Socio-ecological determinants of dengue prevention practices: A cross-sectional study among wet market traders in a selected district in Perak, Malaysia
2022-01-15KamaruddinSalmiahbtMdSaidKadirShaharLim
N.I.K. Kamaruddin, Salmiah bt Md Said, H. Kadir Shahar, P.Y. Lim
Faculty of Medicine and Health Science, Universiti Putra, Kuala Lumpur, Malaysia
ABSTRACT
Objective: To determine the level of dengue prevention practices among wet market traders in a Malaysian district and their associated socio-ecological factors including individual, relationships,community and societal factors.
Methods: A cross-sectional study involving 246 wet market traders was conducted in a district in Perak state in northwest Malaysia between September 2018 to June 2019. Participants were selected through stratified sampling from four wet markets in Hilir Perak district. Data on dengue prevention practices and associated socioecological characteristics were collected using a validated interviewbased questionnaire. The data were analyzed using SPSS version 25. Multiple logistic regression was performed to identify socioecological determinants of dengue prevention practices among wet market traders in Hilir Perak District.
Results: From the total number of respondents, 78% had high dengue prevention practices. Higher dengue prevention practices were associated with owners of wet market shoplots compared to employed workers (adjusted OR 4.18, 95% CI 1.78, 9.85), high perceived susceptibility (adjusted OR 6.93, 95% CI 3.02, 15.92),high familial support (adjusted OR 3.65, 95% CI 1.25, 10.64), and high perceived dengue prevention and control laws and regulations(adjusted OR 3.24, 95% CI 1.44, 7.32).
Conclusions: Dengue prevention practices were associated not only with individual determinants but also with other determinants from relationships to societal level which must be considered in planning or evaluating current dengue control programs.
KEYWORDS: Dengue; Aedes breeding; Socio-ecological factors;Health belief; Wet market
Significance
Other than residential areas, public places are known as sources of potential habitats for Aedes mosquitoes. Wet markets in South East Asia serve as example of public places that have been linked with dengue outbreaks and vector breeding previously. This study explored the level of dengue prevention practices among wet market traders in a Malaysian district and identified the socioecological determinants associated with their practices.
1. Introduction
Dengue virus is transmitted by Aedes aegypti and Aedes albopictus which transmit the virus from infected to healthy individuals through bites. In 2019, dengue infection has recorded the highest incidence among all communicable diseases in Malaysia[1].Vaccination against dengue is a programmatically difficult approach to achieve high population protection from dengue due to excess risk of developing severe dengue in seronegative vaccinated individuals, compared to seronegative non-vaccinated individuals,which necessitates pre-vaccination screening[2]. Therefore, current approach to prevent and control dengue epidemics is still directed towards behavioural modifications in combatting mosquito vectors. This strategy emphasizes on the importance of community participation in prevention and elimination of mosquito breeding,personal protection of mosquito bites, and prevention of further transmission by seeking early diagnosis and treatment[3].
Previously, many studies had described the level of dengue prevention behavior in residential areas[4-6]. With regards to nonresidential areas, a study in Malaysia has established that public places such as schools, restaurants, mosques and parks contribute to proliferation of dengue vectors by housing a significant number of breeding containers, especially plastic containers[7]. However,to our knowledge, dengue preventive practices in wet markets specifically are not well studied despite occurrence of outbreaks and evidence of vector breeding found in wet markets[8,9]. A study using geostatistical analysis found a significant correlation between the number of dengue cases and traditional markets[10].Routine practices by wet market traders such as storing water in containers for cleaning and keeping marine products and vegetable produces fresh are examples of behaviour that could lead to Aedes breeding. Wet markets are also patronized by high number of visitors on daily basis, especially in the morning when Aedes mosquitoes are actively biting[11].
Furthermore, earlier work on dengue prevention practices conducted in residential areas did not explore determinants of preventive practices beyond individual level. Socio-ecological model may serve as a good framework to enable the understanding on not only individuals but also on communities and societal determinants of dengue prevention practices among target population. Other than social capital which may influence health behaviour, lack of community participation and enforcement by the authorities in dengue prevention are among the community and societal characteristics recognized to increase the risk for dengue infection[12]. Thus, this study aimed to determine the level of dengue prevention practices among wet market traders in Hilir Perak District and to identify socio-ecological determinants of dengue prevention practices, which are socio-demographic,individual, relationship, community, and societal determinants.
