Clinical characteristics and surgical treatment of idiopathic uveal effusion syndrome
2022-04-19ZhiJunShenLinShenHongWang
INTRODUCTION
Uveal effusion refers to the leakage of fluid from the choriocapillaris, and may cause exudative detachment of the choroid and retina without retinal breaks. Uveal effusion may be idiopathic or secondary to choroidal tumors,extensive chorioretinitis, and surgery, among others.Macular involvement in exudative retinal detachment leads to significant visual acuity impairment.
The term “uveal effusion syndrome” (UES) was first introduced by Schepens and Brockhurstin 1963; the disease is diagnosed by exclusion when the other causes of uveal effusion have been ruled out. UES is generally divided into nanophthalmic UES and idiopathic UES (IUES). Nanophthalmic UES is easily diagnosed because of the characteristic clinical manifestation,short eyeball axis; IUES is rarely reported in clinical practice and may be misdiagnosed as another exudative choroidal or retinal detachment disease. The causes of IUES remain unknown, and the disease predominantly occurs in otherwise healthy middle-aged people. Gass and Jallowhypothesized that UES is primarily caused by congenital scleral abnormalities that act as barriers to the transscleral outflow of protein from the suprachoroidal space,and secondarily predisposes one to vortex vein obstruction.According to this theory, Gassproposed a surgical management method for the treatment of UES using scleral sclerectomy and sclerostomy; subsequent studies further confirmed the effectiveness of these surgical modalities.In this study, we reviewed the records of patients with an IUES diagnosis treated using surgery, in the past ten years, and analyzed the clinical features and surgical outcomes associated with the disease.
SUBJECTS AND METHODS
This study was approved by Beijing Tongren Hospital Ethical Committee and informed consent was signed by all participants before surgery.
Ophthalmic ultrasound and UBM,among others, can be helpful in the diagnosis of IUES.Sclerectomy and sclerostomy are surgical modalities that can successfully treat the disease. Some patients may experience recurrence after surgery; reoperation remains safe and effective for them. Long-term follow-up is essential in such settings.
All patients underwent routine eye examinations, including binocular indirect ophthalmoscopy, ultrasound examination,optical coherence tomography (OCT), and ultrasound biomicroscopy (UBM), and some underwent fluorescein angiography and indocyanine green angiography. A small number of patients did not undergo angiography examinations due to allergies or poor general conditions. Patients were tested for syphilis, human immunodeficiency virus infection and hepatitis B and C infection and underwent routine blood and urine examinations. The exclusion criteria were as follows:the presence of a short eye axis (eye axis <20.5 mm); uveitis;panretinal photocoagulation; intraocular surgery; trauma,and a known cause of ciliochoroidal effusion. Patients with rhegmatogenous retinal detachment and choroidal detachment as a complication were also excluded.
(3) 当逆作法施工采用盆式开挖法挖土时,最大位移出现在地下连续墙墙顶处,此时应在确保将墙顶位移控制在合理范围的前提下,基于首层土的开挖深度,确定盆式挖土预留土体的经济宽度。针对逆作法盆式开挖不同坡肩宽度下地下连续墙的位移变化情况,采用有限元法进行了研究。以往的工程经验表明,当软土区首层土盆式开挖深度取6.5 m、坡肩宽度取6.0 m时,即可实现将地下连续墙的变形控制在合理范围内的目的。
The causes of UES remain unknown. In 1983, Gasshypothesized that the initial cause of UES is congenital scleral dysplasia, which acts as a barrier leading to the obstruction of the transscleral flow of the suprachoroidal protein and secondary venous occlusion. Retinal detachment and choroidal detachment are resolved by sclerectomy,indirectly confirming that scleral dysplasia causes UES.In 2011, a study that used enhanced depth imaging spectral domain OCT found that the thickness of the choroid was significantly increased in patients with IUES, adding to the theory of Gass pertaining to the scleral barrier to transscleral flow in the disease. In our study, we observed abnormal scleral thickness values on surgery, as well as irregular collagen fiber arrangement and abnormal deposition,indicating the presence of proteoglycans-like in the scleral matrix, as observed on pathological and electro-microscopic examination, further confirming Gass' hypothesis. Previous studies have shown the presence of a complex relationship between collagen fibrils and proteoglycans in the extracellular matrix, leading to transscleral fluid outflow obstruction through these scleral abnormalities. The obstruction of transscleral outflow caused by abnormal sclera first leads to ciliochoroidal detachment; during this period, patients have no clinical symptoms. Our study confirmed, using UBM,that all the participants had binocular leakage and ciliary body detachment.
