lmmune checkpoint inhibitor-associated ophthalmic adverse events: current understanding of its mechanisms,diagnosis, and management
2022-04-19YuWenZhouQianXuYanWangRuoLanXiaJiYanLiuXueLeiMa
INTRODUCTION
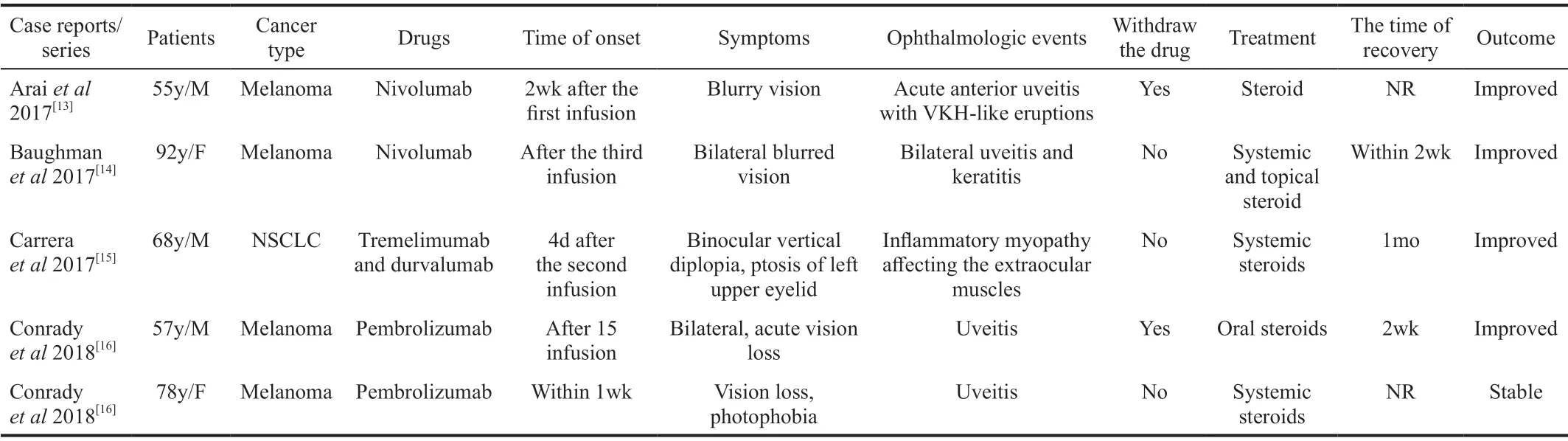
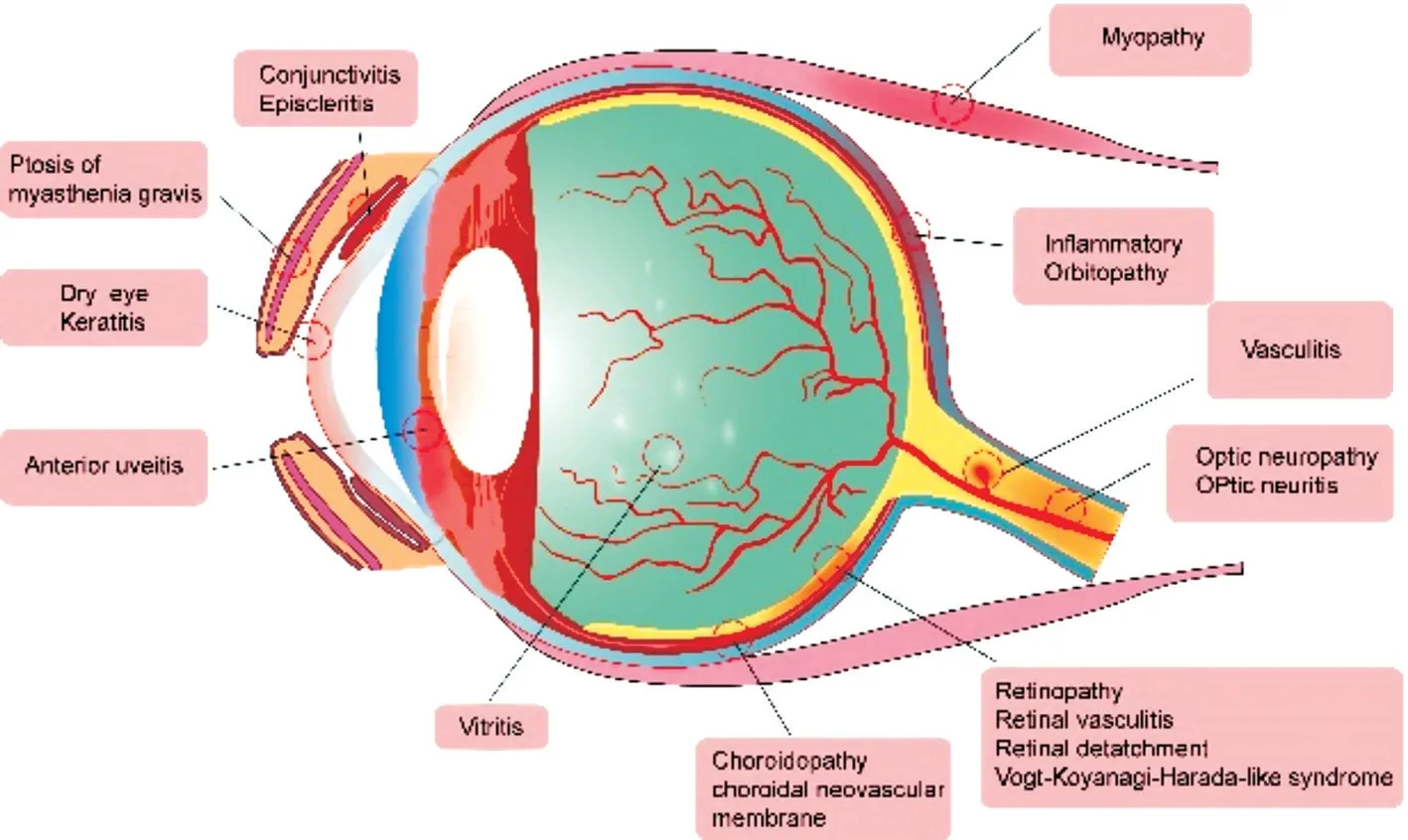
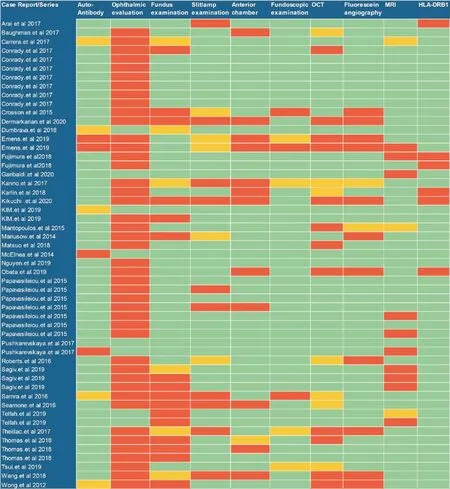
Immune checkpoint inhibitors (ICIs) that target cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed cell death protein 1 receptor/ligand (PD-1/PD-L1) pathways have shown robust evidence of antitumor activity in patients with cancer. These medications include pembrolizumab,ipilimumab, nivolumab, atezolizumab, avelumab, and durvalumaband have been authorized by the Food and Drug Administration (FDA) for numerous cancer therapies. With the progressive implementation of ICIs in clinical practice,however, a key challenge has emerged: the uncontrolled collateral effects of ICIs on the immune system, which can result immune-related adverse events (irAEs) that can affect all organ systems. IrAEs comprise common adverse events,such as dermatological, gastrointestinal, hematological,pulmonary, and rheumatic toxicities, nephritis, and endocrinopathy. They also include rare adverse events (arising in <1% of patients), such as neurological, ocular, and cardiac toxicities, which can largely be controlled by glucocorticoid therapy. Among these toxicities, ophthalmic irAEs,including dry eye, uveitis, ocular myasthenia gravis, uveal effusion, retinal detachment, and conjunctivitis (Figure 1) occur infrequently and are not comprehensively recognized. The current understanding of ophthalmic irAEs is mainly derived from case reports and case series (Table 1). In this review,to strengthen the understanding of ICI-associated ophthalmic toxicity and enhance the quality of life of patients, we elaborate on the incidences, manifestations, diagnoses, potential mechanisms, treatments, and management of ophthalmic irAEs based on the current knowledge and relevant literature.