2. Subjects and methods
2.1. Study design and participants
This study was conducted in four daily wet markets operating in Hilir Perak District, located in northwest Malaysia. The study took place from September 2018 to June 2019 and employed a crosssectional study design. The sample size was calculated based on a study conducted in Peninsular Malaysia[13], using the twoproportion formula for hypothesis testing


The stratified sampling method was used, where all four wet markets in the district were first stratified into urban and suburban wet markets. The district has five mukims (subdistrict divisions) including one administrative mukim. Wet market located in administrative mukim was classified as urban, while remaining wet markets in less urbanized mukims were classified as sub-urban. Stratification was made on the basis that urban wet market traders were hypothesized to have better access to health information and resources that may lead them to better prevention practices compared to sub-urban wet market traders. Subsequently,an equal number of shoplots were selected from each stratum.Estimating that there would be at least two respondents from each shoplot, an equal number of 166 shoplots were selected from each stratum (83 shoplots from the urban stratum, and 83 shoplots from the suburban stratum) to achieve the calculated sample size of 332. Shoplots which were operating on daily basis were selected randomly by using an online random number generator with each shoplot having the same chance to be selected. From the selected shoplots, all traders and workers aged 20-65 years old, who had worked for at least 1 month in the shoplot and worked in the wet market for at least three days in a week were invited to take part in the study. Shoplot owners and workers who did not perform housekeeping and cleaning tasks were excluded from the study.
2.2. Study instrument and data collection
This study used a set of interview-based questionnaires that contained seven sections as follows: sociodemographic characteristics, dengue prevention practices, knowledge on dengue infection and its vectors, health beliefs, social support, community participation, and societal factors. The dengue prevention practices scale was adapted from a previous study on dengue prevention practices nationwide in Malaysia[4]. The options for practices in this study were “not at all”, “rarely”, “often”, “frequent” with assigned points of 0, 1, 2 and 3, respectively. Total points for this scale were 52. The total points of dengue prevention practices were converted into percentage. The number of items to which a respondent answered as “not applicable” was calculated and multiplied by maximum points (3 points), summated, and deducted from the denominator when deriving the score in percentage. The scores were then divided into two categories, which were low (0%-49%)and high (50%-100%).
Knowledge was divided into seven sub-sections, namely:knowledge about dengue and Aedes spp. mosquito, knowledge about the transmission of dengue, knowledge about prevention,knowledge of signs and symptoms of dengue, signs and symptoms of severe dengue, knowledge about treatment, curability and precaution measures for people who may be infected with dengue,and general knowledge about dengue outbreak control measures.For each statement, the respondent would choose between three answers: “yes”, “no” and “not sure”. Each “yes” answer was scored as 1 and “no” and “don’t know” answers were scored as 0. Based on previous studies, the knowledge score was calculated into percentage and further categorized into low (0%-79%) and high (80%-100%)[5,16].
The health belief scale was adapted from a previous study on dengue prevention practices[17]. There were four subconstructs in this scale, namely perceived severity, perceived susceptibility,perceived benefits and perceived barriers. A 5-point Likert scale ranging from 1 for “strongly disagree” to 5 for “strongly agree”was used. For each subconstruct, cut-off point was calculated by using mid-point calculation [(maximum score-minimum score)/2+minimum score] to categorize the respondents into those with high and low scores. The Multidimensional Scale of Perceived Social Support was adopted to measure the social support received from spouse, friends and family[18]. For this study, a 5-point Likert scale was used with each subconstruct’s score ranges from 4 to 20. A score of 4 to 12 was considered as low, and a score of 13 to 20 was considered as high spousal,familial and friendship support.
Community participation was measured by using three items using 5-point Likert scale with the total score ranged from 3 to 15. A score of 3 to 9 was regarded as low, and a score of 10 to 15 was regarded as a high level of community participation. For societal factors, perceived dengue prevention and control laws and regulations, and communication and assistance received from local authorities were measured using six and five items,respectively. A score of 6 to 18 indicated low perceived dengue prevention and control laws and regulations, while a score of 19 to 30 indicated high perceived laws and regulations. Meanwhile,for communication and assistance received from local authorities,a score of 5 to 15 indicated a low level, while a score of 16 to 25 indicated a high level of communication and assistance received.