RESULTS
The baseline characteristics of the 26 patients included in this study are summarized in Table 1. Seventeen (65.4%) of the 26 patients were men, and 9 (34.6%) were women. None of the patients had a family history of the disease. The average age of symptom onset was 46.8y (22-64y). Of the 26 patients,7 (26.9%) had binocular retinal detachment at presentation.The mean duration from symptom onset to surgery was 8.5mo. Three eyes underwent reoperation for recurrent retinal detachment. The time to recurrence in these three eyes was 1,5, and 9y, after surgery, respectively.
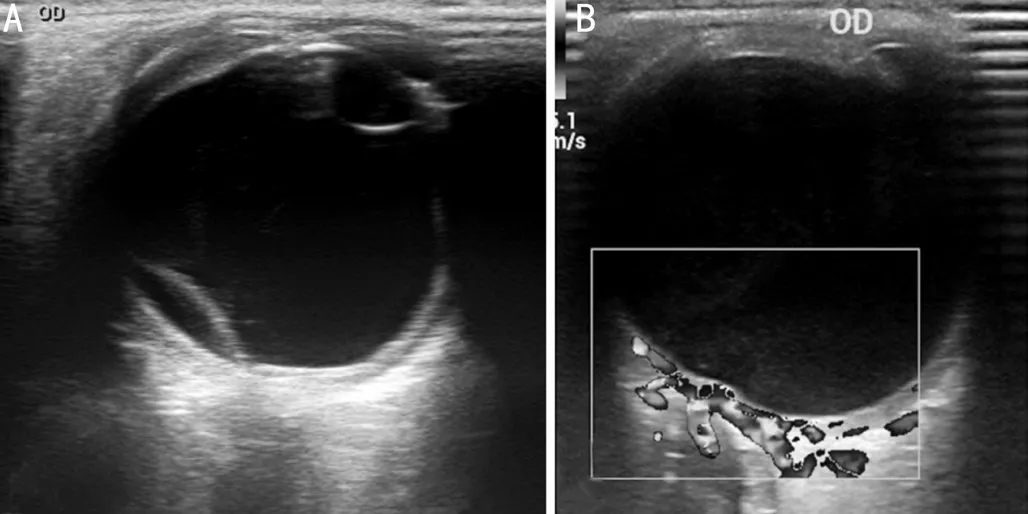
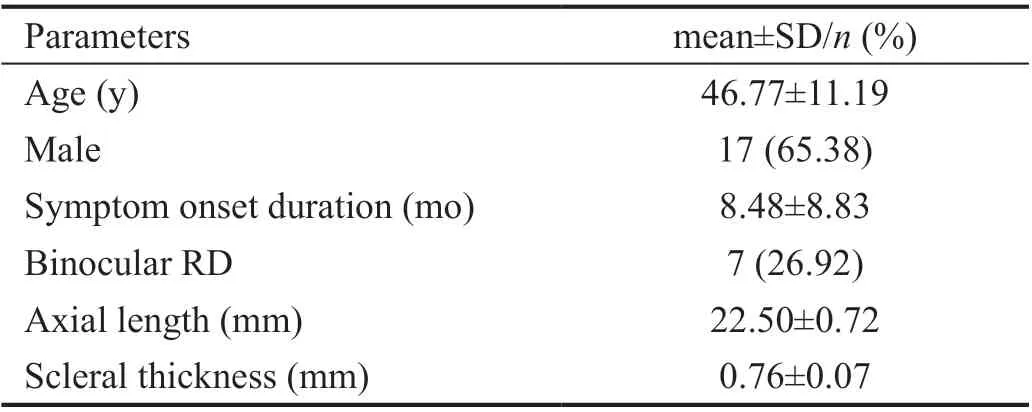
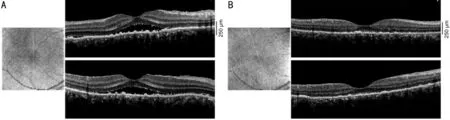
Ultrasound examination of the eyes showed that 24 patients had monocular or binocular retinal detachment (Figure 1A).OCT examination showed only macular exudative retinal detachment in two eyes of two patients (Figure 2A). UBM showed effusion of the ciliary body in the binocular eyes among all patients (Figures 3A-3D). Surgery was performed on the eyes showing retinal detachment, including two in which the subretinal fluid was only confined to the macular region, simulating idiopathic central serous chorioretinopathy.The axial length of the surgical eyeballs ranged from 20.9 to 23.7 mm (average 22.5 mm). The thickness of the sclera near the temporal scleral process was examined by UBM and was found to be an average of 0.76 mm. Fluorescence angiography showed mottled high and low fluorescence in the fundus,which was a leopard-like change.
