Psychological predictors of bipolarity in panic disorder
2022-01-10DaHyeOhDooHeumParkSeungHoRyuJeeHyunHaHongJunJeon
Da Hye Oh, Doo-Heum Park, Seung-Ho Ryu, Jee Hyun Ha, Hong Jun Jeon
Da Hye Oh, Doo-Heum Park, Seung-Ho Ryu, Jee Hyun Ha, Hong Jun Jeon, Department of Psychiatry, Konkuk University Medical Center, Seoul 05030, South Korea
Doo-Heum Park, Seung-Ho Ryu, Jee Hyun Ha, Hong Jun Jeon, Department of Psychiatry, Konkuk University School of Medicine, Seoul 05029, South Korea
Abstract BACKGROUND Panic disorders frequently occur with affective disorders, particularly bipolar disorder. Patients with panic disorder and bipolar disorder are more likely to present with severe symptoms, such as high rates of suicidal behavior, poor symptomatic and functional recovery, and poor drug responses.AIM To investigate the psychological characteristics of panic disorder patients related to bipolarity.METHODS A total of 254 patients (136 men and 118 women, mean age = 33.48 ± 3.2 years) who were diagnosed with panic disorder were included in the study. Panic disorder with bipolarity (BP+) was defined as a score of ≥ 7 on the Korean version of the Mood Disorder Questionnaire (K-MDQ), and a score lower than 7 was considered as a panic disorder without bipolarity (BP-). Self-report questionnaires were analyzed to examine their association with bipolarity. Psychological tests used in the study were the Mood Disorder Questionnaire (MDQ), Panic Disorder Severity Scale, Beck Depression Inventory, State-Trait Anxiety Inventory (STAI), Temperament and Character Inventory (TCI), and Minnesota Multiphasic Personality Inventory (MMPI). Statistical analyses were performed to evaluate the correlation between bipolarity of panic disorder patients and various psychological test results indicative of psychological characteristics.RESULTS Patients with a K-MDQ score of 7 or more were considered to have a history of manic or hypomanic episodes (BP+ group, n = 128), while patients with K-MDQ scores below 7 were defined as those without bipolarity (BP- group, n = 126). The BP+ group were more likely to be unmarried (single 56.2% vs 44.4%, P = 0.008) and younger (30.78 ± 0.59 vs 37.11 ± 3.21, P < 0.001). Additionally, the BP+ group had significantly higher scores on psychological assessment scales, such as the hypochondriasis, psychopathic deviate, masculinity-femininity, psychasthenia, schizophrenia, and hypomania (Ma) in MMPI, and novelty seeking, harm avoidance and self-transcendence in TCI, and STAI (state and trait) compared to the BP- group. In logistic regression analysis, depression in MMPI, selfdirectedness in TCI, and age were negatively associated with MDQ score, meanwhile, Ma in MMPI and STAI (trait) were positively associated with MDQ score.CONCLUSION The result of this study suggests that almost 50% of patients with panic disorder are likely to have hypomanic or manic symptoms, and certain psychological factors are associated bipolarity in panic disorder.
Key Words: Panic disorder; Bipolar disorder; Bipolarity; Anxiety; Minnesota Multiphasic Personality Inventory; Temperament and Character Inventory
INTRODUCTION
Previous studies have shown that patients with bipolar disorder have a high risk of comorbid panic disorder[1]. In addition, patients with bipolar disorder have a higher risk of intra-episode panic disorder during mania[2]. A family study of bipolar disorder showed that there is a possible complex genetic etiology in bipolar disorder and panic disorder comorbidity[1]. MacKinnonet al[3] studied 528 members of 57 families for a genetic linkage study of bipolar disorder. They found that 10 families had a higher rate of comorbid panic disorder, suggesting that comorbid panic disorder can be a specific marker for a familial subtype of bipolar disorder. Contreraset al[4] found that the anxiety trait is a heritable phenotype in subjects with bipolar I disorder in a study of 619 individuals. In another study, relatives of patients with bipolar disorder and panic disorder comorbidity showed a higher risk of both bipolar disorder and panic disorder[5]. Many studies have found that panic symptoms are prodromal symptoms of bipolar disorder or atypical presentation of bipolar disorder[6,7]. In addition, Wuet al[8] compared neuropsychological test scores among a group of bipolar patients with comorbid anxiety disorder, a group of bipolar patients without comorbidity, and a healthy control group. They concluded that patients with bipolar II disorder and comorbid anxiety disorder had the greatest cognitive impairment among the three groups[8]. Moreover, the presence of anxiety disorder in youth increases the risk of bipolar disorder in the future[9].