党组织的思想政治工作是党在长期的工作实践中总结出来的重要经验,是发挥党员先锋模范作用,促进企业健康发展等工作的生命线。企业思想政治工作的思路是指企业思想政治工作的指导思想和战略方针。科学发展观是发展中国特色社会主义必须坚持和贯彻的重大战略思想,也是做好新形势下思想政治工作的重要指导思想。近年来,中心党总支通过加强党的理论知识学习与组织建设,进一步夯实党建工作基础,明确党员责任,团队凝聚力得到了增强,员工创造力得到了激发。在广大党员群众的支持下,先后荣获了“上海市工人先锋号”、“上海市电力公司先进基层党组织”等荣誉称号。
POTENTIAL MECHANISM OF OPHTHALMIC TOXICITY
The mechanism of ICI-associated ophthalmic events has yet to be fully understood. The eyes have special mechanismsto limit the invasion of inflammation and infectious agents,thus protecting visual functionAnatomical mechanisms,such as the presence of the blood-retinal barrier and absence of efferent lymphatic vessels, protect the eyes from infection,whereas immune mechanisms, such as the upregulation of the Fas ligand and tumor growth factor-beta (TGF-β), can prevent inflammation by converting T cells into regulatory T cells and causing immune cell death.
Blockade of these regulatory T cells may trigger adverse reactions, and reprogramming of the cell death pathway may lead to ocular adverse events due to ICI therapy. To further downregulate the inflammatory T-cell activity, retinal pigment epithelial cells express both PD-L1 and CD86, which can interact with PD-l and CTLA-4, respectively. High levels of PD-L1 were also found to express in various ocular tissues and may play crucial roles in preventing autoimmunity. In addition, PD-1 and PD-L2 were expressed on tumor cells of ocular adnexal invasive squamous cell carcinomas to varying degrees; as a consequence, these tumor cells can potentially respond to ICI therapy.
IMMUNE CHECKPOINT INHIBITOR-ASSOCIATED OPHTHALMIC ADVERSE EVENTS
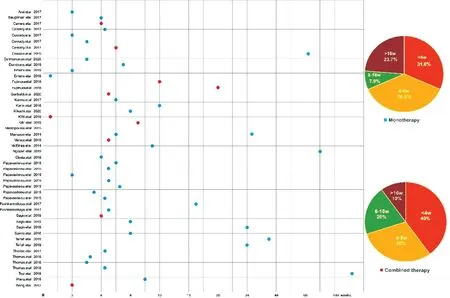
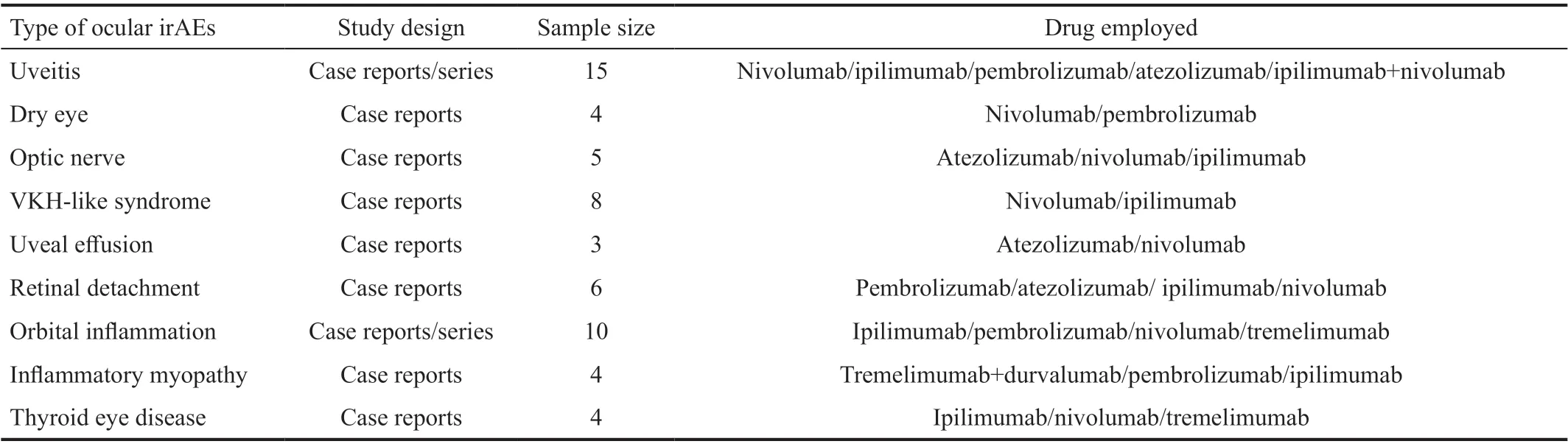
Ocular irAEs can occur at any time during treatment, and even after the cessation of ICIs. However, most (approximately 70%) irAEs typically occur within two months after the initiation of therapy. A minority of irAEs occurs after 48wk,and these irAEs can involve various parts of the eye and orbit. We reviewed published cases of adverse ophthalmic reactions and found that the time to onset of ophthalmic irAEs was earlier when combined with ICIs (either with other ICIs or other conventional therapies; Figure 2). Apart from the variability of the time to onset, there is variability in the ocular symptoms: the most common clinical manifestation of ICIrelated ophthalmic toxicity is dry eyes (3%-24%), uveitis(1%), and myasthenia gravis involved with the eyes (frequency undefined). Other less common ophthalmic adverse events include uveal effusion, retinal detachment, conjunctivitis,ocular myositis, vasculitis, keratitis, episcleritis, vitritis,choroidopathy, and a broad spectrum of neuro-ophthalmic toxicities (Figure 1). Information on various types of ocular adverse events are summarized in Table 2. Most of these adverse reactions can be effectively controlled by periocular,topical, or systemic corticosteroids.