The average preoperative intraocular pressure (IOP) was 14.8(9-27) mm Hg, and the postoperative IOP (the first day after surgery) averaged 13.9 (7-24) mm Hg.
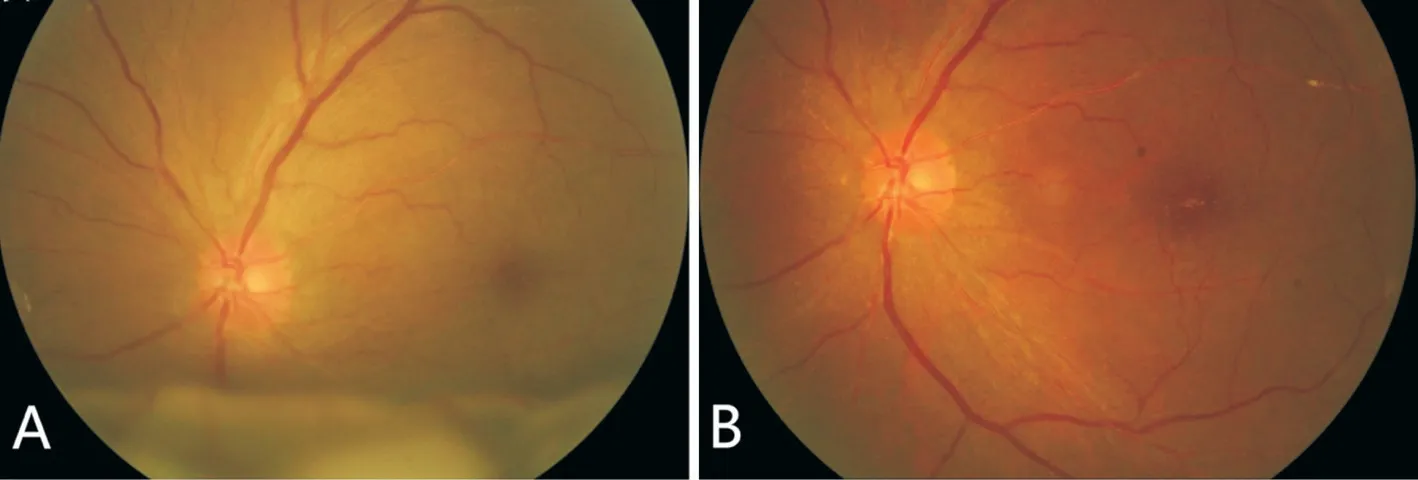
Surgery was performed on all 33 eyes with retinal detachment.Retinal detachment was characterized by exudative retinal detachment and subretinal fluid shifts with changes in the eye or head position; no break or tear was seen on fundus examination, and no viable proliferations were observed in the vitreous (Figure 4A). Macular retinal detachment was predominantly characterized by neuroepithelial detachment,and more often accompanied by retinal retinoschisis.
