Y-splitting medial rectus muscle and recession in treatment for convergence excess esotropia
2022-04-19LiJuanHuangYuYuWuNingDongLi
INTRODUCTION
A fornix incision was performed at the inferonasal region of the operated eye under general anesthesia.After being exposed and hooked, the MR muscle was split longitudinally from its insertion to the location of 15 mm posterior to the insertion into two equal halves with a small hook (Figure 1A). Each half of MR was sutured separately at the 1 mm posterior to the insertion with locking bites using a double armed, 6-0 Vicryl suture, and then severed from the insertions. The two separated MR bundles were recessed and reattached to the globe in a Y-shape with one-tendon-width apart (Figure 1B). The amount of recession was calculated by the deviation angle at distance. Surgical success was defined as a horizontal deviation of <8 PD at near and distance at primary gaze position. Overcorrection was defined as exotropia of ≥10 PD at distance, and undercorrection was defined as esotropia of ≥10 PD. The follow-up was scheduled postoperatively at 1d, 1wk, 1, 3, and 6mo.
Optical correction with bifocal lens is useful for those patients who have orthophoria or esophoria at distance, and esotropia at near due to high AC/A ratio, but not useful for those patients with normal or lower AC/A. If the patients have an esodeviation angle of more than 8 PD at distance under completely optical correction, they usually cannot compensate their esotropia by fusion, so that they have to accept surgical treatment for their esotropia.
Although some surgical techniques have been reported for CEET treatment, it is still a tough issue for many surgeons to treat this type of esotropia due to the difference between the esodeviation angles at near and distance. Here, we evaluate the effectiveness of bilateral medial rectus (MR) recession and Y-splitting in surgical treatment of CEET. The technique of muscle Y-splitting has been proved to be effective in reducing the muscle torque and changing the muscle contraction in the secondary gaze positon, so that it can be used in resolving excessive adduction when convergence at near.
SUBJECTS AND METHODS
Pre- and postoperative evaluations were performed for general ocular conditions(best corrected visual acuity, anterior segment and fundus),ocular movement at nine cardinal gaze positions, ocular misalignments and binocular status. Patients younger than 14y had cycloplegic refraction and those older than 14y had refraction without cycloplegia. The prism and alternate cover test was used to measure the deviation angles at near (33 cm)and distance (6 m) under the conditions of with and without the corrective lens. The AC/A ratio was assessed using the gradient method. The formula was AC/A= (PD-PD)/3 D.PDis the deviation angle measured by the prism and alternate cover test looking at a target at 5 m, while PDis the deviation angle measured with a -3 D lens added to the eye. Binocular sensory status was evaluated with the Bagolini striated glasses at near and distance, and by stereoacuity assessment at near using the Titmus test (Stereo Optical Co., Inc., Chicago, IL,USA).
Medical records were retrospectively reviewed for six patients with CEET who underwent strabismus surgery by the authors from January 2018 to December 2020.