以我国某一农村为例,对农村人畜饮水安全的影响因素进行分析,该地区主要是利用雨水与泉水进行供水,主要水源来自该县的一水库,饮水问题基本得到解决,其水质受人为因素、环境因素、地理位置等影响极易出现污染,水质不能满足国家对生活饮水的安全标准规定,且因使用受污染的水导致许多村民都出现了骨质疏松、粪便呈血、牙齿变黄等症状,严重威胁着村民的身体安全。通过调查发现,该地区的农村人畜饮水安全影响因素主要体现在以下几方面。
通过总结分析,发现单元教学课具有以下特色:1.注重创设问题情境,从生活实际或数学内部提出问题,体现学习新知识的必要性。2.注重抽取分式概念的基本要素,让学生经历分式概念的建构过程,有利于培养学生的数学抽象概括能力。3.注重温故知新,借助类比的方法,构建分式内容的整体框架。4.注重设计各类活动,拓展数学学习方式,展示分式内容的学习成效。5.注重数学思想方法的渗透,依托类比与转化,解决新知识的学习方法问题。6.注重反思与总结,从数学学习的过程与活动中捞足“油水”,积累丰富的学习经验。
Ophthalmic adverse events have been reported most frequently with ipilimumab, followed by nivolumab and pembrolizumab and subsequently by atezolizumab, avelumab, and durvalumab. The incidence of ICI-associated ocular side events is <1%. A total of 15 cases of ocular toxicities were reported in a series of 1474 cases who were treated with nivolumab with or without ipilimumab. A prospective cohort study recently attempted to explore the relationship between ICIs and ocular adverse events in 745 patientsand observed intraocular inflammation in 5 cases, ocular surface disease in 2 cases, and orbital myopathy in 1 case. One study has shown that patients receiving ICIs as therapy who developed colitis were also susceptible to episcleritis or uveitis.
Dry eye disease is a presentation that is characterized by tear hyperosmolarity, tear-film instability,ocular surface inflammation, and damage due to reduced tear quantity and/or quality. Dry eye disease associated with ICIs was the first and the most frequently reported ocular surface adverse event with an incidence ranging from 3% to 24%and presenting with nonspecific eye irritation and as a part of the sicca syndrome. It can also lead to corneal perforation. ICI-related dry eyes can be effectively managed with topical cyclosporine and artificial tears. One patient had nivolumab-associated corneal graft rejection and did not respond well to systemic or subconjunctival corticosteroids.Uveitis refers to the inflammation of the uvea, a highly vascularized layer between the retina and sclera. Among all ophthalmic toxicities, uveitis is one of the most common adverse reactions. It is associated with anti-CTLA-4 and anti-PD-1/PD-L1 agents, such as ipilimumab, durvalumab,avelumab, pembrolizumab, nivolumab, and atezolizumab.
Vogt-Koyanagi-Harada (VKH) disease, known as a bilateral diffuse granulomatous uveitis, is diagnosed in patients who receive anti-PD-1 agents. It presents with blurry vision,xanthopsia, and exudative retinal detachments with bilateral uveitis and is amenable to systemic and occasional topical corticosteroid therapy.
Myasthenia gravis involved with the eye is the most frequently reported adverse event of orbital and ocular adnexa. It can present with blepharoptosis,ocular motility abnormalities, diplopia, or severe systemic symptoms in addition to respiratory distress. These symptoms can be managed with oral/intravenous corticosteroids,intravenous immunoglobulin, pyridostigmine, and plasmapheresis.Severe consequences, such as death from respiratory failure,have also been recorded.
Patients with uveitis irAEs can use periocular, topical, or systemic corticosteroids to control inflammation, and intravitreal corticosteroids can be used for treating macular edema.Some severe cases particularly require the cessation of ICI therapy.
