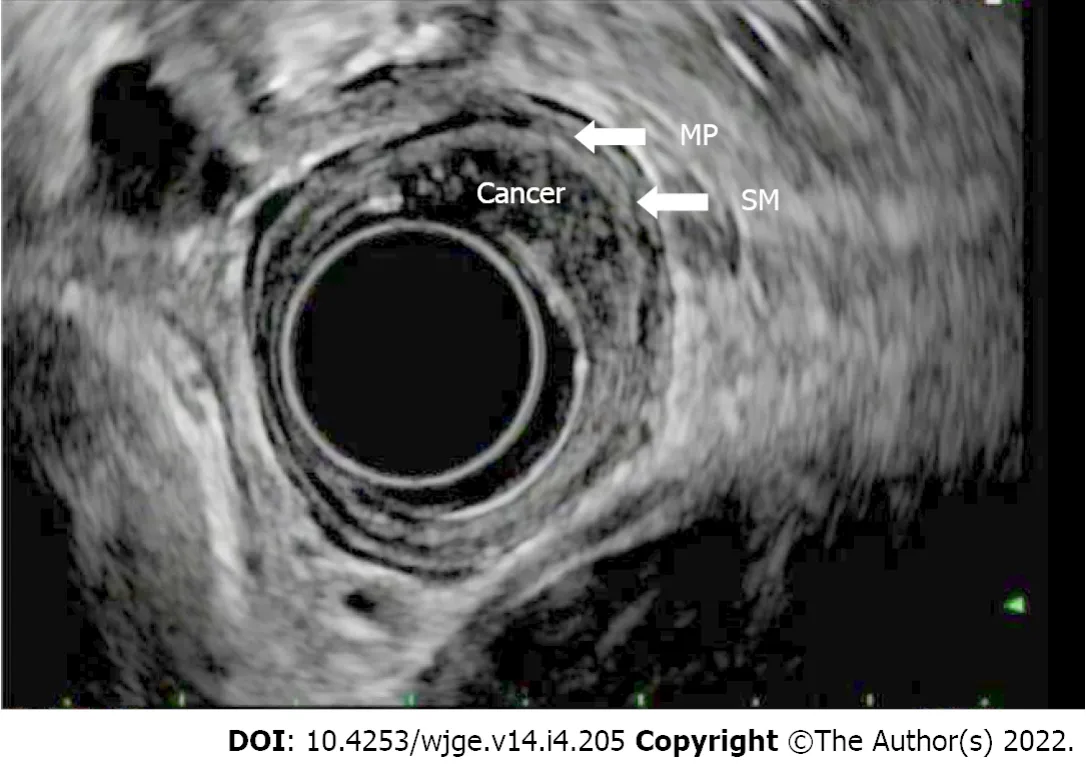
T(is) refers to high grade dysplasia that is limited to the epithelium and does not penetrate the lamina propria.T1a tumors invade the lamina propria and/or muscularis mucosae,whereas T1b lesions invade into (but not through) the submucosa.By EUS,a T1a layer would invade through the first endosonographic,hyperechoic layer and possibly invade into,but not through the second hypoechoic later.T1b lesions would invade into,but not through the third,hyperechoic layer (Figure 4).T2 lesions invade past the submucosa into the muscularis propria (but do not breach the outer border).By EUS,these would invade into,but not through,the fourth (hypoechoic) layer.T3 lesions invade past the muscularis propria into the adventitia (Figure 5).By EUS,this would denote invasion past the fourth endosonographic layer into the fifth (hyperechoic) layer.T4a and T4b both invade structures adjacent to the esophagus,but T4a are considered resectable (invasion of pleura,pericardium,diaphragm),while T4b are considered unresectable (invasion of the aorta,vertebral body,trachea) (Figure 6).The true positive rate for EUS T-staging ranges between 0.89 (0.86-0.92),as gathered by one meta-analysis of 27 primary articles[6].


The accuracy of EUS lessens in staging cancers not on either ends of the spectrum (T1 or T/4).In a study by Tekola
[7],38 patients with ECA who were staged as T2N0 underwent surgery.EUS under staged 32% of these tumors.Other data have shown that up to 55% of tumors staged as T2N0 were shown to have nodal disease on resection.For this reason,many patients staged with T2N0 cancers are now undergoing preoperative chemoradiation.This practice is supported by Capovilla
[11],whose study demonstrated that patients with T2N0 esophageal and squamous cell cancers who underwent neoadjuvant therapy had a statistically higher survival rate than patients who underwent up front surgery.If future studies support this practice,then the importance/role of EUS in triaging patients to neoadjuvant
surgery may in fact diminish[7-11].