The lifetime prevalence of panic disorder is approximately 21% of bipolar disorder, which is much higher than approximately 10% of major depressive disorder. Birmaheret al[10] found that panic disorder or bipolar disorder are likely to co-occur with other psychological disorders in youths. Moreover, patients with concomitant panic disorder and bipolar disorder have a higher risk of psychotic symptoms and suicidal ideation. In other studies, patients with panic disorder and comorbid bipolar disorder had higher rates of suicidal behaviors, severe and longer depressive episodes, higher severity of illness scores, poorer treatment outcomes, and lower quality of life[11-14]. In addition, they tend to have a higher risk of rapid switching and a shorter euthymic period[15,16]. Patients with bipolar disorder with high global anxiety levels developed a greater proportion of weeks in major depressive episodes[17]. Therefore, an early diagnosis of bipolarity in panic disorder patients is important to establish an appropriate treatment plan to improve the prognosis of patients.
Antidepressants are often used in the treatment of panic disorder, and it is well known that antidepressant-induced manic symptoms are quite common in such patients[11]. The lack of information regarding bipolar disorder comorbidity in patients with panic disorder can negatively impact the choice of treatment and management, which is the reason why an early diagnosis of bipolar disorder in patients with panic disorder is important in the treatment outcome of patients[7,11]. Previous studies have discussed the prognosis of bipolar disorder according to the presence of panic disorder[8,10-17], however, few studies have investigated bipolarity in patients with panic disorder[18,19]. The aim of this study was to compare clinical characteristics of panic disorder according to the bipolarity, and to investigate factors that predict the potential risk of bipolar disorder in patients with panic disorder.
MATERIALS AND METHODS
Study design and participants
This cross-sectional study was conducted in Konkuk University Hospital, Korea. A total of 254 consecutive patients, who were newly diagnosed with panic disorder according to the DSM-V (Diagnostic and Statistical Manual of Mental Disorders), were included in the study. The exclusion criteria include history of (1) Schizophrenia like psychosis; (2) Cognitive impairment due to dementia; (3) Intellectual disability; (4) A history of major neurological disorder; (5) Organic mental disorder; and (6) Substance use problem. This study was approved by the Institutional Review Board of Konkuk University Hospital (IRB number: KUMC 2021-01-028), and written informed consent was waived due to the retrospective nature of the study.
Instruments
Demographic data and psychological test results were also collected. Psychological tests included the Mood Disorder Questionnaire (MDQ), Panic Disorder Severity Scale (PDSS), Beck Depression Inventory (BDI), State-Trait Anxiety Inventory (STAI), Temperament and Character Inventory (TCI), and Minnesota Multiphasic Personality Inventory (MMPI).
MDQ, which was used as a screening tool for bipolar disorder, is a self-report instrument that takes approximately five minutes to complete. Patients with scores above the threshold score of 7 were considered as patients with bipolarity (BP+ group) and the remaining were considered as patients without bipolarity (BP- group). The Korean version of the MDQ (K-MDQ) was used in this study, and the validity and reliability of the questionnaire have been proven to be useful for screening bipolar disorder[20].
PDSS is a standard measurement scale for panic disorders. The instrument included seven items associated with symptoms accompanied by panic disorder[21,22]. This study used the Korean version of the PDSS, which has good test-retest reliability and inter-rater reliability[21].
The BDI-II is a self-report checklist for assessing the severity of depressive symptoms. The 21 items included emotional, physiological, and cognitive symptoms of depression. This study used the Korean version of the BDI-II, which is considered a valid and reliable tool[23].
The STAI is a 40-item self-report instrument used to evaluate anxiety symptoms. The State Anxiety Scale measures an individual’s current state of anxiety, and the Trait Anxiety Scale evaluates an individual’s stable tendency toward anxiety[24]. This study adopted the Korean version of the scale translated by Leeet al[21], which has demonstrated fine psychometric properties[24].
The TCI is a self-report questionnaire based on a biosocial personality model. Cloninger’s biosocial model of personality was used to develop the TCI questionnaire. The temperament, which is related to the biosocial model of personality, is composed of novelty seeking, harm avoidance, reward dependence, and persistence. The character is evaluated in three different aspects of a person’s characteristics: selfdirectedness, cooperativeness, and self-transcendence[25]. The Korean version of the TCI was used in the study. The Korean version of the TCI has been reported to be reliable for assessing personality[26].
