Multicentric recurrence of intraductal papillary neoplasm of bile duct after spontaneous detachment of primary tumor: A case report
2022-03-07FukuyaKuwanoNagasawaMoritaTanakaYadaMasumotoMotomura
INTRODUCTION
Multiple endocrine neoplasia type 1 (MEN1) is a rare hereditary tumor syndrome inherited in an autosomal dominant manner and characterized by a predisposition to a multitude of endocrine neoplasms, mostly of the parathyroid, endocrine pancreas and anterior pituitary tumors. Other endocrine tumors in MEN1 include gastroenteropancreatic neuroendocrine tumors, adrenocortical tumors, and rarely pheochromocytoma[1-3]. MEN1 is caused by inactivating mutations ofgene. The incidence is 1/10000–1/100000.is a tumor suppressor gene and is located on human chromosome 11q13.gene is 9 kb and contains 10 exons. Exons 2–10 are coding regions.gene encodes the protein menin, which contains 610 amino acids[4,5].Menin plays an important role in cell division and proliferation, cell cycle regulation and genomic stability. Mutations ofgene can lead to functional loss of menin,and occurrence of multiple tumors[6-11]. Gene mutation analysis is an important diagnostic method for MEN1[1].
It has been reported that expression of menin is preserved in human normal thyroid tissue and thyroid tumors, but it can be decreased or absent in certain types of thyroid tumors[11-14]. Currently, little is known about the prevalence of papillary thyroid carcinoma (PTC) and nodular goiter in MEN1 patients, and it is unclear whether tumorigenesis of these thyroid tumors is MEN1 related. The role of menin protein deficiency in tumorigenesis of PTC and/or nodular goiter is still controversial. Here,we present a patient with MEN1 accompanied by coinstantaneous PTC and nodular goiter and review the related literature.
CASE PRESENTATION
Chief complaints
肋骨骨折是胸部创伤最严重的表现形式,是仅次于颅脑创伤致死的第二大病因,其死亡率在2%~20%[1]。肋骨骨折的诊断主要靠影像学检查,而骨折的定位和诊治往往涉及到肋骨的分段。为此,临床提出了肋骨的“解剖学分段”,而影像也提出了肋骨的“影像学分段”。我院从2015年CT运行以来便开始总结并提出了“肋骨CT四段法”。本研究通过对肋骨CT分段的应用,以及对各区段肋骨骨折发生率和临床术后诊断符合率的统计分析,来探讨肋骨的CT分段在肋骨骨折诊治中的应用价值。
伊泰普水电站1996年至2011年的年度发电量统计表和2012年、2013年的相关报导显示,其每年的年发电量绝大多数的年份都超过了819.9亿kW·h,自2007年装机容量达到14 000 MW以后,除2010年的年发电量为859.7亿kW·h以外,每年的年发电量都超过了900亿kW·h其中2012年为982亿kW·h,2013年的年发电量达到986.3亿kW·h。这也充分证明伊泰普水电站的这种装机容量选择的方法对其它这种类型的水电站装机容量选择非常适用。
History of present illness
Her father had a history of stomach surgery, but the details were unknown since he died 20 years ago. Other relatives of the patient had no symptoms of MEN1 syndrome.
水表和人们的生活密切相关,常见水表是由壳体、套筒、内芯三个部分组成。在日常使用中,水表的计量性能和安装环境、使用条件、管网水质等密切相关。以下结合实践,探讨了计量准确度的影响因素和改进对策。
History of past illness
式中:r为电动机转动半径;δ为等效旋转质量比;Cd为阻尼系数;Af为前区面积;vk为电动机速度;fr为滚动阻力;idf为差速比.
Personal and family history
The patient immediately came to our hospital after discovery of the neck mass.