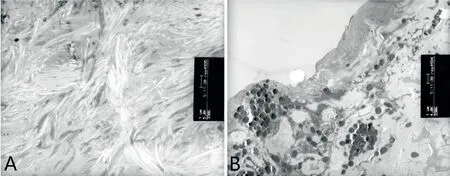
During the surgery, we observed the spontaneous release of a pale-yellow suprachoroidal effusion fluid as the choroid was exposed. However, the choroidal effusion fluid was intentionally not drained out. The sclera was abnormally rigid and thick, and scleral texture disorder was noted; therefore, the razor blade knife had to be changed frequently. No complications occurred during the surgery. Pathological examination of the surgically excised scleral slice confirmed the presence of scleral collagen fiber arrangement disorder. Electron microscopy of the scleral slice also showed an irregular scleral fiber arrangement and marked deposits of matrix between the fiber bundles (Figure 5).
Three patients with recurrent retinal detachment underwent a second surgery—four-quadrant lamellar sclerectomy—combined with partial full-thickness sclerostomy. The scar tissue was removed during surgery and abnormal scleral thickness was observed again. Retinal detachment was resolved within 4mo after the second surgery.
All patients were followed-up for at least 6mo after surgery.Retinal detachment was gradually resolved from 1wk to 5mo after surgery (Figures 2B and 4B). Pigmentation was observed in the retinal detachment zone. Choroidal detachment resolution was achieved earlier than retinal detachment resolution (Figure 1B), and ciliary body effusion was gradually resolved (Figures 3E-3H). The visual acuity of 30 eyes increased to varying degrees, and there was no significant change in the visual acuity in three eyes.
DISCUSSION
In this study, we only reviewed the clinical data of hospitalized patients who undergone surgery in the past ten years. Some outpatients who were relieved by medical treatment were not included in the analysis. We found that ophthalmic ultrasound and UBM, among others, aided the diagnosis of IUES.Sclerectomy and sclerostomy were associated with treatment success. However, some patients experienced recurrence after surgery; they underwent successful reoperation.
高校学生管理是一项较为复杂的工作,管理者要顺应时代的发展趋势,坚持以人为本,与时俱进。人本理念在高校学生管理中的运用,最根本的是要解决观念问题,正确指导学生进行管理体制和方法的创新,要对理论知识进行深入的研讨,还要在实践中不断的完善管理经验,让学生们转变思想观念,强化服务意识,逐步实现民主交流、平等沟通、和谐统一的校园生活环境。
UES was first reported in 1963 by Schepens and Brockhurst;however, only a few cases of the disease have been reported to date. The incidence of IUES is even lower in the existing literature. To the best of our knowledge, the current study, which included 33 eyes from 26 patients, presents the largest number of IUES cases to date. We reviewed the records of IUES patients with an axial surgical eyeball length of≥20.5 mm, consistent with the criteria employed by Johnson and Gass.
Uyamaclassified 19 eyes from 16 patients with IUES into three groups: type 1 included nanophthalmic eyes with an axial eyeball length shorter than 19.0 mm; type 2 included nonnanophthalmic eyes with a rigid and thick sclera and an axial length averaging 21.0 mm; type 3 included non-nanophthalmic eyes with a normal size and scleral thickness and an axial eyeball length ranging from 25.0 to 22.9 mm. They concluded that sclerectomy was effective in types 1 and 2 only; in type 3 eyes, this treatment modality was ineffective. However, in the type 3 group, only two eyes from two patients were treated.Johnson and Gassinvestigated 23 eyes of 20 patients with IUES who underwent quadrantic partial-thickness sclerectomy with an axial length of ≥20.5 mm (average 23.1 mm),and found that subretinal and/or supraciliochoroidal fluid resolution occurred within 6mo in 19 eyes (83%) after one procedure and in 22 eyes (96%) after one or two procedures.
All patients underwent four-quadrant lamellar sclerectomy combined with partial full-thickness sclerostomy. The extent of each quadrant slice was 5×7 mm, about half to twothirds of the scleral thickness. A 1×2 mmsclerostomy was made in the center of each sclerectomy site. All the excised scleral pieces underwent pathological examination. The pieces obtained from one patient underwent electron microscopy.