5.药敏纸片试验结果见表2。药敏纸片试验结果表明敏感的药物依次是:头孢菌素、环丙沙星;中度敏感的依次是:青霉素和卡那霉素;而对土霉素、链霉素、庆大霉素具有抗药性。
There is a lack of data for comparing the incidence, pattern,and occurrence time of uveitis induced by CTLA-4 with PD-1/PD-L1 inhibitors. Uveitis irAEs can occur in approximately 1% of patients and manifest as anterior-, posterior-, or pan-uveitis. The time to onset after the initial infusion of ICIs ranges broadly from approximately 2wk to 14mo (median time is 9wk). A typical initial chief complaint is conjunctival redness or bilateral blurred vision. Other symptoms, such as eye pain, photophobia, and floaters are also observed with uveitis. Nevertheless, the mechanisms of uveitis irAEs have yet to be assessed comprehensively.
A significant reduction in the visual acuity associated with a nonpainful redness in both eyes was found in ophthalmologic evaluation. Slit-lamp examination revealed the presence of anterior chamber cells of strong positive, bilateral granulomatous keratic precipitates, bilateral anterior, and posterior synechiae and some pigmentary deposits on the anterior lens capsule that were predominant in the left eye.Fluorescein angiography confirmed unilateral or bilateral papilledema. A light macular edema associated with a subfoveal serous retinal detachment can be revealedOCT.
Thyroid-like orbitopathy, characterized by ophthalmoplegia due to extraocular muscle involvement and proptosis, may occur in patients treated with ipilimumab even in the absence of thyroid dysfunction. It has been suggested that anti-CTLA-4 agents enhance the activation and proliferation of CD8+ T lymphocytes, facilitating the development of Grave's orbitopathy. Anti-CTLA-4 in combination with an anti-PD-L1 inhibitor has also shown to be related to Grave's orbitopathy and an inflammatory myopathy of the diplopia,extraocular muscles, ptosis, and weakness. Moreover,inflammatory orbitopathy, orbital inflammatory syndromes,and orbital apex syndrome have been described in several studies. Systemic corticosteroids can be used to manage these patients.
繁华一瓢饮止:《金粉世家》号称民国红楼,的确是有点红楼的影子。尤其是对女性的塑造都极用心,为整部小说的基调和氛围都增色许多。
Retinal vasculitis resulting in blurry vision secondary to pembrolizumab has been reported in the setting of metastatic cutaneous melanoma to the vitreous cavity. One patient complained of blurred vision and was treated with prednisolone eye drops. Pembrolizumab was continued, and the tumor lesion achieved complete response after 15 cycles of treatment. The ocular presentation improved after external beam radiotherapy and vitrectomy for the vitreous metastases.
Uveal effusion has been reported in patients treated with anti-PD-1/PD-L1 agents, such as pembrolizumab, nivolumab, and atezolizumab. ICI-associated uveal diffusion usually manifests as symptoms, such as redness, blurry vision, ocular, and serous choroidal detachment including the foveal presence of intraretinal and subretinal fluid. Although the uveal effusion can also be attributed to intraocular inflammation, ICI-related uveal effusion can resolve after discontinuing the immunotherapy, indicating that ICIs play an important role in causing uveal effusions.
There are isolated reports of serous retinal detachment with or without choroidopathy, immune retinopathy, exudative retinal detachment with ciliochoroidal effusion, and melanoma-associated retinopathy with atypical chorioretinal lesionsleading to photophobia and blurry vision that have been treated with variable therapies, including topical and oral corticosteroids, discontinuation of ICIs, or observation alone. Early cessation of checkpoint inhibitors has favorable visual acuity outcomes.
Conjunctivitis in patients treated by ICIs is rarely reported, and the incidence and time to onset varies by patient. In one case study, the patient complained of irritated red eyes without the impairment of vision after 13 doses of nivolumab. Conjunctiva swab test was negative,and symptoms were not relieved after antibiotic ocular drop treatment. The ophthalmologist's examination revealed bilateral sterile conjunctivitis with no signs of retinal or uveitis lesions. The manifestation was partially improved after topical steroid therapy. Two cases of conjunctivitis have been reported in a retrospective study, presenting with irritation and conjunctival injection; however, neither required ICI discontinuation. One case improved after treatment with topical corticosteroids.
Ocular myositis was reported in a case with metastatic renal carcinoma. Symptoms such as a subacute presentation of bilateral eyelid ptosis and painless ophthalmoplegia were observed after the second infusion of pembrolizumab. A mild elevation of TSH and CK was found in laboratory tests. A physical examination indicated complete, non-fluctuating, external ophthalmoplegia with bilateral eyelid ptosis. Deltoid muscle biopsy demonstrated mixed macrophagic/lymphocytic endomysial inflammatory infiltration, with prevalent CD68 and CD8 cells, sometimes expressing PD-1/PD-L1 antigens.94 MHC-I overexpression in the cytoplasm and sarcolemma was observed in nonnecrotic cell clusters. In perifascicular regions, CD56+ cells were also observed. After starting corticosteroid therapy and discontinuing pembrolizumab, the patient's symptoms were relieved and the laboratory tests normalized.