Physical examination
Because the patient had a large functional parathyroid cyst, her serum calcium and iPTH levels were significantly abnormal and several solid nodules were detected in the right thyroid lobe (the largest nodule was suspected to be malignant by ultrasound). Fine needle aspiration (FNA) could not be performed for parathyroid cysts. And the patient refused FNA of the thyroid nodule before operation for fear of additional injury and requested to perform rapid intraoperative pathological diagnosis. Parathyroidectomy and unilateral thyroid lobectomy were recommended and performed with the patient’s consent.
There was an anterior neck mass which was movable due to breathing.
Laboratory examinations
The results of biochemical tests were as follows: serum calcium 2.82 mmol/L(reference range: 2.11–2.52 mmol/L); albumin 47.7 g/L (reference range: 40–55 g/L);serum intact parathyroid hormone (iPTH) elevated to 676.3 pg/mL (reference range:12–88 pg/mL); gastrin 17: 0.8 pmol/L (reference range: 1–15 pmol/L); thyroid function was normal; thyroid peroxidase antibody was 23.98 IU/mL (reference range:< 35 IU/mL).
A 35-year-old woman presented with a neck mass on physical examination, but without abnormal feelings.
Imaging examinations
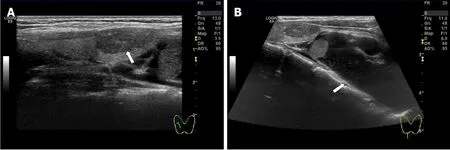
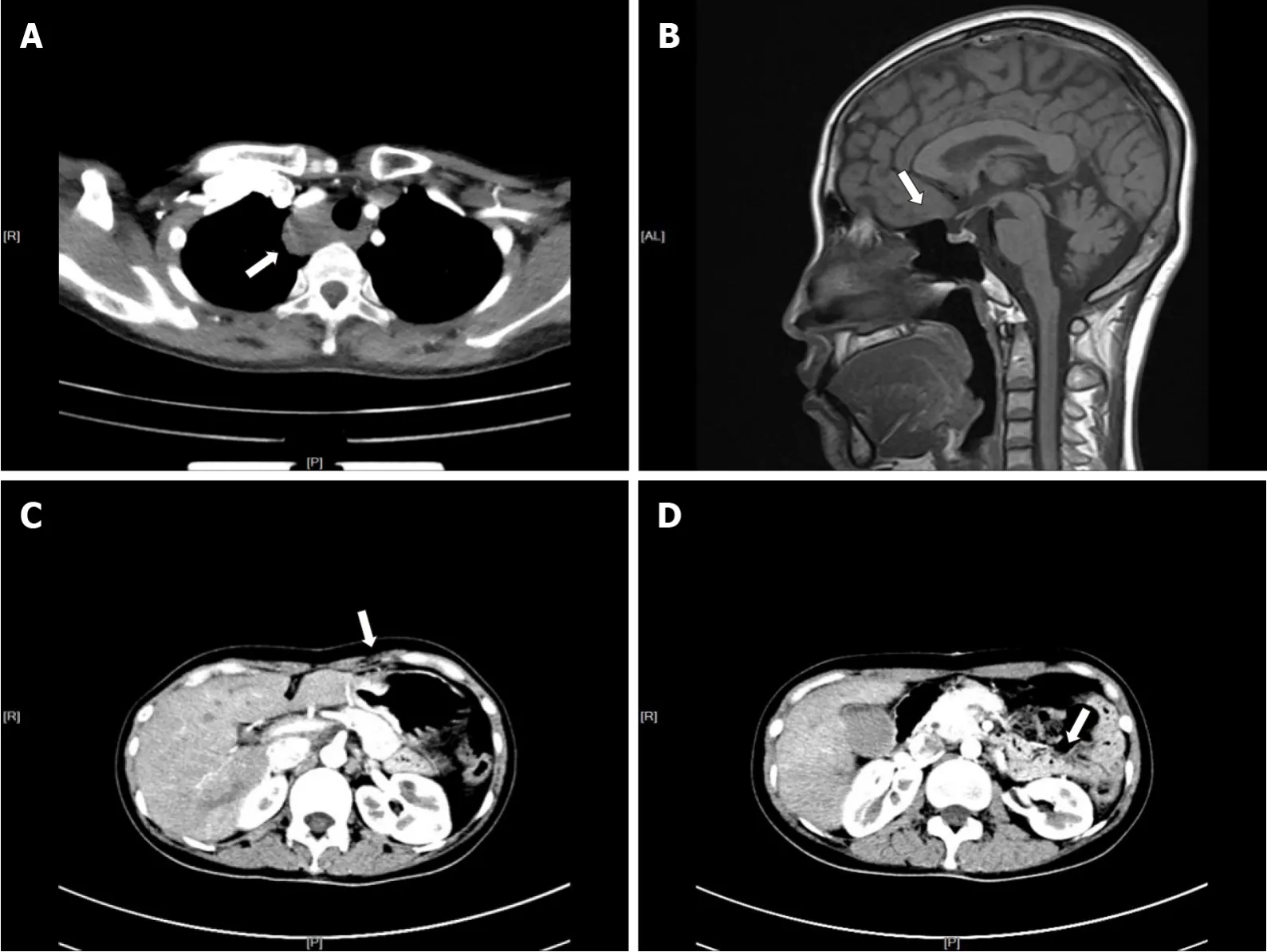
Neck ultrasound revealed a 64 mm × 28 mm × 45 mm cystic mass located below the right lobe of the thyroid gland with a well-defined smooth border, and several solid nodules were detected in the right thyroid lobe, with the largest (18 mm × 10 mm × 8 mm) in the right lower thyroid lobe. The largest nodule in the thyroid had an unclear boundary, dotted calcification and abundant internal blood flow (Figure 1A and B).Computed tomography (CT) or magnetic resonance imaging examination showed changes in the pituitary region; lesions in the right thyroid lobe and superior mediastinum; and changes after partial gastrectomy and in the tail of the pancreas(Figure 2A–D). In 99mTc-methoxyisobutyl isonitrile scintigraphy, tracer uptake was increased in the right lower region of the thyroid gland and mediastinum, and no abnormal retention of the tracer in the late phase was observed. No uptake was detected in other regions. Preoperative sestamibi single-photon emission computed tomography (SPECT)/CT found a lesion in the right lower thyroid lobe and part of which extended to the superior mediastinum (Figure 3A). Bone scanning showed Tscores -2.6 and Z-scores -2.0.