The surgical approach of Y-splitting MR and recession is effective in treatment of CEET.
Written informed consent was obtained from the patients or the patient's guardian preoperatively.All protocols adhered to the principles of the Declaration of Helsinki.
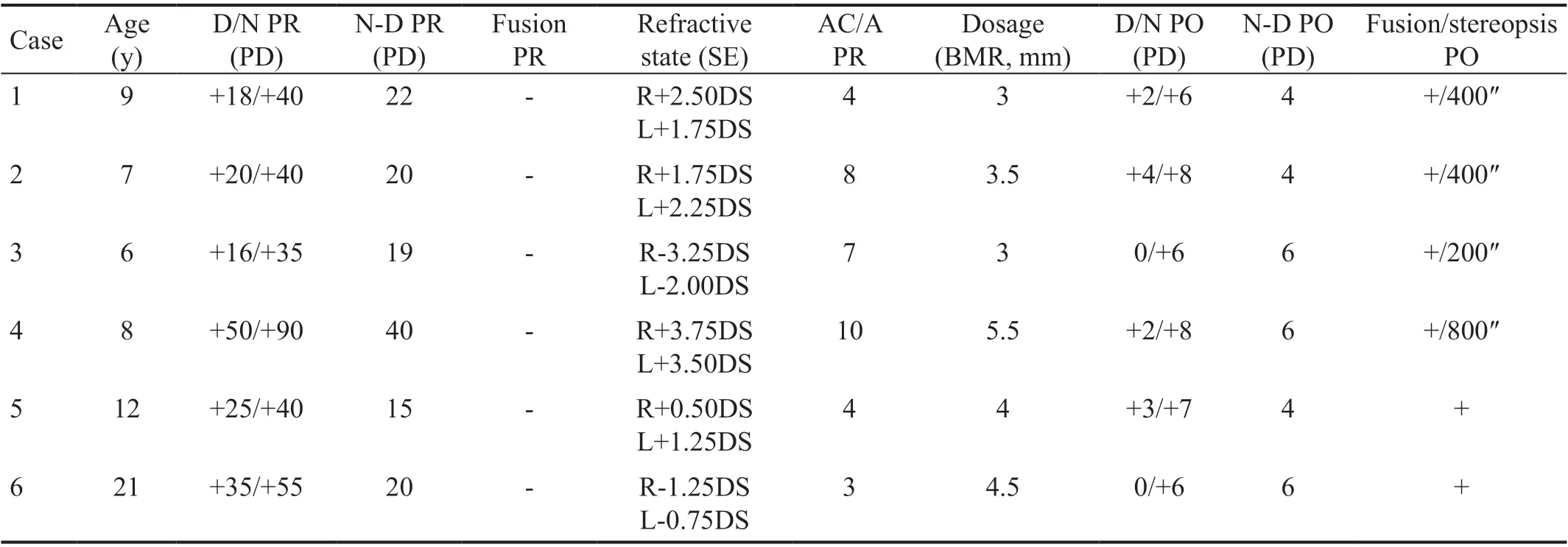
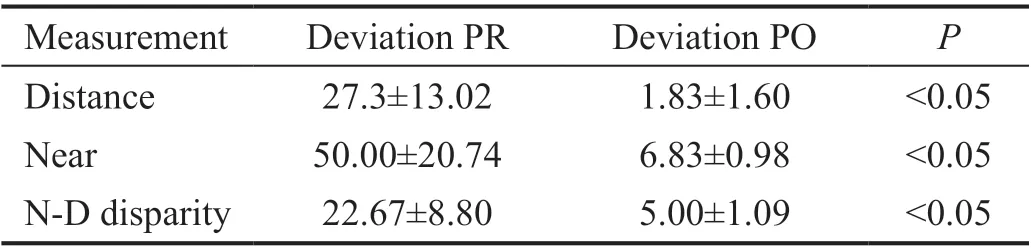
All six patients with CEET had undergone bilateral MR recession with Y-splitting procedure. The mean esodeviation at the primary position was 27.3±13.02 PD preoperatively and 1.83±1.60 PD postoperatively at distance (<0.05). The mean esodeviation at near was 50.00±20.74 PD preoperatively and 6.83±0.98 PD postoperatively (<0.05). The mean neardistance disparity was significantly reduced from 22.67±8.80 PD preoperatively to 5.00±1.09 PD postoperatively (<0.05;Tables 1 and 2). Patients had achieved satisfactory surgical outcomes showing a good ocular alignment at near and distance without limitation on any gaze positions (Figure 2).In addition, their sensory status had been improved because patients who didn't have binocular vision had acquired near stereopsis or binocular vision postoperatively.
Convergence excess esotropia (CEET) refers to an esodeviation angle at least 15 prism diopters (PD) larger at near than at distance under the fully optically correction of refractive error. Patients with CEET may have a high or a normal accommodative convergence to accommodation(AC/A) ratio, with a refractive status of hyperopia, emmetropia,or even myopia.
As mentioned above, surgical treatment for CEET is a tough issue for many doctors due to the distance-near disparity of esodeviation. If the surgical dosage was calculated based on the deviation angle at near, overcorrection would occur at distance. On the other hand, if the surgical dosage was calculated based on the deviation angle at distance,postoperative under-correction would be present, and thus patients would have to wear bifocal lens to correct residual esotropia at near postoperatively. However, for those patients with normal and low AC/A or myopia, bifocal lens could be useless for correction of esotropia at near.
The paired-test was used to compare the mean deviation angles at near and distance, as well as the mean difference between the near and distance deviations preand post-operatively. SPSS version 22.0 for Windows (SPSS,Chicago, IL, USA) was used for statistical analysis. Avalue of <0.05 was considered statistically significant.
3) 当故障判断完成后,要确认故障诊断的结果。若诊断错误,需要输入人工诊断结果,若正常则读取下一组数据继续测试,若诊断出故障则将在线数据处理后加入相应的故障抗体库进行更新,对于新故障还将引入新的抗体类别。
RESULTS


大区域范围路网评价方面,基于严重拥堵比例的方法较基于行程时间比的方法对高峰道路拥堵变化更敏感,其原因是重点刻画了道路出行拥堵所占的比例[11-13],而行程时间比的方法则计算了全部样本,属于均值类方法,评价范围越大,平滑的效果越明显. 图1对比了基于两种模型计算北京市中心城区周一和周五工作日的交通指数,严重拥堵里程比例方法更体现出周一早高峰通勤拥堵以及周五晚高峰交通拥堵特性. 在评价大范围路网区域时,应优先选用严重拥堵里程比例方法.
DISCUSSION
实验结果中,计量资料数据采用±s表示,用SPSS 17.0软件进行分析,采用单因素方差分析(ANOVA),组间比较采用t检验;计数资料数据(HE染色实验结果)采用Ridit检验分析。以P<0.05为有统计学差异。
A series of surgical procedures have been designed to decrease the distance-near disparity in CEET, including posterior fixation with sutures on the belly or on the pulley of MR,as well as slanted recession of the MR, Scott's procedure(simultaneous resection and recession on MR), as well as Y-splitting of MR with recession.