Forward and backward translations were performed by professional translator and verified by a public health physician.Face validity was performed to evaluate the phrasing and item understandability. Content validity was also assessed through a panel of experts consisting of two public health physicians who reviewed the questionnaire. Internal consistency reliability test was performed to measure Cronbach’s alpha using IBM Statistical Package for Social Sciences (version 25). For each subconstruct,Cronbach’s alpha ranged from 0.652 to 0.942. For test retest,intraclass correlation coefficient was used to assess the reliability of the scales. Intraclass correlation coefficient values obtained ranged from 0.764 to 0.978, indicating good and excellent reliability[19]. The researcher was assisted by two trained data collectors and met respondents individually to conduct interviews based on the questionnaire. The answers were entered into an electronic datasheet by the interviewer in the field. The datasheet mandatorily required an answer for every question before it allowed the user to proceed to the next section, thus eliminating any possibility of missing data. The overall activities of the data collectors were monitored directly on site by the researcher with strict supervision. Twenty completed questionnaires were checked randomly for completeness and consistency.
2.3. Data analysis
The data was analyzed using IBM Statistical Package for Social Sciences version 25 for Windows. Following descriptive statistical analysis, the relationship between dengue prevention practices and independent variables such as sociodemographic factors,knowledge, attitude, health belief, relationship factors, community factors, and societal factors was examined using the Chi square test. Association in cells that contained less than 20% or less than 5 counts of total number was analyzed using Fisher’s exact test. A subsequent analysis using simple logistic regression was performed to estimate the relationship between the level of dengue prevention practices with each of the independent variables.Following that, multivariate analysis using multiple logistic regression model was performed to obtain the socio-ecological determinants of dengue prevention practices. Multicollinearity was checked and there was no highly correlated variable. Assumptions for multiple logistic regression were checked using classification table (overall percentage>70% was considered adequate), Hosmer and Lemeshow test (P value >0.05 and small discrepancy between observed and expected probability), and Receiver Operating Characteristics curve (area more than 0.7) to find the best final regression model.
2.4. Ethical approval
Ethical approval was obtained from University Putra Malaysia’s Ethics Committee for Research Involving Human Subjects before data collection (No. UPM/TNCPI/RMC/1.4.18.2). The research was also registered with the Malaysian National Medical Research Register. All procedures complied with ethical standards and Helsinki Declaration of 1975. Permission to conduct the study at the wet market facilities was requested and approval was obtained from the President of the local council in writing. In addition,informed written consent was obtained from each respondent who took part in this study. Confidentiality of information was maintained through keeping safe records of the responses, and anonymity of data management and analysis.
3. Results
3.1. Characteristics of wet market traders
The response rate was 88.55% (147/166) among the shoplots,and 86.93% (246/283) for wet market traders. Most of the respondents were male (55.69%), 78.05% respondents received up to secondary school education, with average monthly household income of USD 473, and 81.30% had married (Table 1). A majority of the respondents had high level of dengue prevention practices (192, 78.05%). Figure 1 displays the distribution of respondents according to dengue prevention practices that were most frequently used. The least frequently practiced dengue preventive measures were “putting Abate/chemical in water storage containers” (0.8%), “applying insect repellent over exposed body parts everyday” (0.8%), and “wearing bright colored clothes to avoid mosquito bites” (2.0%).

Table 1. Distribution of respondents according to sociodemographic characteristics.
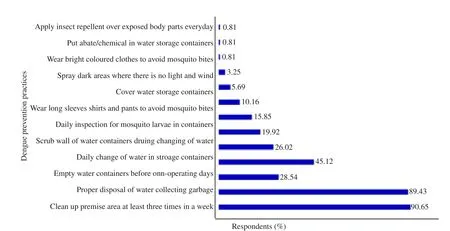
Figure 1. Percentage of respondents according to type of prevention practices.