FINAL DIAGNOSIS
The final diagnosis of the presented case was thyroid neoplasm (right lobe).
The patient underwent partial resection of the pancreas and stomach for pancreatic and gastroduodenal neuroendocrine tumor 4 years ago. The patient had a history of pituitary microadenoma for 2 years, which was not treated but under observation.
TREATMENT
Her father had a history of stomach surgery, but the details were unknown since he died 20 years ago. Other relatives of the patient had no symptoms of MEN1 syndrome.
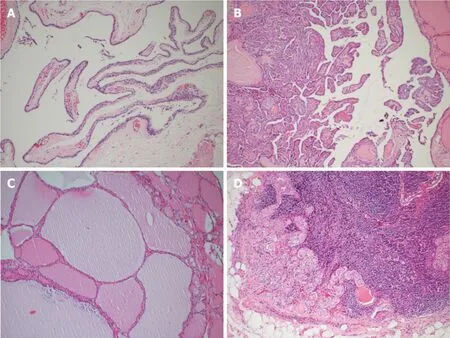
During the operation, gross examination of the largest cyst showed that it was partially surrounded and contiguous with the right lower thyroid lobe and extended to the superior mediastinum, and it was peeled off easily from the right lower thyroid lobe and mediastinum. Furthermore, it was filled with clear watery fluid, suggesting that it was a parathyroid cyst (Figure 3B). The largest cyst and right lobe of the thyroid were removed. The central lymph nodes were cleared. Intraoperative frozen section pathology showed that the largest cyst was the source of parathyroid, and parathyroid carcinoma was excluded. A PTC (maximum diameter 1 cm, invading the capsule) was found in the thyroid right lobe. In the central lymph nodes, 4/5 had cancer metastasis.iPTH at 20 min after resection was decreased to 253.4 pg/mL. Other parathyroid glands were explored. Two upper parathyroid glands were normal. The left lower parathyroid was enlarged and removed. Rapid intraoperative pathological examination revealed that the left lower parathyroid had adenomatoid hyperplasia.After another 20 min, serum iPTH decreased to 63.9 pg/mL. The postoperative pathological results were PTC (maximum diameter 1cm, invading the capsule) in the right thyroid lobe and nodular goiter. In the central lymph nodes, 4/5 had PTC metastasis. In the right cervical cysts, parathyroid cysts (monolocular) showed adenomatous hyperplasia. In the left lower parathyroid, adenomatous hyperplasia was observed (Figure 4). The patient had indications for a total thyroidectomy because of central compartment lymph node metastasis. But the patient had a strong desire to preserve the thyroid gland and refused to remove the left lobe.