In patients with ECA who have dysphagia,the majority have advanced disease.One study showed that dysphagia was noted in 89% of patients having T3-4 ECA,while only 53% without dysphagia had T3-4 disease (
<0.001).Another study showed similar findings where the presence of dysphagia in the setting of a cancer had a sensitivity 0.89 and sensitivity of 0.88 for at least locally advanced disease.For this reason,in patients with ECA and dysphagia,EUS may be less likely to affect treatment decisions[12,13].
N-staging
Next,the N-stage is determined.The N stage refers to the presence or absence,along with the total number of regional lymph nodes affected.N0 indicates the absence of lymph node involvement,N1 denotes two involved lymph nodes,N2,three to six involved lymph nodes,and N3,seven or more lymph nodes.
Even after surgery,EUS can be utilized in determining tumor recurrence,despite post-surgical EUS surveillance not being considered standard of practice at this time.In one small study of 40 patients who had undergone prior surgical resection,3 recurrences were identified with EUS despite absence of symptoms (no reported dysphagia) and a negative CT[30].In fact,another study of 43 patients undergoing q6 mo EUS surveillance had a 92% positive predictive value for early recurrence in a population where two-thirds of those with recurrence were asymptomatic[31].
The next day was our first date and he drove1 across town to go home in midday2 traffic to get cleaned up for our date, only to turn around and come back across town in rush hour traffic to pick me up. Well, by the time he arrived at my hotel room, I had already worked a long day and I just wanted to relax. I was too old for dating, especially someone who I wasn t going to see after a couple of weeks anyway.

EUS has a pooled sensitivity of 59.5% to 97.2% sensitivity for N staging (40%-100% specificity).This is compared to a pooled sensitivity of 24% for distinguishing N0 from N1 by CT (with 100% specificity)[6].Nodal staging is important prognostically since patients with nodal involvement have been found to have worse prognosis as compared to those who do not (N0 disease).Patients with 0,1-2,and >2 malignant appearing,peri-esophageal lymph nodes on index EUS were found to have 66 mo,14.5 mo,and 6.5 mo,respectively,of median survival time[18].
M-staging
Lastly,distant lymph nodes,the liver,peritoneum,and the left adrenal gland are inspected for lesions.M staging differentiates presence of metastases (M1)
absence of metastases (M0).As previously discussed,there is a limited role for EUS if M1 disease is established on CT.However,EUS at the position of the antrum or bulb of the duodenum can provide an important means for evaluation of peripancreatic or porta hepatis lymph nodes.In the body of the stomach,EUS can evaluate the liver(Figure 8),and in the fundus and cardia,EUS can evaluate perigastric and peripancreatic lymph nodes as well as evaluate the celiac plexus (though the latter is not considered M1).Additionally,EUS can provide a detailed evaluation of the left adrenal gland and the peritoneum.An important difference between the older classification (American Joint Committee on Cancer) system and the current,affecting the utility of EUS in differentiating M0 from M1 disease,is that the involvement of a celiac lymph node is now considered regional (N) disease and no longer metastatic (M1a).
UTILITY OF EUS IN OBSTRUCTING TUMORS
EUS may not be technically feasible in patients with obstructing cancers.An obstructing tumor can be seen on presentation in up to 30% of cases.There are some risks of dilating a malignant stricture to pass an echo endoscope,including perforation[19].Additionally,it may be difficult to stage accurately a lesion following esophageal dilation given disruption of normal tissue planes.There is questionable additional benefit of endosonography following the endoscopic finding of a malignant stricture as the presence of a malignant obstruction typically denotes advanced disease (T3-T4)[20].Patients with malignant obstructions that cannot be traversed have poorer outcomes as compared to patients without evidence of stenosis,with median survivals of 10 mo
20 mo,respectively.