从城市土地利用集约程度的角度出发,设计各种情景仿真方案的土地利用面积变化率水平,且设定某类用地面积变化率以其用地转入率和转出率之差为准。情景方案设计结果如表1所示,基准利用方案以SD模型初始模拟结果为主,其余两种情景模拟方案的参数值增减量均是以基准利用方案相关用地面积变量值和《城乡用地分类与规划建设用地标准》(GB50137-2011)中各种人均用地量指标为参照标准进行。
Neuro-ophthalmic adverse events were first reported in a pediatric patient with grade 4 glioblastoma multiforme in 2018. It has also been shown to be associated with ipilimumab, but the incidence is very low. Several cases with neurologic adverse events, including optic neuritis,Grave's orbitopathy, papillitis, and myasthenia gravis have been reported to occur at a median onset of 35d after ICI therapy. Papilledema, multiple cranial neuropathies,and cerebellar ataxia with associated nystagmus have also been observed. The manifestations of neuro-ophthalmic adverse events range from mild to severe and present with visual disturbances, including part or full-field vision loss,disc edema, or scotomas. Prompt recognition, treatment,and management are crucial to prevent morbidity. Most symptoms can be alleviated with corticosteroids, but some severe optic neuropathy requires intravenous immunoglobulin or plasmapheresis. Of note, severe ophthalmoplegia induced by immunotherapy requires early intervention and treatment because of potentially fatal side events.
The granulomatous inflammation of lacrimal glands has been rarely reported. The pathogenesis of granulomatous infiltration in the context of ICIs may be attributed to IL-2 secretion by activated T cells and lymphocytic infiltration with CD8+ T cells. One patient with simultaneous and bilateral keratitis and uveitis in the setting of nivolumab therapy for metastatic melanoma was presented in a case report. The patient presented with bilateral blurred vision after the third dose of nivolumab. Other keratitis types mainly present with corneal haze and pain and can be managed with topical corticosteroids. Episcleritis induced by ipilimumab was also reported in clinical trials; however, details on therapy and outcomes were not given.
DIAGNOSING IMMUNE CHECKPOINT INHIBITORASSOCIATED OPHTHALMIC TOXICITY
Patients with ophthalmic irAEs require thorough ophthalmologic tests that can assess the presence of ophthalmologic, fundus,neurologic, and systemic disease (Figure 3). Ophthalmic evaluation is the most common form of diagnosis; nearly all patients with ICI-associated ophthalmic toxicity were identified in this manner(Figure 3). Patients with ICIrelated ophthalmic toxicity accompanying with fever and flulike symptoms were recommended treatment with antinuclear antibody during the periods of adverse events. Of note,antinuclear antibody usually has good sensitivity but poor specificity for autoimmune disease. The antinuclear antibody evaluation, either using absolute values or changes from baseline, is required to better understand the diagnostic and predictive value in cases with ocular immune-associated adverse reactions.
党的十八大提出,建设“学习型、服务型、创新型马克思主义执政党,确保党始终成为中国特色社会主义事业坚强领导核心”。“三型”党建目标的提出,无论从中国社会转型时期的现实需要来看,还是从马克思主义政党观来看,都是具有重大意义的党建目标定位[2]。我党不只是当代中国的执政党,更是社会的建设党,必须让广大党员干部明白党的实质与党群的血肉关系,才能让我党成为“三型”马克思主义政党。
The examination of neuro-ophthalmic events may be accompanied by a series of imaging studies and ancillary laboratories based on medical history and examination findings, including infectious and autoimmune serologies,MRI, optical coherence tomography (OCT), and cerebrospinal fluid (CSF) examination. Orbital and cerebral MRI may provide ophthalmologist with valuable diagnostic and prognostic information.
ICI-associated inflammatory orbitopathy is an orbital adverse effect that presents with proptosis, pain, eyelid edema,chemosis, and extraocular motility restriction. One case of orbital myopathy that involved the extraocular muscles was associated with blepharoptosis and dyspnea and required tremelimumab and durvalumab discontinuation and the use of systemic corticosteroids.