After surgery, the patient was closely monitored on serum calcium and was pumped calcium gluconate 2.0 g/day through a central venous catheter for 5 d. After taking 1.5 g calcium carbonate daily for 3 mo, her serum calcium levels returned to normal. Meanwhile the patient received endocrine suppression therapy after the operation.
OUTCOME AND FOLLOW-UP
After the operation, genetic analysis was performed, and a germlinegene mutation was detected. There was a heterozygous mutation in the second exon ofgene which was 357-360delCTGT. During follow-up, there was no hypoparathyroidism or other complications. The laboratory data on postoperative day 2 showed that serum calcium was 1.98 mmol/L and iPTH was 24.1 pg/mL. After taking 1.5 g calcium carbonate daily for 3 mo, the patient’s laboratory data improved: calcium 1.98 mmol/L and iPTH 43.7 pg/mL. Calcium was 2.47 mmol/L and iPTH was 61 pg/mL after 18 mo. One month after the operation, the dose of levothyroxine was reduced from 75 mg to 50 mg.

DISCUSSION
Currently, the role of inactivating mutations ofgene in tumorigenesis of PTC and/or nodular goiter is still controversial. It remains to be determined by more case reports and further research.
在饲料中增加一定比例的脂肪粉或者植物油,适度提高能量水平。公猪和母猪可适当的增加饲喂量,并添加具有抗应激、抗氧化能力的饲料添加剂,以增强猪体的抗寒能力。保育期采用湿拌料饲喂方式的,使水的温度保持在20℃~30℃,禁止使用冷水饲喂。
MEN1 is a rare hereditary tumor syndrome inherited in an autosomal dominant manner and presents mostly as the parathyroid[15], endocrine pancreas (such as gastrinoma)[16] and anterior pituitary tumors[17]. Other endocrine and nonendocrine lesions of MEN1, such as adrenal cortical tumors, carcinoids of the bronchi,gastrointestinal tract and thymus lipomas, angiofibromas, and collagenomas, have also been described[1,18]. MEN1 with a large functioning parathyroid cyst is rare. Cavalli[15] found that approximately 300 cases of sporadic parathyroid cysts had been reported up to 2017, and only two cases have been described in MEN1. Parathyroid cysts can be divided into functioning and nonfunctioning, and most parathyroid cysts are nonfunctioning. The functioning parathyroid cysts are more likely to be caused by degenerative changes in parathyroid adenoma than hyperplasia in our case[19]. In many cases, it is difficult to diagnose the nature of the cyst merely by ultrasound before surgery. Parathyroid cysts need to be differentiated from lymphatic cysts, cystic thyroid nodules and hemangioma[20,21]. The diagnostic rate can be improved by laboratory examination and other imaging examinations. Preoperative SPECT/CT is useful in localizing parathyroid cysts in most patients, with an accuracy rate up to 79%if it is interpreted in combination with cervical ultrasound images[22]. Postoperative pathological diagnosis is the gold standard. The clinical features of hyperparathyroidism (HPT) with MEN1 are similar to those with sporadic HPT, but the former is often more aggressive. For patients who have HPT with MEN1, early surgical treatment is preferred. Surgical treatment should be considered in asymptomatic patients when (1) serum calcium is higher than the reference range 2.52mmol/L; (2)glomerular filtration < 60 mL/min; (3) bone mineral density at any point is 2.5 or lower, or patient has fragility fractures; and (4) age < 50 years. Whether early surgery can reduce the incidence rate and mortality is not clear. For patients who have HPT with MEN1, especially in asymptomatic or mild and young patients, early parathyroidectomy can reduce the long-term effects of HPT on the patients, especially reducing the bone loss. Although our case was a young woman with normal upper parathyroid glands on both sides, and bilateral lower parathyroid glands showed adenoma-like changes and hyperplasia, parathyroid hormone and serum