EUS-FNA
The utility of EUS is also diminished when evaluating early-stage ECA as there is loss of sensitivity for superficial disease.High frequency probes can help to provide better evaluation of the mucosa and the submucosa.In 75%-82% of cases,high frequency probes (12-20 MHz) can help distinguish T1a from T1b disease in patients without evidence of metastatic disease[25].This can help determine candidacy for endoscopic resection techniques as a curative option during the same session.In another study,the accuracy of T staging when using a high frequency probe was 64% as compared to a conventional radial EUS,which was 49%[26].When encountering a more superficial lesion that can be endoscopically resected,performing EUS first is helpful in confirming that the muscularis propria is uninvolved and in ruling out malignant lymphadenopathy.Once the lesion is endoscopically resected,then the true pathologic T stage is confirmed.
EUS vs other staging modalities
In one study,EUS results altered management by guiding the need for neoadjuvant chemotherapy in 34.8% of patients evaluated[22].In another retrospective study of 56 patients,EUS was superior in the ability to identify locally advanced disease,with 58.9% sensitivity as compared to 26.8% and 37.5%sensitivity for CT and PET,respectively.EUS,however,is less accurate for early-stage lesions (T1 or T2)as compared with more advanced tumors.Additionally,PET is superior for detection of distant metastasis as compared to EUS,with a sensitivity of 81%
73% and specificity of 91%
86%,respectively[23].EUS also plays an important role in detecting disease recurrence along with restaging after chemotherapy +/- radiation.
With improvements in imaging such as PET/magnetic resonance imaging (MRI),the overall utility of EUS is controversial.In one study of 74 patients undergoing preoperative staging,MRI outperformed EUS with higher specificity and accuracy in T staging[24].In patients with dysphagia or an obstructing lesion,EUS has less utility given most of these patients have locally advanced disease and thus would not be definitive surgical resection candidates.In one study evaluating 147 patients with esophageal adenocarcinoma and dysphagia,133 of these patients had a partially or completely obstructing mass on initial endoscopic evaluation.Overall,128 of these 133 (96%) patients had locally advanced disease[12].
One of the benefits of EUS,specifically linear EUS,is the ability to perform FNA and/or FNB of lymph nodes and lesions in adjacent structures.EUS with FNA has 80% sensitivity in distinguishing T4 from T1-T3 disease and 78% accuracy in nodal staging[21].In patients with T1-T2 disease,FNA can determine lymph node involvement,which in turn determines if these patients would theoretically need neoadjuvant chemotherapy or proceed directly to surgery.When performing FNA,it is important to avoid passing through the main tumor or major blood vessels to avoid both false positives as well as tumor seeding.
We have also found that EUS is challenging when evaluating early to intermediate gastroesophageal junction (GEJ) tumors.In one study evaluating EUS in GEJ tumors prior to surgical resection (in patients that had not undergone prior chemotherapy or radiation),EUS T staging was only accurate in 48% of cases (23% percent were under-staged and 29% were over-staged as correlated with pathologic T staging).This inaccuracy was even more pronounced in short segment tumors at the GEJ[27].
Role of EUS in restaging
The role of EUS in staging disease following neoadjuvant therapy is evolving.Patients are typically restaged after completion of neoadjuvant therapy to determine if the next most appropriate step is surgical resection
definitive or palliative chemotherapy.Traditionally,it was thought that EUS is less reliable following neoadjuvant chemotherapy given inflammation and fibrosis sustained during treatment,which affects the ability to interpret reliably an EUS exam.The mucosal changes following neoadjuvant chemotherapy can cause hypoechoic appearance of the esophageal wall and over-staging of tumor invasion,possibly precluding some patients from an appropriate surgical resection.Following neoadjuvant chemotherapy,a recent meta-analysis and systematic review found the sensitivity and specificity of T1 23% and 95%,T2 29% and 84%,T3 81% and 42%,and T4 43% and 96%,respectively.In the same study,the pooled sensitivity and specificity of N staging was found to be 69% and 52%,respectively[28].
Another retrospective study of 103 patients with locoregionally advanced ECA who had undergone neoadjuvant chemotherapy showed that reduced mass size,as determined by EUS (0.7
1.7 cm,
=0.01),correlated with a pathologic response[29].However,in this same cohort,fluorodeoxyglucose-PET outperformed EUS in prediction of long-term survival following neoadjuvant chemotherapy (in patients following neoadjuvant chemotherapy but prior to surgical resection).