The MMPI is commonly used in personality and psychopathology assessments of patients[27]. It contains 10 clinical subscale to evaluate personality and psychopathology of patients: hypochondriasis (Hs), depression (D), hysteria (Hy), psychopathic deviate (Pd), masculinity-femininity (Mf), paranoia (Pa), psychasthenia (Pt), schizophrenia (Sc), hypomania (Ma), and social introversion (Si). The Korean version of the MMPI-II was used in this study and has been reported to be reliable in assessing personality and psychological symptoms in Korean adults[28].
Statistical analysis
Kolmogorov-Smirnov test determined whether the data were normally distributed. The Mann-Whitney and chi-square test was conducted to compare demographic and clinical variables between the group with an MDQ score of less than 7 and the group with an MDQ score of 7 or more (BP+ group). The relationships between the MDQ scores and other psychological variables were analyzed using the Spearman’s rank correlation analysis and the logistic regression analysis. The statistical significance level was set atP< 0.05. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS 17.0) software (SPSS Inc., Chicago, IL, United States).
RESULTS
Table 1 presents the characteristics of the participants. The average age at diagnosis was 33.5 years (range, 18-68 years). There were more female (54.7%) than male participants, and most had at least a high school education. The mean score of K-MDQ was 6.4 ± 3.6 (range, 0-13). Half of the patients (n= 128) had high K-MDQ scores (≥ 7). The mean score of K-MDQ was 9.4 ± 1.7 in the BP+ groupvs3.4 ± 2.2 in the BP- group.
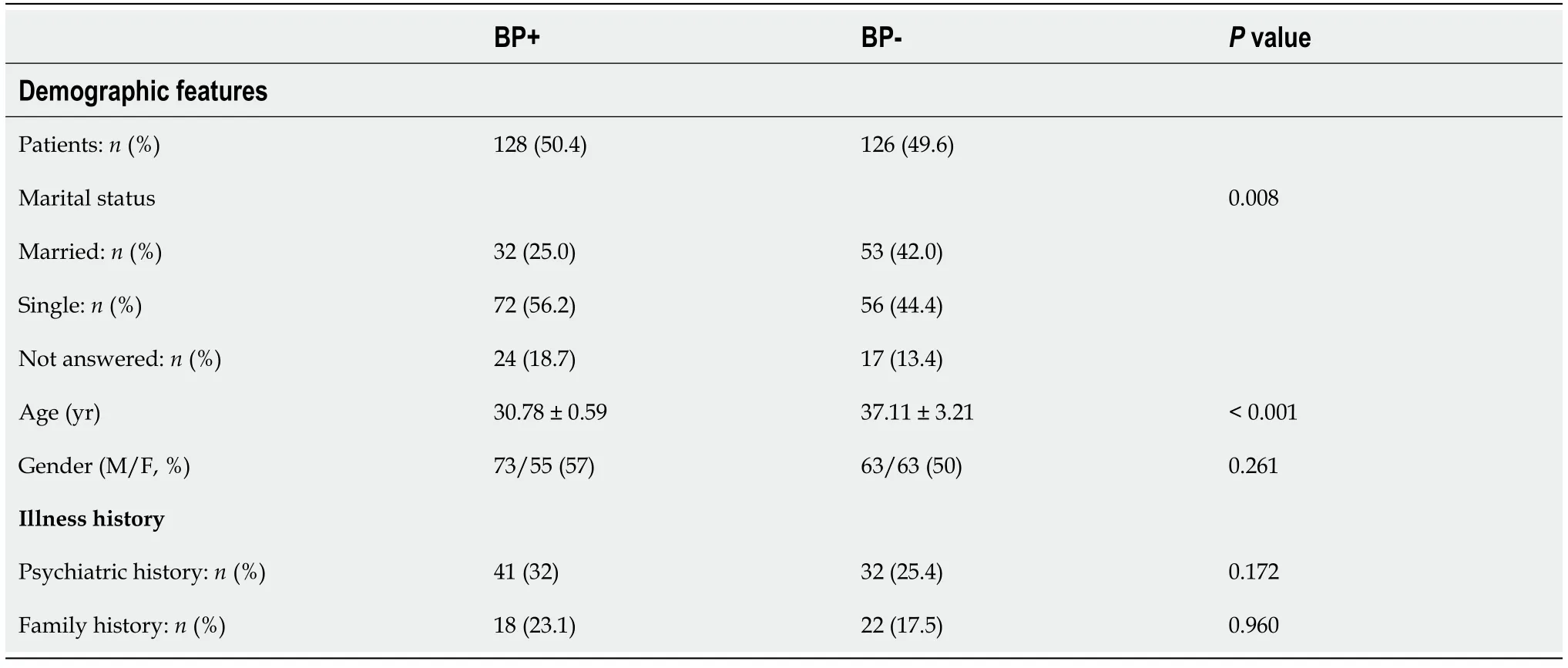
Table 1 Comparison of demographic and clinical features between panic disorder with bipolarity and panic disorder without bipolarity groups
Patients in the BP+ group were younger (30.78 ± 0.59vs37.11 ± 3.21) at the time of the diagnosis and were either unmarried or divorced (single 56.2%vs44.4%,P= 0.008) compared to patients in the BP-group. (Table 1) However, a gender, a past psychiatric history, and a family history of psychiatric disorders did not significantly differ between the two groups (Table 1). The BP+ group had significantly higher scores on the MMPI clinical scales. These clinical scales include hypochondriasis, psychopathic deviate, masculinity-femininity, psychasthenia, schizophrenia, and hypomania. In addition, BP+ group had significantly different scores in some TCI dimensions than BP- group. Compared to BP- group, BP + group had higher novelty seeking, harm avoidance, and self-transcendence