calcium levels had increased significantly. To avoid a permanent hypoparathyroidism, we did not perform subtotal parathyroidectomy or a total parathyroidectomy with parathyroid tissue autotransplantation. And based on our past experience, unless it is a parathyroid cancer, surgery can achieve a better treatment effect by removing the problematic parathyroid glands. In the present case, the parathyroid hormone had decreased from 676.3 pg/mL to 63.9 pg/mL after the removal of the bilateral inferior parathyroid glands, and the patient’s serum parathyroid hormone was 47.6 pg/mL at 27 mo postoperatively. FNA is the most useful means for diagnosis of thyroid nodules,however, it is not widely accepted for diagnosis of parathyroid tumors due to the risk of dissemination of tumor cells.
据介绍,每一个合作的农户或种植基地,农拓者都会安排专业人员对土壤进行分析,收集历年作物生长、天气变化等大量数据,在大数据的基础上量身打造出覆盖种、肥、药和田间管理等多方面的全程种植解决方案,并在种植过程中进行监督化的跟踪管理。在这种模式下,农民的种植水平得以提升,避免了肥药的浪费和无效施用,精准的病虫害解决方案保障了作物健康,促进了农民增产增收,交出了辣椒亩产增幅30%、番茄亩产增幅40%、其他作物均有不同比例增产的答卷。
Two different forms of MEN1, sporadic and familial, have been described[23]. The sporadic form presents with two of the three principal MEN1-related endocrine tumors (parathyroid adenoma, enteropancreatic tumor and pituitary tumor) within a single patient, while the familial form consists of MEN1 with at least one first-degree relative showing one of the endocrine characteristic tumors[24-27]. In our case, the patient did not provide a clear family history. It is still unclear what form of MEN1 our patient had. There is no evidence to exclude the accidental occurrence of MEN1 with PTC and nodular goiter in this patient.
So far, few cases of thyroid carcinoma and/or nodular goiter combined with MEN1 have been reported. Whether there is a correlation among them is still controversial[12,28,29]. Hill[30] investigated the probability of concomitant thyroid cancer in patients with MEN1. They found that in patients with MEN1, a 28% substantial incidence of thyroid cancer was observed and all cancers in MEN1 patients were common PTCs histologically (100%). We noticed that only PTCs that measured >1 cm in diameter were considered in the report by Hill[30]. But at present, papillary thyroid microcarcinoma (PTMC) accounts for more than half of all PTCs in clinical practice. If we take these PTMC cases into account, the actual incidence of papillary thyroid carcinoma would be higher in MEN1 patients. Our case was PTMC. MEN1 is caused by inactivating mutations of thegene that encodes the protein menin[2]. Menin is a nuclear protein whose interaction with several other nuclear proteins indicates a role in transcriptional regulation. Previous studies have supported a role for MEN1 in controlling cell growth and differentiation, and in sensing or repairing DNA damage as well. The loss of menin function in tumor precursor cells is involved in the mechanism underlying tumor formation in MEN1[8-10,31-33]. Research showed that the inactivation of menin in the thyroid gland of young mice affected the proliferation of follicular cells[13]. Capraru[11] showed that the expression of menin was positive, identical to normal thyroid tissue, but it could be decreased or absent in some thyroid tumors including PTC. As is well known, mutations of thegene cause deficiency in the menin protein in MEN1 patients. There was a heterozygous 357-360delCTGT mutation in the second exon of MEN1 gene in our case. Further molecular studies are needed to evaluate the role of menin protein deficiency in tumorigenesis of PTC and nodular goiter. Kazubskaia[34] investigated follicular cell (papillary and follicular) thyroid carcinoma, genetic inheritance and molecular diagnostic markers. They believed that familial PTC and PTC may be a component of multitumor