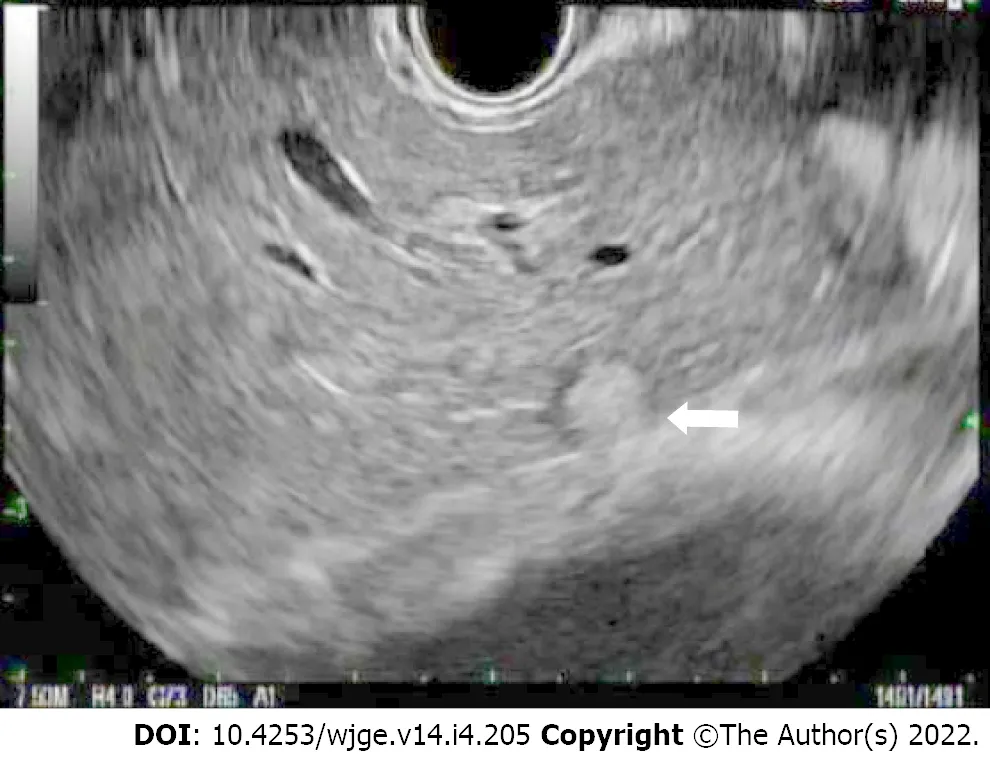
Endosonographic characteristics of lymph nodes that suggest malignant potential include size greater than 1 cm,round shape,sharp and demarcated borders,and hypoechoic echotexture (Figure 7).When a lymph node is found to possess all four of these aforementioned features,the accuracy of predicting a malignant lymph node is 80%-100%[14,15].The location of the lymph node may also be informative in differentiation of benign and malignant.For example,the presence of celiac lymph nodes usually indicates pathology since they are not usually present.In one study,89% of endosonographically detectable celiac lymph nodes were confirmed to be malignant on FNA[16].Another predictor of malignant lymph node status includes association with T3-T4 staged lesions[17].
In one meta-analysis,the pooled sensitivity for detecting complete pathologic response following neoadjuvant therapy was 0.35,0.62,0.01,and 0.08 for CT,PET-CT,EUS,and MRI,respectively.While the sensitivity of EUS was poor,specificity was 0.99 as compared to 0.83,0.73,and 0.83 for CT,PET-CT,and MRI,respectively[32].
One day his queen presented him with a baby daughter as beautiful as the dawn, and the king himself was so happy and delighted that, for a whole week, he forgot to hunt, and spent the time in public and private rejoicing
Alan woke up at 4:30 on Tuesday for his morning flight to San Francisco. As he kissed our five-year-old daughter Sonali and me good-bye, I pulled him toward me, knocking him over. He laughed heartily4 and said, I ll return with the pot of gold.
One multicenter study evaluating 138 patients before and after neoadjuvant therapy showed that EUS was able to detect adequately residual disease in 90% of patients 12 wk following therapy.Specifically,EUS was able to detect residual thickness and residual area of the tumor[33].Another meta-analysis evaluating EUS for restaging following neoadjuvant chemotherapy found that EUS had a pooled sensitivity and specificity of 81% and 42% in T3 tumors (with markedly lower sensitivities of 23%,29%,and 43% in T1,T2,and T4 tumors,respectively)[28].