scores, and lower self-directedness and cooperativeness scores. Moreover, the BP+ group also showed higher levels of depressive symptoms as measured by the BDI (31.5vs21,P< 0.001), and anxiety symptoms measured by STAI (state) and STAI (trait) (state: 63vs57,P< 0.001/trait: 61.5vs51.5,P< 0.001) (Table 2).
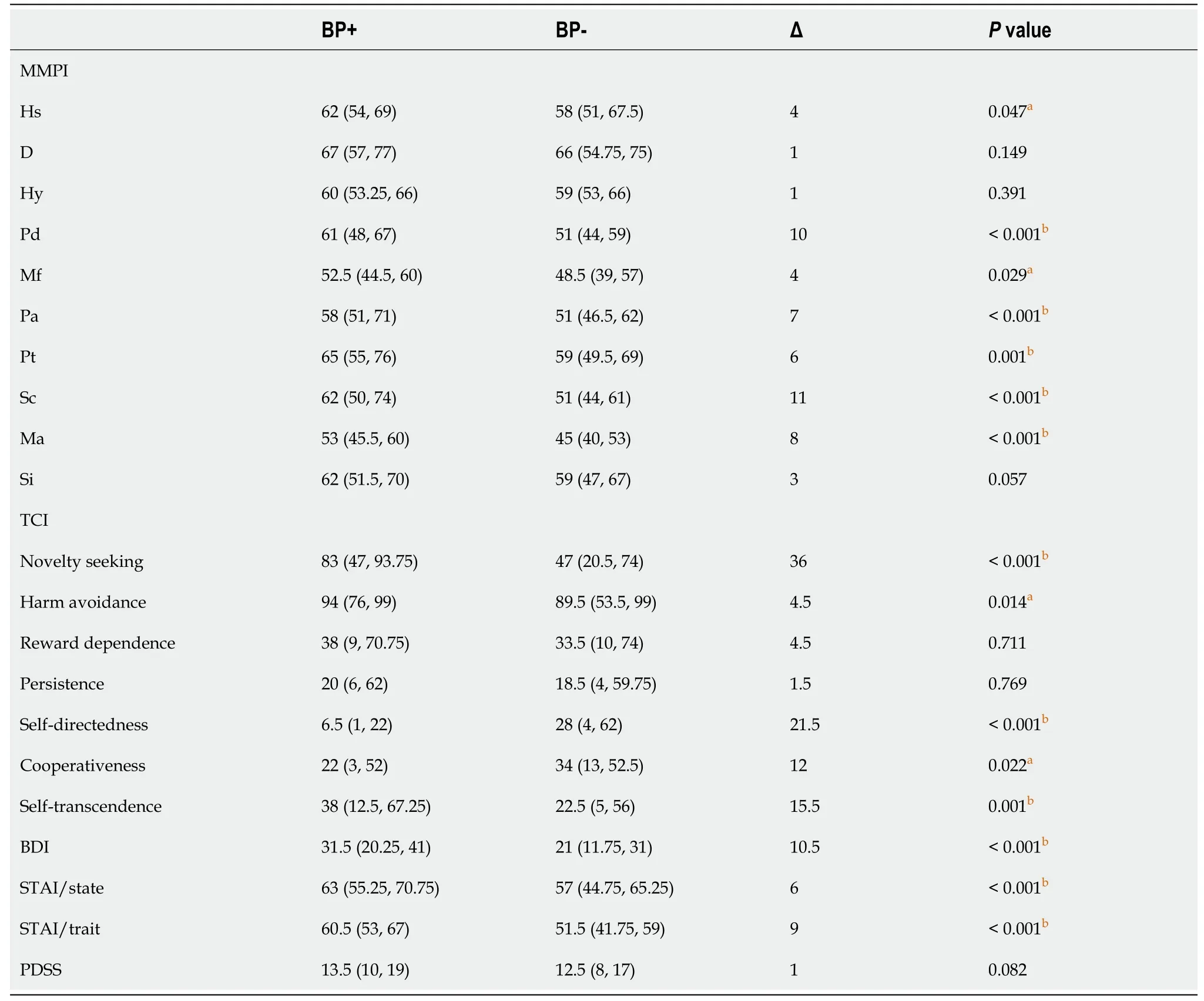
Table 2 Comparison of psychological test result between panic disorder with bipolarity and panic disorder without bipolarity groups
In correlation analyses (Table 3 and Supplementary Table 1), K-MDQ scores were associated with increasing Hs, D, Pd, Mf, Pa, Pt, Sc, Ma and Si in MMPI clinical scales, TCI novelty seeking, harm avoidance and self-transcendence dimensions, and higher BDI, STAI (state), and STAI (trait) scores. K-MDQ scores were negatively associated with TCI self-directedness dimension scores (P< 0.05).
This study used logistic regression analysis to assess the association of K-MDQ and clinical variables, and the age at onset, MMPI (depression), MMPI (hypomanic), TCI (self-directedness), and STAI (trait) were found to be significantly associated with bipolarity in patients with panic disorder (Table 4). Younger age was significantly associated with an increased K-MDQ score (BP+ group). Moreover, in the MMPI and TCI