A wide spectrum of ocular manifestations should be included in the differential diagnosis by ophthalmologists to prevent irreversible vision loss and mortality. It is worth mentioning that melanoma-associated retinopathy, a rare autoimmune disease, has been shown to be associated with the diagnosis of cutaneous melanoma. It is characterized by various optic disc findings and the presence of antiretinal antibodies. Melanoma-associated retinopathy presents with several forms of chronic visual impairments, which usually develop several months after the diagnosis of melanoma.Melanoma-associated retinopathy occurs with the melanoma diagnosis, regardless of the therapy, and is therefore easily distinguished from ICI-associated ocular toxicity.
TREATMENT AND OUTCOME OF ICI-ASSOCIATED OPHTHALMIC ENVENTS
The treatment regimens for ophthalmic irAEs vary depending on the case. Recently, detailed recommendations for the treatment of ICI-induced ophthalmic adverse events have been proposed. For patients with moderate adverse events (CTCAE grade 2, such as those involving the anterior segment), ICIs should be suspended until the symptoms reduce to grade 1 or normalize; corticosteroids may be administered. For patients with severe adverse events (grade 3 or 4, such as those involving the posterior segment), systemic corticosteroids should be administered. Large doses and long periods of corticosteroids should be avoided because of multiple adverse events that result from it.
In addition to being considered as a drug-associated toxicity,some ophthalmic toxicities, such as uveitis, may serve as a prognostic marker of response to ICIs. Attiareported a series of 56 metastatic melanoma patients treated with ipilimumab and found that autoimmunity correlated with the regression of tumor. Among those with severe irAEs, 36% had objective tumor regression compared with 5% of those without irAEs. There was also a report in which one patient developed severe ophthalmic adverse event during treatment with ipilimumab; however, the patient sustained tumor remission.Of the 15 reviewed cases, tumor regression upon manifestation of uveitis was described in 7 cases in which either a complete or partial response was obtained. There was a report of a case who was treated with pembrolizumab and soon developed symptoms, including blurred vision, hearing loss, and acute onset ataxia. Simultaneously, a robust regression of metastases was also detected. Some severe adverse events of panuveitis, such as a VVKH syndrome induced by ipilimumab,requiring high-dose oral corticosteroids have also been reported. The sequential administration of nivolumabassociated VKH disease has been reported with a positive clinical outcome.
The above evidence suggested that ICI-associated ophthalmic toxicity may be a potential marker for tumor response. As a result, the administration of corticosteroids requires careful consideration, because of possible compromise of antitumor activities of ICIs. Of note, some patients can also achieve a significant reduction of tumor burden through the symptomatic treatment for ocular adverse effects.
POSSIBLE MANAGEMENT OF OPHTHALMIC ENVENTS AND FUTURE DIRECTIONS
Effective communication with a multidisciplinary team and primary care provider is essential for the prompt recognition and management of ICI-related ophthalmic events. In the era of anticancer immunotherapies, first, it is of great importance for clinicians to distinguish ICI-related events from potential autoimmune-associated causes and common toxic adverse events. Second, it is vital that ophthalmologists do not mistake uveitis-like manifestations as purely inflammatory. The eye is an immune-privileged organ; even in the setting of an otherwise complete systemic response to therapy, it may be vulnerable to metastases. Two published case reports described cutaneous melanoma metastatic to the vitreous cavity and retina in patients treated with ICIs. These studies elucidated how such manifestations can be confused with inflammatory uveitis but require different management and may have an important impact on prognosis. Third, in the context of a diagnostic dilemma, eliciting a history of systemic irAEs and understanding ophthalmic irAEs that are rarely isolated are critical.
In general, most ophthalmic toxicities can initially be managed by periocular, topical, or systemic corticosteroids. In practice,when the ocular inflammation is mild or only covers the anterior segment, ICI discontinuation might not be required.Of course, the evaluation for the cessation or discontinuation of treatment will vary on a case-by-case basis depending on the severity and availability of ophthalmologic treatment. In severe or steroid-refractory cases, in which the symptoms are debilitating, it is necessary for ophthalmologists to consult with oncologists in determining the benefits and risk of cessation or continuation of ICIs. Immunotherapy discontinuation resulting in the spontaneous resolution of symptoms has rarely been reported. Steroids are required for most patients to alleviate the duration and intensity of symptoms.Alternative immunomodulatory therapies, such as intravenous immunoglobulin or plasma exchange, may offer additional benefits for patients with severe ophthalmologic events.