This was great sorrow to the little mermaid; she knew how much more sweetly she herself could sing once, and she thought, “Oh if he could only know that! I have given away my voice forever, to be with him
EUS special considerations
Other considerations when discussing the role of EUS in the staging of ECA include the cost effectiveness.EUS performed prior to treatment decisions has been found to save $3443 per patient in its ability to identify stage 1 or stage 4 disease and avoid inappropriate neoadjuvant chemotherapy or surgery[34].In patients without metastatic disease,EUS is the least expensive staging modality for ECA($13811) as compared to CT-guided FNA ($14350) or surgery ($13992).While CT is the most appropriate initial staging test in most cases,EUS can theoretically suffice as a reasonable initial study as demonstrated in one single center study.EUS found advanced disease more frequently than CT (44 %
13%) and is cheaper ($804
$844) than CT (in cases where the probability of finding advanced disease is less than 20%)[35].
It is also important to note that performing high quality EUS is provider dependent and can vary with skill level and experience.In general,it is believed that at least 100 examinations are needed for a provider to provide T-staging reliably and accurately in ECA.High quality EUS examination also has been shown to improve survival in one randomized control trial of 223 patients with non-metastatic gastroesophageal cancer (hazard ratio of 0.706 with 95% confidence interval from 0.501 to 0.966)[36].
CONCLUSION
EUS has an important role in the staging of ECA.It is superior to cross sectional imaging in the locoregional staging of ECA.Unlike cross sectional imaging,it also has the added advantage to perform FNA and/or FNB of surrounding lymph nodes and organs and,consequently,alter management.Instances when EUS may not be as beneficial are in patients with dysphagia since they most likely have at least advanced locoregional disease and would undergo neoadjuvant or definitive therapy depending on their M status.While less accurate,EUS has an evolving role in neoadjuvant therapy.Since the performance of EUS is operator dependent,it should ideally be performed by physicians specifically trained in EUS.
It happened that where the Prince s father lay buried, there grew a rosetree--a most beautiful rose tree, which blossomed only once in every fiveyears, and even then bore only one flower, but that was a rose! It smelt2 sosweet that all cares and sorrows were forgotten by him who inhaled3 itsfragrance.
And what, said the tiger-lily? “Hark, do you hear the drum?— ‘turn, turn,’—there are only two notes, always, ‘turn, turn.’ Listen to the women’s song of mourning! Hear the cry of the priest! In her long red robe stands the Hindoo widow by the funeral pile. The flames rise around her as she places herself on the dead body of her husband; but the Hindoo woman is thinking of the living one in that circle; of him, her son, who lighted those flames. Those shining eyes trouble her heart more painfully than the flames which will soon consume her body to ashes. Can the fire of the heart be extinguished in the flames of the funeral pile?”
EUS is particularly helpful with respect to T staging as we can accurately visualize and delineate the esophageal wall layers.Treatment decisions are partially dependent on T staging since depth of cancer penetration is important in predicting the risk of lymph node metastasis.Treatment for locally advanced disease,defined as stage IIB through IIIC,typically is neoadjuvant chemotherapy,with the goal to proceed with surgical resection following restaging,if appropriate.Neoadjuvant chemotherapy is associated with superior pathologic response and improved outcomes in these patients.For patients with surgically unresectable tumors or patients who are poor surgical candidates,definitive chemotherapy is offered.
Look! said the barber, here comes something in the nick of time! seized basin and soap, made a lather2 whilst the hare was approaching, and then, as it ran at full tilt3, shaved its moustaches, without cutting it or injuring a single hair on its body
Mark Radlinski has no conflict of interests
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
United States
Mark Radlinski 0000-0002-5078-577X;Vanessa M Shami 0000-00001-7528-5141.
It s for my sister, he told her, desperate to reverse the bad impression he was making. It had happened to him often here; he was too forward or direct and gave offense39. The robe slipped to the floor and he bent to pick it up, his face flushing as he rose. Her gloves were lying on the glass, her bare hands folded lightly next to them. His discomfort40 seemed to soften41 her, for when he met her eyes again, they were kind.