questionnaire, as the MMPI (depression) and TCI (self-directedness) clinical scales decreased, K-MDQ scores increased. In addition, the increase in MMPI (hypomanic) clinical scale scores was significantly associated with the BP+ group (bipolarity of patients). The patients who showed an innate trait of anxiety tested by STAI (trait) tended to be more related to high K-MDQ scores (BP+ group).
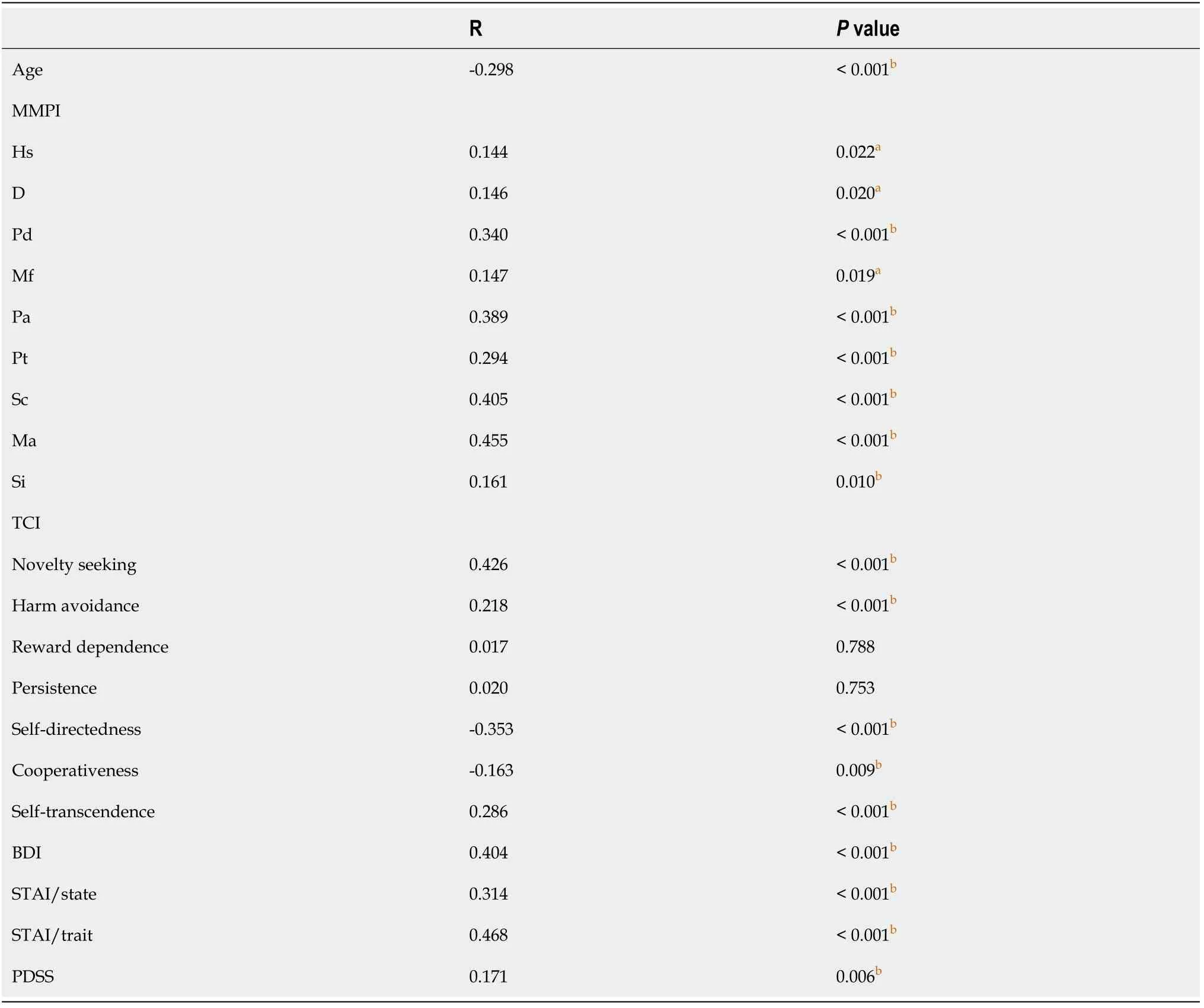
Table 3 Correlation analyses between Korean version of the Mood Disorder Questionnaire score and other measured variables
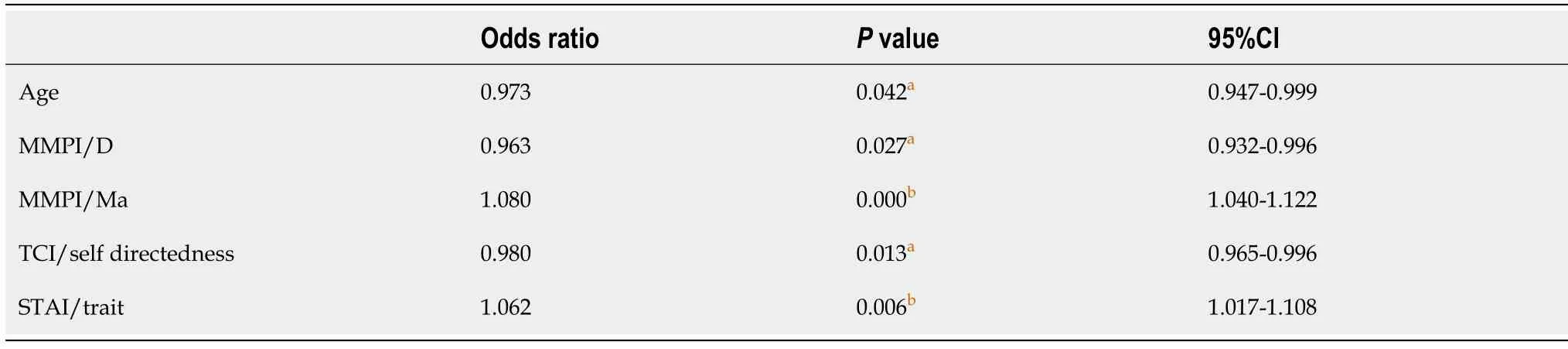
Table 4 Logistic regression analysis showing the association of panic disorder with bipolarity group (Korean version of the Mood Disorder Questionnaire score ≥ 7) with clinical variables
DISCUSSION
Among the 254 subjects who were diagnosed with panic disorder, approximately 50% of the patients scored 7 or more on the K-MDQ, suggesting a history of manic/ hypomanic symptoms in the past. Younger age and the Ma subscale of the MMPI were associated with the higher risk of bipolarity. In addition, the STAI (trait) score, which indicates the innate anxiety level, is positively related to the bipolarity of panic patients, while the self-directedness score in the TCI was negatively associated.