syndromes, such as MEN1, Cowden syndrome, and familial adenomatous polyposis. We speculate upon possible reasons for the association between MEN1 and PTC/nodular goiter. Loss of heterozygosity (LOH) studies have been used to identify sites harboring tumor suppressor genes involved in tumor initiation or progression.is a tumor suppressor gene located on human chromosome 11q13. Specific genomic areas, such as 3p22, 7q31, 11q13 and 11q23, have been reported to be involved in some epithelial or endocrine tumor types[35]. PTC is also one of the endocrine tumors. Whether inactivating mutations of 11q13 can induce PTC remains to be further studied. Chu[36,37] found MEN1 deletion in neurotrophic tyrosine kinase receptor (NTRK)-rearranged PTC patients. They also proved that nucleotide variants and indels in pTERT, MEN1 and CDH1 were observed in several kinase fusion-related PTCs. The relationship among MEN1, PTC and NTRK needs to be further studied. In the analysis ofgene, about 20% may have false negative results due to the diversity of the causative mutation and scattered position in the entire open reading frame. Moreover, approximately 10% new germline mutations are being detected in the overall MEN1 patients, which may be the reason why the genotype- phenotype correlations could not be identical in 10%-30% of patients[38]. In 2008, Kim[29]reported the first case of PTC combined with MEN1 in Korea. Their patient’s genetic analysis of DNA had revealed no germline mutation ingene locus. But there was a genetic mutation in our case. Menin, the protein encoded bygene is ubiquitously expressed in endocrine tissues, is less in many endocrine tumors including PTC. Deletion of the MEN1 tumor suppression still might be etiologically related to the oncogenesis of PTC. DNA analysis of more samples with PTC combined with MEN1 may be helpful. Now it is very difficult to confirm the LOH ofgene completely and accurately, which has dozens of polymorphic markers[29]. The clinical aspects and molecular genetics of MEN1 were reviewed together with the reported 1336 mutations[39]. It has been proved that many of the diseases that have been widely believed to be associated with MEN1 mutations, such as pituitary tumors, lung carcinoids,, sometimes failed to exhibit meaningful LOH at 11q13[40]. For PTC,some people have used three of polymorphic markers to test one patient’s sample,with limited results[12]. The exact significance remains to be determined by more case reports and further research. It is another possibility that MEN1 patients who develop PTC may have specificmutations of the affected allele that act like dominant oncogenes with regard to thyroid cancer oncogenesis. If any of these scenarios was the case, thegene could play a role in the development of the papillary cancer without obvious LOH of the gene locus.
CONCLUSION
In summary, we presented a rare case of MEN1 combined with PTC and nodular goiter, in which a germline mutation of thegene was detected. It is possible there is a potential correlation between MEN1 syndrome and PTC/nodular goiter.However, further studies and additional case reports are required to clarify it.
猜你喜欢
杂志排行
World Journal of Clinical Cases的其它文章
- Mycoplasma hominis meningitis after operative neurosurgery: A case report and review of literature
- Recurrence of sigmoid colon cancer–derived anal metastasis: A case report and review of literature
- New method to remove tibial intramedullary nail through original suprapatellar incision: A case report
- Metastasis to the thyroid gland from primary breast cancer presenting as diffuse goiter: A case report and review of literature
- Gastric submucosal lesion caused by an embedded fish bone: A case report
- Epibulbar osseous choristoma: Two case reports