李劼人笔下的女性虽然独立自主,在那个仍然封建落后的社会环境下和三从四德的传统女性相比具有超前性和先锋性,但是她们仍然在男权主义下苦苦挣扎生存。他们并没有完全摆脱男性的压迫和摧残,她们虽然有一定的独立自主意识,但是她们仍然摆脱男性而独立生存。她们渴望浮出水面,却只能在呼吸和窒息中挣扎。
It is controversial whether ICIs should be re-introduced after recovery from ophthalmic toxicity. Although ophthalmic dysfunction can be significantly improved by corticosteroid therapy, an anti-PD1 agent re-challenge might induce symptom recurrence and even aggravate immune-related toxicities. In particular, the re-challenge of ICIs after a grade 3 toxicity requires extreme precaution. These recommendations may include some specific genres, such as uveitis, episcleritis, and blepharitis, but do not address other possible ocular presentations. It is important to be aware of the recurrence of adverse events after the re-introduction of ICIs. The management of the recurrence of ophthalmic toxicity is also challenging. As a result, the collaboration of clinical oncologists and ophthalmologists should give careful consideration to patients according to their presentations,outcomes, and alternative cancer therapy options to weigh the pros and cons of reintroducing immunotherapy.
随着我国加入WTO,中国将会成为世界烟叶生产和消费的中心,但是我国烟叶的生产和质量水平与世界烟草大国相比还有相当大的差距。烟叶生产环节多,技术要求高,烟农零星分散种植,不利于生产水平和烟叶质量的提高。美国、巴西、津巴布韦等烟叶生产大国早在20世纪90年代末就全部采取了农场化种植、机械化操作、企业化管理的经营模式,烟叶生产的各环节都采取了机械化作业的模式,降低了生产成本,提高了烤烟生产的科技含量,烟叶产量、质量和效益较好,市场竞争力强。目前,发展适度规模种植,进行机械化作业、规范化管理已经成为烤烟生产适应国内、国际市场形势,提高生产水平和烟叶质量的发展方向。
CONCLUSION
ICIs, either alone or in combination with other therapies, can lead to ophthalmic adverse reactions, such as dry eyes, uveitis,ocular myasthenia gravis, uveal effusion, retinal detachment,conjunctivitis, ocular myositis, vasculitis, keratitis, episcleritis,and a wide spectrum of neuro-ophthalmic toxicities. Of all ICI-related ophthalmic events, dry eyes and uveitis are the most common ophthalmic adverse reactions. Although the incidence of ophthalmic toxicities induced by ICIs remains relatively low, oncologists and ophthalmologists must be vigilant for these adverse reactions because permanent damage and blindness can result from neglect. The time to onset and clinical presentations of ophthalmic irAEs are variable. They can occur at any time during treatment, including after the cessation of ICIs with nonspecific symptoms ranging from blurred vision, painless ophthalmoplegia, diplopia, eyelid swelling, eye redness, floaters, exophthalmos, vision loss to shaped scotoma, headaches, and auditory changes. The assessment of ophthalmic evaluation in combination with autoimmune serologies, OCT, CSF, fundus examination, slitlamp examination, fluorescein angiography, MRI, and biopsy,if necessary, contribute to the diagnosis of ICI-related ophthalmic adverse reactions. Among these diagnostic methods,ophthalmic evaluation is easily performed and has widespread availability. Before the initiation of ICIs, a comprehensive assessment of ophthalmic risk factors and a detailed ophthalmic history should be obtained, particularly for patients with autoimmune disease or pre-existing ophthalmic disease and in the context of ICIs combined with other regimens. For patients with confirmed ophthalmic events, most ophthalmic toxicities can initially be managed by periocular, topical or systemic corticosteroids. In severe or steroid-refractory cases,alternative immunomodulatory therapies, such as intravenous immunoglobulin or plasma exchange, might offer additional benefits. Ophthalmologists need to discuss with oncologists to determine the benefits and risks of discontinuing ICIs. Of note,ICI-associated ophthalmic events may be a potential positive marker for tumor response. In addition, ophthalmic function re-assessments and frequent monitoring are necessary. To better understand these events and provide effective therapy strategies, larger studies are needed.
None;None;None;None;None;None.
猜你喜欢
杂志排行
International Journal of Ophthalmology的其它文章
- Leptin activates the JAK/STAT pathway to promote angiogenesis in RF/6A cells in vitro
- CCPG1 involved in corneal Aspergillus fumigatus infection
- Anti-scarring effect of sodium hyaluronate at filtration pathway after filtering surgery in rabbits
- Five-in-one: a novel, cost-effective yet simple use of micro needle holder
- CO2 laser-assisted sclerectomy surgery and trabeculectomy combination therapy in Peters’ anomalyrelated glaucoma: a case report
- Congenital fibrovascular pupillary membranes: case series with pathological correlation and surgical treatment