Table 2 summarizes the distribution of respondents according to individual, relationships and societal characteristics. A total of 99 respondents (40.24%) had a high level of knowledge (80%and above). More than half of the respondents (57.32%) had high perceived susceptibility while a majority of the respondents had high perceived severity (95.12%). As shown in Table 3, perceived social support from relationships that was assessed in this study were from spouse/partner, family and friends. A majority of respondents received high spousal support (80.08%), high familial support (90.24%), and high friendship support (71.14%) as shown in Table 3. Low community participation was reported by 94.72%of the respondents, while half of the respondents perceived dengue prevention and control laws and regulations as good (52.03%).

Table 2. Distribution of respondents according to individual characteristics.

Table 3. Distribution of respondents by other socio-ecological characteristics(N=246).
A total of 66.20% of the respondents thought that health inspectors should not be allowed to break into empty or locked premises if the premises were suspected to host Aedes breeding places, while only 34.55% and 46.75% considered that maximal compound, and general dengue prevention and control legislations, respectively, to have benefits toward their dengue prevention practices and behavior. For communication and assistance received from local authorities, 50.81% of the respondents reported a low level of communication and assistance from local authorities. However, 61.38% stated that they have received dengue information from local authorities. About half of the respondents (53.66%) have had their premises inspected by the authorities before, and 43.50% stated that they have received recommendations on dengue prevention. As many as 35.77% of respondents stated that they could contact local authorities if they ever needed help with dengue prevention activities, while 42.68%were not sure and 21.54% felt that they did not have access to contact local authorities (data not shown).
3.2. Socio-ecological determinants of dengue prevention practices
Bivariate analysis using simple logistic regression was conducted and 13 variables were found to have significant association with the level of dengue prevention practices (Table 4). All variables with P value of less than 0.25 and another two variables which are likely to influence the level of practices (types of products sold and communication/assistance received from local authorities)were then included as candidates in multivariable modelling.Table 5 shows the result obtained from multiple logistic regression analysis. The owners of wet market shoplots had four times higher odds of having a high level of dengue prevention practices compared to hired workers (AOR 4.18, 95% CI 1.78, 9.85). The second socio-ecological determinant was one of the health belief subconstructs, namely perceived susceptibility, where it was found that respondents with high perceived susceptibility had an almost seven times odds to have high level of dengue prevention practices compared to those who had a low score of perceived susceptibility(AOR 6.93, 95% CI 3.02, 15.92). Respondents who had higher familial support were nearly four times more likely to have high level of dengue prevention practices compared to those with less familial support (AOR 3.65, 95% CI 1.25, 10.64). One of the societal determinants was also found to be significantly associated with the level of practice, where it was found that wet market traders with better perceived dengue prevention and control laws and regulations were three times more likely to have high level of dengue prevention practices compared to those who scored lower on this subconstruct (AOR 3.24, 95% CI 1.44, 7.32).

Table 4. Bivariate analysis of socio-ecological determinants associated with high level of dengue prevention practices (≥50%).

Table 5. Multivariable analysis of socio-ecological determinants associated with high level of dengue prevention practices (N=246).
4. Discussion
This study shows that a majority of the respondents had a higher level of dengue prevention practices, and it is comparable to a study done nationwide in Malaysia where 73% of respondents had a high level of dengue prevention practices[4]. However, a lower proportion of respondents were found to have high dengue prevention practices in a study conducted among aborigine population in Malaysia (55.4%)[13]. The difference observed maybe attributed to the difference in socioeconomic and educational background of common population and aborigine population in this country. Furthermore, this study has also found that putting Abatein water storage containers was practiced least frequently. A similar finding was observed in previous study conducted in Malaysia where it also revealed that putting Abatein water storage containers was among the least practiced dengue prevention (46.8%)[4]. This may be due to insufficient information received through health education activities intended to spread awareness and to clear misconceptions about the safety of larvicides that may serve as a barrier in larval control practice[20].Other than that, this study shows that 76% of the respondents had never used insect repellents. This low usage of insect repellent was also observed in local studies where only 11.3% and 10.7% of respondents had used insect repellents, respectively[4,13]. Hence,social media engagement, health education during enforcement activities and community campaigns should also stress on the importance of personal protective measures that can be used to prevent dengue, other than reducing sources of breeding.