Chang KL
She beckoned to them, and smiled, and wanted to tell them how happy and well off she was; but the cabin-boy approached, and when her sisters dived down he thought it was only the foam of the sea which he saw
Filipodia
Chang KL
1 Statistics for Esophageal Cancer:Esophageal Cancer Stats.[cited 19 May 2021].Available from:www.cancer.org/cancer/esophagus-cancer/about/key-statistics.html
2 Cancer Stat Facts:Esophageal Cancer.NIH.[cited 19 May 2021].Available from:https://seer.cancer.gov/statfacts/html/esoph.html
3 Faigel DO,Deveney C,Phillips D,Fennerty MB.Biopsy-negative malignant esophageal stricture:diagnosis by endoscopic ultrasound.
1998;93:2257-2260 [PMID:9820410 DOI:10.1111/j.1572-0241.1998.00629.x]
4 Rice TW,Patil DT,Blackstone EH.8th edition AJCC/UICC staging of cancers of the esophagus and esophagogastric junction:application to clinical practice.
2017;6:119-130 [PMID:28447000 DOI:10.21037/acs.2017.03.14]
5 Ajani JA,D'Amico TA,Bentrem DJ,Chao J,Corvera C,Das P,Denlinger CS,Enzinger PC,Fanta P,Farjah F,Gerdes H,Gibson M,Glasgow RE,Hayman JA,Hochwald S,Hofstetter WL,Ilson DH,Jaroszewski D,Johung KL,Keswani RN,Kleinberg LR,Leong S,Ly QP,Matkowskyj KA,McNamara M,Mulcahy MF,Paluri RK,Park H,Perry KA,Pimiento J,Poultsides GA,Roses R,Strong VE,Wiesner G,Willett CG,Wright CD,McMillian NR,Pluchino LA.Esophageal and Esophagogastric Junction Cancers,Version 2.2019,NCCN Clinical Practice Guidelines in Oncology.
2019;17:855-883 [PMID:31319389 DOI:10.6004/jnccn.2019.0033]
6 Kelly S,Harris KM,Berry E,Hutton J,Roderick P,Cullingworth J,Gathercole L,Smith MA.A systematic review of the staging performance of endoscopic ultrasound in gastro-oesophageal carcinoma.
2001;49:534-539 [PMID:11559651 DOI:10.1136/gut.49.4.534]
7 Tekola BD,Sauer BG,Wang AY,White GE,Shami VM.Accuracy of endoscopic ultrasound in the diagnosis of T2N0 esophageal cancer.
2014;45:342-346 [PMID:24788081 DOI:10.1007/s12029-014-9616-9]
8 Kountourakis P,Correa AM,Hofstetter WL,Lee JH,Bhutani MS,Rice DC,Komaki R,Maru DM,Ross WA,Vaporciyan A,Swisher SG,Ajani JA.Combined modality therapy of cT2N0M0 esophageal cancer:the University of Texas M.D.Anderson Cancer Center experience.
2011;117:925-930 [PMID:20960497 DOI:10.1002/cncr.25651]
9 Rice TW,Mason DP,Murthy SC,Zuccaro G Jr,Adelstein DJ,Rybicki LA,Blackstone EH.T2N0M0 esophageal cancer.
2007;133:317-324 [PMID:17258554 DOI:10.1016/j.jtcvs.2006.09.023]
10 Stiles BM,Mirza F,Coppolino A,Port JL,Lee PC,Paul S,Altorki NK.Clinical T2-T3N0M0 esophageal cancer:the risk of node positive disease.
2011;92:491-6;discussion 496 [PMID:21704291 DOI:10.1016/j.athoracsur.2011.04.004]
11 Capovilla G,Moletta L,Pierobon ES,Salvador R,Provenzano L,Zanchettin G,Costantini M,Merigliano S,Valmasoni M.Optimal Treatment of cT2N0 Esophageal Carcinoma:Is Upfront Surgery Really the Way?
2021;28:8387-8397 [PMID:34142286 DOI:10.1245/s10434-021-10194-9]
12 Mansfield SA,El-Dika S,Krishna SG,Perry KA,Walker JP.Routine staging with endoscopic ultrasound in patients with obstructing esophageal cancer and dysphagia rarely impacts treatment decisions.
2017;31:3227-3233 [PMID:27864719 DOI:10.1007/s00464-016-5351-6]
13 Ripley RT,Sarkaria IS,Grosser R,Sima CS,Bains MS,Jones DR,Adusumilli PS,Huang J,Finley DJ,Rusch VW,Rizk NP.Pretreatment Dysphagia in Esophageal Cancer Patients May Eliminate the Need for Staging by Endoscopic Ultrasonography.