In line with our data, in a previous study, an early age at onset of panic disorder was associated with an increased morbidity risk for bipolar comorbidity[29]. In addition, an early onset of bipolar spectrum disorders is characterized as a severe form of bipolar disorder and tends to have a higher risk of having first-degree relatives with affective disorders[29]. In this study, the patients with bipolarity showed a younger age at onset, which has been found in previous studies[18,30]. Moreover, a previous study has already shown that the risk of anxiety disorder increases as the onset age of bipolar disorder decreases[31]. So, it would be important to evaluate bipolarity thoroughly in younger panic disorder patients in clinics. In our study, patients with a bipolar tendency were more likely to be unmarried at the time of assessment. In previous investigations, bipolar patients had a higher risk of experiencing difficulties in marriages, which is also shown in this study[18,32].
Several psychometric tests have been developed to help diagnose psychiatric patients and the MMPI is one of the most commonly used standardized psychometric tests of adult personality and psychopathology[33]. It is well known that the MMPI Ma subscale is used to identify manic symptoms of individuals at the time of evaluation[34]. In our study, it was found that MMPI hypomanic subscale scores were positively correlated with bipolarity in patients with panic disorder. The result of this study was consistent with previous studies, stating that the high score of hypomanic subscale is indicative of diagnosis of bipolar disorder[35,36]. Higher Ma score in MMPI indicates that patients with panic disorder and bipolarity experience more physical and psychological vitality; however, they also experience dissatisfaction, tension, and anxiety in life[36]. In addition, patients with panic disorder and bipolarity felt less depressed compared to patients without bipolarity, which results from the nature of bipolar disorder manic symptoms.
Engströmet al[37] conducted a study with 100 euthymic bipolar patients and 100 controls from the normal population to determine the differences in temperament and character of each group. They showed that bipolar patients scored higher in harm avoidance and lower in reward dependence, self-directedness, and cooperativeness in TCI than controls[37]. In addition, in a previous study focusing on the relationship between temperament and panic disorder, high scores of harm avoidance, and reward dependence were related to panic symptoms[38]. The results of our study were consistent with those of a previous study indicating that patients with bipolarity showed a negative relationship with self-directedness scores in the TCI test. This result suggests that panic disorder patients with bipolarity are more likely to be aimless and inept than panic disorder patients without bipolarity. The TCI harm avoidance, reward dependence, and cooperativeness scores did show some correlation with bipolarity based on our correlation analyses, but not in our regression analysis. This suggests that a lower self-directedness score can be used as a marker to predict bipolarity in patients with panic.
In this study, the STAI (trait) score was positively related to the bipolarity of patients with panic disorder. High levels of anxiety were positively correlated with bipolarity, particularly when having anxious characteristics in patients with panic disorder. Bipolarity was more related to the anxious characteristics of patients than to the current anxiety levels. In other words, patients with higher anxiety levels and anxiety sensitivity were more likely to be diagnosed with bipolar disorder in the future. Anxiety sensitivity is known to be a contributing factor to the high prevalence and severity of panic disorder comorbid with bipolar disorder, particularly during the manic state of bipolar disorder, as our study has suggested[19]. Contreraset al[39] found a significant positive correlation between trait anxiety score and mania episodes in lifetime. However, there was no correlation between trait anxiety scores and lifetime depressive episodes. Azorinet al[40] also stated that an irritable temperament is a source of mood instability and stress, which interacts with other temperamental characteristics to induce both anxiety and bipolar symptoms. In addition, studies have shown that when the level of anxiety sensitivity is high, the prognosis of patients with bipolar disorder is worse and panic disorder symptoms are more severe[7,19,41,42]. Therefore, it is important to make an evaluation about panic disorder patients’ anxiety sensitivity to diagnose bipolar disorder for a better prognosis.
This study has several limitations. First, this study was a cross-sectional, retrospective study with relatively small number of participants. We included consecutive patient who were clinically diagnosed with panic disorder based on the strict diagnostic criteria. However, the study design may be related to the selection bias and hinder the generalizability of the results. Second, even though we have consulted a biomedical statistician to confirm the proper statistical method to use in the study, there is a possibility of type I error because thePvalue was not corrected in the multiple comparison. Finally, a self-report questionnaire was used to evaluate the bipolarity. The MDQ is a validated questionnaire for evaluating manic/hypomanic symptoms in patients with various psychiatric conditions, however, clinicians did not confirm the history of manic/hypomanic symptoms of the participants in this study.