In this study, employment status was shown to be significantly associated with dengue prevention practices through multivariate analysis. The owners of shoplots in the wet markets were more likely to have a high level of dengue prevention practices compared to workers hired to work in the shoplots. A qualitative study has found that perceived responsibility plays a crucial role in vector control[21]. The perception of responsibility possessed by owners of shoplots and their sense of belonging to the community of wet market traders may cause them to have higher dengue prevention practices compare to workers who are hired by shoplot owners. Therefore, it is important for authorities to address this factor by implementing strategies to create a sense of ownership in the community and strengthen social responsibility among all wet market workers, irrespective of their employment status. Usage of personal protection, frequent checking for mosquito breeding and removal of stagnant water should be considered as standard aspects that may be included in the checklist used by wet market shoplot owners during their employee orientation. Regular health campaigns conducted by authorities or community leaders can be made inclusive for all layers of wet market workers including newly employed workers.
In this study, all four subconstructs of health beliefs being studied(perceived susceptibility, perceived severity, perceived benefit,and perceived barrier) were found to be significantly associated with dengue prevention practices through bivariate analysis.However, after adjusting for the confounders, the final predictive model showed that only perceived susceptibility was able to significantly predict the level of dengue prevention practices where high perceived susceptibility increases the odds of having high dengue prevention practices. This finding is similar to many studies done previously. For example, perceived susceptibility was found to be a significant predictor for dengue prevention practices in studies conducted nationwide and on the Orang Asli (aborigine)population in Malaysia[4,13]. Previous studies that evaluated perceived susceptibility and perceived severity together as a perceived threat also found a significant association between these health belief subconstructs and dengue prevention practices[22].It outlines the importance of a person perceiving that they may contract a disease to influence them in making health decisions or change their health behaviors.
Familial support was found to be a significant determinant of high dengue prevention practices as derived from the multivariate analysis. Emotional and instrumental support received from friends and families were similarly considered as a component in social capital as measured in a cluster randomized controlled trial in Mexico[23]. The study has found that households with high social capital were more likely to be negative for larvae or pupae after adjusting for intervention status. These findings illustrated the important role of social support and social capital in health promotion and disease prevention. Finally, this study has found significant association between perceived laws and dengue prevention practices. Laws and regulations act as government“levers” to secure safer behavior among the population, whether through modification of individual behavior, regulation of agents of behavioural change (for example, regulation of unsafe and unhealthy practices), and alteration of informational, physical,social and economic environment to enable safer and healthier behavior[24]. Legal and regulatory interventions thus act as a critically important strategy to prevent injury and to promote health. The finding in this study shows that awareness and perception of laws among the public are important to ensure good preventive practices.
This study was based on self-reported practices of dengue prevention and not through objective observation of the practices.Therefore, the result depended on the honesty of the respondents.However, to minimize inaccurate reporting, the study objectives were explained thoroughly, and rapport was established to create trust and ensure honest responses from the interviewees. The respondents were told that there would not be any consequence or judgement and confidentiality would be kept. Some degree of selection bias may exist as 11.4% respondents did not agree to participate in this study and may otherwise represent the portion of respondents with lower level of prevention practices. Besides, the practices and their determinants may vary with health education and intervention programs that are being carried out by local authorities at a given time.
In conclusion, the majority of wet market traders in the district had high level of dengue prevention practices. Significant associations were observed between determinants from different levels of the Socio-ecological Model, which were individual(employment and perceived susceptibility), relationships (family support), and societal determinants (perceived dengue prevention and control laws and regulations). It is evident by this study that the level of dengue prevention practices is determined not only by individual but also by other socio-ecological determinants from relationship to societal levels which can be considered in planning or evaluating current dengue control programs.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Authors’ contributions
N.I.K.K and S.M.S developed the theoretical formalism. N.I.K.K acted as field investigator and performed the analytic calculations.P.Y.L. verified the analytical methods and calculations. N.I.K.K.took the lead in writing the manuscript, however all authors contributed to the final version of the manuscript. S.M.S.supervised the project, with assistance from H.K.S. All authors provided critical feedback and helped shape the research, analysis and manuscript.
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- Dissemination of scientific information to fight against COVID-19: Academic journals’ role
- Methods and parameters of melting curve analysis for identification of Leishmania species: A scoping review
- Intention of healthcare workers to accept COVID-19 vaccination and related factors:A systematic review and meta-analysis
- Predicting COVID-19 fatality rate based on age group using LSTM