2016;101:226-230 [PMID:26603024 DOI:10.1016/j.athoracsur.2015.06.062]
14 Catalano MF,Sivak MV Jr,Rice T,Gragg LA,Van Dam J.Endosonographic features predictive of lymph node metastasis.
1994;40:442-446 [PMID:7926534 DOI:10.1016/s0016-5107(94)70206-3]
15 Bhutani MS,Hawes RH,Hoffman BJ.A comparison of the accuracy of echo features during endoscopic ultrasound (EUS)and EUS-guided fine-needle aspiration for diagnosis of malignant lymph node invasion.
1997;45:474-479 [PMID:9199903 DOI:10.1016/s0016-5107(97)70176-7]
16 Eloubeidi MA,Wallace MB,Reed CE,Hadzijahic N,Lewin DN,Van Velse A,Leveen MB,Etemad B,Matsuda K,Patel RS,Hawes RH,Hoffman BJ.The utility of EUS and EUS-guided fine needle aspiration in detecting celiac lymph node metastasis in patients with esophageal cancer:a single-center experience.
2001;54:714-719 [PMID:11726846 DOI:10.1067/mge.2001.119873]
17 Vazquez-Sequeiros E,Wiersema MJ,Clain JE,Norton ID,Levy MJ,Romero Y,Salomao D,Dierkhising R,Zinsmeister AR.Impact of lymph node staging on therapy of esophageal carcinoma.
2003;125:1626-1635 [PMID:14724814 DOI:10.1053/j.gastro.2003.08.036]
18 Chen J,Xu R,Hunt GC,Krinsky ML,Savides TJ.Influence of the number of malignant regional lymph nodes detected by endoscopic ultrasonography on survival stratification in esophageal adenocarcinoma.
2006;4:573-579 [PMID:16630763 DOI:10.1016/j.cgh.2006.01.006]
19 Hancock SM,Gopal DV,Frick TJ,Pfau PR.Dilation of malignant strictures in endoscopic ultrasound staging of esophageal cancer and metastatic spread of disease.
2011;2011:356538 [PMID:22203779 DOI:10 .1155/2011/356538]
20 Pfau PR,Ginsberg GG,Lew RJ,Faigel DO,Smith DB,Kochman ML.Esophageal dilation for endosonographic evaluation of malignant esophageal strictures is safe and effective.
2000;95:2813-2815 [PMID:11051353 DOI:10.1111/j.1572-0241.2000.02309.x]
21 Cerfolio RJ,Bryant AS,Ohja B,Bartolucci AA,Eloubeidi MA.The accuracy of endoscopic ultrasonography with fineneedle aspiration,integrated positron emission tomography with computed tomography,and computed tomography in restaging patients with esophageal cancer after neoadjuvant chemoradiotherapy.
2005;129:1232-1241 [PMID:15942562 DOI:10.1016/j.jtcvs.2004.12.042]
22 Pfau PR,Perlman SB,Stanko P,Frick TJ,Gopal DV,Said A,Zhang Z,Weigel T.The role and clinical value of EUS in a multimodality esophageal carcinoma staging program with CT and positron emission tomography.
2007;65:377-384 [PMID:17321235 DOI:10.1016/j.gie.2006.12.015]
23 Lowe VJ,Booya F,Fletcher JG,Nathan M,Jensen E,Mullan B,Rohren E,Wiersema MJ,Vazquez-Sequeiros E,Murray JA,Allen MS,Levy MJ,Clain JE.Comparison of positron emission tomography,computed tomography,and endoscopic ultrasound in the initial staging of patients with esophageal cancer.
2005;7:422-430 [PMID:16270235 DOI:10.1007/s11307-005-0017-0]
24 Guo J,Wang Z,Qin J,Zhang H,Liu W,Zhao Y,Lu Y,Yan X,Zhang Z,Zhang T,Zhang S,Dominik NM,Kamel IR,Li H,Qu J.A prospective analysis of the diagnostic accuracy of 3 T MRI,CT and endoscopic ultrasound for preoperative T staging of potentially resectable esophageal cancer.
2020;20:64 [PMID:32912319 DOI:10.1186/s40644-020-00343-w]
25 Shah PM,Gerdes H.Endoscopic options for early stage esophageal cancer.
2015;6:20-30 [PMID:25642334 DOI:10.3978/j.issn.2078-6891.2014.096]
26 Wu LF,Wang BZ,Feng JL,Cheng WR,Liu GR,Xu XH,Zheng ZC.Preoperative TN staging of esophageal cancer:comparison of miniprobe ultrasonography,spiral CT and MRI.