颗粒复合肥按国标生产,一般只含氮磷钾,养分不平衡。在生产方面,液体肥同样具有优势,液体复混肥生产过程无污染,无排放,更加环保和节能;颗粒复合肥生产过程是能耗过程,存在污染和排放。
总之,加强企业青年人才队伍建设,更好地发挥青年人才在企业生产建设中的主力军作用,是提升企业基层工作水平的关键所在。应把培养造就青年人才作为企业人才队伍建设的一项重要战略任务,开展青年人才职业生涯规划,开展青年人才责任教育,加强青年人才管理制度建设,加大青年人才选任力度,采取及早选苗、重点扶持、跟踪培养等特殊措施,使大批青年人才持续不断涌现出来。为不断提升基层工作水平,推动企业和谐、健康发展,实现“打造世界一流,实现率先发展”目标,提供坚实的人才保障。
In some patients, the degree of UES may show spontaneous improvement; however, the disease course is long and may result in serious visual acuity damage. In previous reports,including 20 patients with a natural disease course and a follow-up period of up to 8y, 9 patients showed spontaneous choroidal reattachment within 4mo to 6y, while the remaining 11 did not show improvements at the end of the observation period. Therefore, timely surgery is required for IUES patients with retinal detachment.
Inconsistent with the findings of previous research, our study found that the sclera of IUES patients with an axis greater than 20.5 mm is still thickened, and the blade needs to be replaced repeatedly during surgery. Ultrasound examination could not accurately measure scleral thickness. While we attempted to measure the thickness of the sclera near the scleral process by UBM, we did not measure the normal scleral thickness using the same method. We found that the mean thickness of the sclera near the scleral process was 0.76 mm by UBM. A previous study showed that UBM may be a more accurate and precise method for the measurement of scleral thickness than magnetic resonance imaging; the study found mean thicknesses values of 0.65±0.08 and 0.55±0.05 mm for eyes with UES and control eyes, respectively, by UBM.
Other clinical features observed in our patients were: a predominance of young and middle-aged patients; male predominance; chronic disease course; asymptomatic initial stage; normal intraocular pressure, slightly higher intraocular pressure in some cases; and absence of inflammatory reaction in the anterior segment and vitreous cavity, consistent with previous studies.
根据莱考夫的阐述,算术是沿路线运动的隐喻与算术是量尺隐喻也同样有着密切的关系。他指出,我们运动的路线形成了一条物理线段—一一条沿着我们的轨迹的想像的线。运动的路线和物理线段之间有着简单的关系。运动的起点与物理线段的一端相一致,运动的终点与物理线段的另一端相一致,运动的路线与物理线段的剩余部分相一致。正是因为有了路线与物理线段的这种一致性,所以有了与量尺隐喻相关的“算术是沿路线运动”的隐喻。[2]71-72
This study has some limitations. First, there was no control group. Some patients with exudative retinal detachment experience spontaneous recovery, but this may take a long time. Previous studies have shown that prolonged retinal detachment durations lead to gradual vision impairments.Therefore, surgery is required in cases with exudative retinal detachment, especially when the macula is involved. Second,most of the patients lived far away from the hospital and were spread across the country; therefore, data on the patients' final vision values could not be obtained because patients tended not to attend the follow-up if retinal reattachment was achieved.Our study did not statistically detect the relationship between patients' visual acuity and preoperative visual acuity as well as the preoperative lesion time. Previous studies have shown that there is no statistical correlation between postoperative visual acuity and preoperative lesion time.
In conclusion, we found that four-quadrant scleral lamellar sclerectomy combined with partial full-thickness sclerostomy was safe and effective for patients with IUES. In patients with relapse, reoperation is still safe and effective. Among IUES patients, the axial axis is normal, but the thickness and composition of the sclera are abnormal. Further research is needed to determine the causes of scleral thickening and component changes; genetics or metabolism may play a role in the disease course.
None;None;None.
杂志排行
International Journal of Ophthalmology的其它文章
- Leptin activates the JAK/STAT pathway to promote angiogenesis in RF/6A cells in vitro
- CCPG1 involved in corneal Aspergillus fumigatus infection
- Anti-scarring effect of sodium hyaluronate at filtration pathway after filtering surgery in rabbits
- Five-in-one: a novel, cost-effective yet simple use of micro needle holder
- CO2 laser-assisted sclerectomy surgery and trabeculectomy combination therapy in Peters’ anomalyrelated glaucoma: a case report
- Congenital fibrovascular pupillary membranes: case series with pathological correlation and surgical treatment