Posterior fixations with sutures on the belly of muscle, also named as Faden procedure, can reduce effectively the muscle torque at its field of action without disturbance of the primary gaze position, and has been used for the surgical management for CEET because this procedure may produce a restrictive action on the overactive MR at the second gaze position.However, the main challenge for many doctors is the surgical technique on performing a retro-equatorial suture fixation at the sclera, which in turn would increase the risk of sclera perforation. An alternative approach of Faden procedure is posterior fixation of the muscle pulley with MR recession,however, we don't have sufficient experience in this procedure.Recently, extraocular muscles have been proved to be compartmentalized by their function. The superior and MR compartment had different contractility in conjugate adduction in similar-magnitude convergence. Taking advantage of the functional difference in the compartments of extraocular muscle, the surgical approaches of slanted recession or slanted resection to weaken or strengthen the corresponding muscle compartments are used to surgical managements for convergence insufficiency exotropia, A-V pattern, as well as CEET in which the lower two-thirds compartments would be recessed farther than the upper one-thirds compartment of MR. The recessed amount of lower compartments is calculated according to the deviation angle at near, while the surgical amount for the recessed upper compartment is calculated on the deviation angle at distance. In our own experience, this surgical approach works very well when the deviation angle is less than 50 PD at distance and the distancenear disparity under 25 PD. If more than these parameters,for example, case 4 in the Table 1, recession of MR would be augmented or resection of later rectus is needed. In addition,the lower compartment of MR is needed to be recessed far more distance than the upper compartment to correct a larger near-distance disparity, which is not easy to operate on a whole muscle rather than on a split muscle.
Scott procedure has the same effect as Faden procedure through simultaneous resection and recession on MR in which the amount of recession is equal to the amount of resection of extraocular muscle, or a bit larger than that of resection.We think this procedure would benefit for correction of CEET with orthotropia or a small angle of esodeviation. However,for CEET with a moderate or a larger angle of esodeviation,an additional MR recession is needed to counteract the effect caused by MR resection, which could result in limitation on adduction due to large amount of recession.
Y-splitting recession as a secondary and/or unilateral surgery for distance/near esotropia can reduce distance/near disparity. Recently, the surgical approach of Y-splitting MR and recession has been proven to be powerful for CEET treatment because of the combined effects of muscle recession and splitting. Recession of muscle may decrease the muscle force while Y-splitting may reduce muscle torque similar to the Faden procedure, and they work together to decrease the esotropia and the distance-near disparity. The effectiveness of this procedure is further supported in this study by the satisfactory surgical outcomes from our patients. We agree to that separation of one-muscle width is enough for two halves of MR instead of separating them far away from other each. We feel that the method used by Hoerantneris too complicated in measuring the locations of insertions for two separated MR bundles. The surgical dosage described by Hoerantner. In their method, the amount of recession was on the average of 2.6±0.6 mm. The arms of two separated half muscle were 15 mm longer with an angle of 62.8±5.7 degrees. The rotating torque was able to be changed significantly by the 15 mm length separation of extraocular muscles through mathematical calculation. Although we didn't calculate the angle of two separated muscle, we think onetendon-width separation is more easily determined. However,we agree to their opinion that that the splitting distance should be 15 mm or more, so that the muscle torque could be effectively reduced when combination with MR recession. In addition, Bagherithink that two unequal separated arms of MR may produce vertical or torsional deviations. We think their opinion should be confirmed further because a lot of patients with esotropia don't have a good binocular status and are not able to detect torsional deviation even though they have torsion in their fundi. Anyway, we think that MR splitting and recession is a safe and powerful approach in surgical correction of CEET, and easily learned.
Supported by the National Natural Science Foundation of China (No.81670883).
在缺陷分析中可以使用统计方法对收集的缺陷进行分类、汇总。基于不同的缺陷属性,根据需要统计缺陷分布情况,利用统计结果分析缺陷产生的根本原因,将其成为改进软件测评过程的依据。缺陷统计内容包括:
None;None;None.
猜你喜欢
杂志排行
International Journal of Ophthalmology的其它文章
- Leptin activates the JAK/STAT pathway to promote angiogenesis in RF/6A cells in vitro
- CCPG1 involved in corneal Aspergillus fumigatus infection
- Anti-scarring effect of sodium hyaluronate at filtration pathway after filtering surgery in rabbits
- Five-in-one: a novel, cost-effective yet simple use of micro needle holder
- CO2 laser-assisted sclerectomy surgery and trabeculectomy combination therapy in Peters’ anomalyrelated glaucoma: a case report
- Congenital fibrovascular pupillary membranes: case series with pathological correlation and surgical treatment