2003;9:219-224 [PMID:12532435 DOI:10.3748/wjg.v9.i2.219]
27 Dhupar R,Rice RD,Correa AM,Weston BR,Bhutani MS,Maru DM,Betancourt SL,Rice DC,Swisher SG,Hofstetter WL.Endoscopic Ultrasound Estimates for Tumor Depth at the Gastroesophageal Junction Are Inaccurate:Implications for the Liberal Use of Endoscopic Resection.
2015;100:1812-1816 [PMID:26233274 DOI:10.1016/j.athoracsur.2015.05.038]
28 Sun F,Chen T,Han J,Ye P,Hu J.Staging accuracy of endoscopic ultrasound for esophageal cancer after neoadjuvant chemotherapy:a meta-analysis and systematic review.
2015;28:757-771 [PMID:25168285 DOI:10.1111/dote.12274]
29 Swisher SG,Maish M,Erasmus JJ,Correa AM,Ajani JA,Bresalier R,Komaki R,Macapinlac H,Munden RF,Putnam JB,Rice D,Smythe WR,Vaporciyan AA,Walsh GL,Wu TT,Roth JA.Utility of PET,CT,and EUS to identify pathologic responders in esophageal cancer.
2004;78:1152-60;discussion 1152 [PMID:15464463 DOI:10.1016/j.athoracsur.2004.04.046]
30 Catalano MF,Sivak MV Jr,Rice TW,Van Dam J.Postoperative screening for anastomotic recurrence of esophageal carcinoma by endoscopic ultrasonography.
1995;42:540-544 [PMID:8674924 DOI:10.1016/s0016-5107(95)70007-2]
31 Fockens P,Manshanden CG,van Lanschot JJ,Obertop H,Tytgat GN.Prospective study on the value of endosonographic follow-up after surgery for esophageal carcinoma.
1997;46:487-491 [PMID:9434213 DOI:10.1016/s0016-5107(97)70001-4]
32 de Gouw DJJM,Klarenbeek BR,Driessen M,Bouwense SAW,van Workum F,Fütterer JJ,Rovers MM,Ten Broek RPG,Rosman C.Detecting Pathological Complete Response in Esophageal Cancer after Neoadjuvant Therapy Based on Imaging Techniques:A Diagnostic Systematic Review and Meta-Analysis.
2019;14:1156-1171 [PMID:30999111 DOI:10.1016/j.jtho.2019.04.004]
33 van der Bogt RD,Noordman BJ,Krishnadath KK,Roumans CAM,Schoon EJ,Oostenbrug LE,Siersema PD,Vleggaar FP,van Lanschot JJB,Spaander MCW.Endoscopic ultrasound measurements for detection of residual disease after neoadjuvant chemoradiotherapy for esophageal cancer.
2019;51:326-332 [PMID:30497088 DOI:10.1055/a-0795-3220]
34 Shumaker DA,de Garmo P,Faigel DO.Potential impact of preoperative EUS on esophageal cancer management and cost.
2002;56:391-396 [PMID:12196778 DOI:10.1016/s0016-5107(02)70044-8]
35 Hadzijahic N,Wallace MB,Hawes RH,VanVelse A,LeVeen M,Marsi V,Hoffman BJ,Sahai AV.CT or EUS for the initial staging of esophageal cancer?
2000;52:715-720 [PMID:11115901 DOI:10.1067/mge.2000.108481]
36 Russell IT,Edwards RT,Gliddon AE,Ingledew DK,Russell D,Whitaker R,Yeo ST,Attwood SE,Barr H,Nanthakumaran S,Park KG.Cancer of Oesophagus or Gastricus - New Assessment of Technology of Endosonography(COGNATE):report of pragmatic randomised trial.
2013;17:1-170 [PMID:24034150 DOI:10.3310/hta17390]
杂志排行
World Journal of Gastrointestinal Endoscopy的其它文章
- Improving sessile serrated adenoma detection rates with high definition colonoscopy:A retrospective study
- Endoscopic retrograde cholangiopancreatography for bile duct stones in patients with a performance status score of 3 or 4
- Endoscopic ultrasound guided interventions in the management of pancreatic cancer