CONCLUSION
In this study, we were able to predict bipolarity in panic disorder patients through simple self-report questionnaires, which have been widely used. Early diagnosis of bipolarity in patients with panic disorder will have a positive effect on the patient's treatment outcome. It should be noted that among patients with panic disorder, patients with an anxious personality have a high comorbidity rate for bipolar disorder. Based on the results of this study, it is possible to detect bipolarity in advance through a simple questionnaire in actual clinical practice.
ARTICLE HIGHLIGHTS
Research background
Panic disorders frequently occur with affective disorders, particularly bipolar disorder.The lifetime prevalence of panic disorder is about 21% of bipolar disorder, much higher than about 10% of major depressive disorder. Patients with panic disorder and bipolar disorder are more likely to present with a severe course of disorder, such as high rates of suicidal behavior, poor symptomatic and functional recovery, and poor drug responses.
Research motivation
Patients who suffer from both panic disorder and bipolar disorder have a poorer prognosis than patients who suffer from only one disorder. So, it is crucial to predict a bipolarity of a patient who is diagnosed with panic disorder at early phase of disease course to select a proper treatment for the patients. However, there is no standard evaluation tool to predict a bipolarity of panic disorder patients.
Research objectives
In this study, we tried to identify the specific symptoms of patients with panic disorder that indicate bipolarity to establish a proper treatment plan.
Research methods
A total of 254 patients (136 men and 118 women, mean age = 33.48 ± 3.2 years) were diagnosed with panic disorder. Panic disorder with bipolarity (BP+) was defined as a score of ≥ 7 on the Korean version of the Mood Disorder Questionnaire (K-MDQ), and a score lower than 7 was considered a panic disorder without bipolarity (BP-). Selfreport questionnaires were analyzed to examine their association with bipolarity.Psychological tests included the Mood Disorder Questionnaire (MDQ), Panic Disorder Severity Scale, Beck Depression Inventory, State-Trait Anxiety Inventory (STAI),Temperament and Character Inventory (TCI), and Minnesota Multiphasic Personality Inventory (MMPI). Statistical analyses were performed to evaluate the correlation between panic disorder and bipolarity. Our collected data was not normally distributed. So, for statistical analysis, we used Mann-Whitney test to compare continuous variables between two groups, and Spearman’s rank correlation to find the relationship between the MDQ scores and other variables.
Research results
Patients with a K-MDQ score of 7 or more were considered to have a history of manic or hypomanic episodes (BP+ group,n= 128), while patients with K-MDQ scores below 7 were defined as those without bipolarity (BP- group,n= 126). The BP+ group were more likely to be unmarried (single 56.2%vs44.4%,P= 0.008) and younger (30.78 ± 0.59vs37.11 ± 3.21,P <0.001). Moreover, the BP+ group had significantly higher scores on some psychological assessment scales, such as the hypochondriasis, psychopathic deviate, masculinity-femininity, psychasthenia, schizophrenia, and hypomania (Ma) in MMPI, and novelty seeking, harm avoidance and self-transcendence in TCI, and STAI (state and trait) compared to the BP- group. In logistic regression analysis, MMPI (depression), MMPI (paranoia), and age were negatively associated; however, MMPI (Ma) and STAI (trait) were positively associated with the BP+ group (K-MDQ score ≥ 7). In addition, BP+ was positively associated with current manic symptoms (1.080,P= 0.000) and trait anxiety (1.062,P= 0.006), and negatively associated with current depressive symptoms.
Research conclusions
The result of this study suggests that MMPI, TCI and STAI can be used to predict the bipolarity of panic disorder patients. These psychological assessments can be considered to performed in clinics to establish proper treatment plans for a better prognosis.
Research perspectives
Further investigations should aim to assess the validity of specific psychological factors to be used to detect bipolarity in panic patients prospectively.
杂志排行

World Journal of Psychiatry的其它文章
- Current global research landscape on COVID-19 and depressive disorders: Bibliometric and visualization analysis
- COVID-19 impact on high school student’s education and mental health: A cohort survey in China
- Brain reward circuitry: The overlapping neurobiology of trauma and substance use disorders
- Intimate partner violence: A loop of abuse, depression and victimization
- How do serotonergic psychedelics treat depression: The potential role of neuroplasticity