Uncertainty following an inconclusive result from the BRCA1/2 genetic test: A review about psychological outcomes
2022-01-08SoniaMoniqueBramantiCarmenTrumelloLuciaLombardiAlessandraCavalloLiborioStuppiaIvanaAntonucciAlessandraBabore
Sonia Monique Bramanti, Carmen Trumello, Lucia Lombardi, Alessandra Cavallo, Liborio Stuppia, Ivana Antonucci, Alessandra Babore
Sonia Monique Bramanti, Carmen Trumello, Lucia Lombardi, Alessandra Cavallo, Liborio Stuppia,Ivana Antonucci, Alessandra Babore, Department of Psychological, Health and Territorial Sciences, School of Medicine and Health Sciences, University “G. d’Annunzio”, Chieti 66100,Italy
Abstract BACKGROUND An inconclusive result from BRCA1/2 genetic testing indicates that a genetic variant of uncertain significance is detected. This case constitutes the majority of genetic test results, but studies specifically addressing the psychological adjustment of people with inconclusive results are scarce.AIM To examine psychological outcomes of receiving an uninformative BRCA1/2 test result.METHODS PubMed, PsychInfo, and Cochrane Central Register of Controlled Trials were screened for studies focusing on distress, anxiety, and depression levels in individuals with inconclusive genetic test results. This review is based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses method.RESULTS Studies on psychological outcomes of inconclusive BRCA1/2 focused on general and specific distress, anxiety, and depression. Overall, they produced mixed results. These inconsistent findings are probably due to the uncertainty caused by this type of result, that may also influence the decisions of individuals about surveillance and prophylactic options, reducing their compliance. In addition, this review highlights specific risk and protective factors that affect psychological adjustment in individuals with an inconclusive genetic testing result.CONCLUSION Individuals with inconclusive genetic test results need specific educational programs and support to better understand the meaning of their results in order to be able to make decisions about surveillance and prophylactic options.
Key Words: Genetic testing; BRCA1/2 mutation; Inconclusive result; Psychological distress; Depression; Anxiety; Review
INTRODUCTION
In the context of breast and ovarian cancer surveillance, genetic screening for the detection of mutations inBRCA1(chromosome 13) andBRCA2(chromosome 17) genes is a significant advance in cancer care. Each individual carries these two genes, which are responsible for the control and repair of DNA alterations; however, in their mutated form, they are linked to an increased risk of tumor development[1]. These genes are characterized by autosomal dominant inheritance, so one parent has a 50% chance of transmitting them to their children[1,2]. The lifetime risk of developing breast cancer in the general population ranges from 10%-14%, and this risk rises to 85% in women who carry a mutation in theBRCA1andBRCA2genes[2,3].
For individuals with high cancer history, genetic counselling is proposed. Medical and family histories are collected, and if there is at least 10% likelihood, a buccal smear or a blood sample is taken. The possible test results are positive, negative, or inconclusive[4]. The first one implies that the individual is a carrier of a mutation with an increased risk of developing cancer during his life. A negative result means that the individual is not a carrier of mutation, so he has the same probability of developing cancer as the general population. An inconclusive result produces a more complex situation, as it means that a deleterious mutation is neither identified nor definitively excluded. This may be due to two main reasons: (1) No known BRCA1/2 mutations were found, but a genetic variant of uncertain significance is detected; and (2) Not detecting a mutation in a cancer-affected person who is the first member tested (proband) in a high-risk family[5,6]. In the current review we indistinctly use the terms “inconclusive” and “uninformative” to refer to both the aforementioned situations. Though the inconclusive case constitutes the majority of genetic test results[1,7], research and clinical attention is lacking in this topic, as stated by several authors[5,8].
Undergoing genetic testing and its results can produce a significant psycho-social impact[2,9]. Generally, individual who receives a positive test result reports higher levels of distress, anxiety, and depression[10] while who receives a negative test result reports a decrease in distress levels following the discovery of test results[11]. A recent review of existing literature[12] highlighted that a positive genetic testing results can be traumatic, although not all individuals with such a result experience increased distress. The high distress levels experienced by individuals who receive a positive test results may depend by an increased risk of future diseases and the implications for their whole family[12]. A study highlighted that a possible factor that influences affective states is the perceived risk of developing cancer, regardless of test result[13]. Overall, higher levels of distress, anxiety and depression could depend by some risk factors as having a cancer diagnosis, having a greater history of breast/ovarian cancer, being younger than 40 years old, being unmarried and having high pre-test levels of anxiety and depression[12].
As for those who receive an inconclusive result, the literature is conflictual; some studies identify higher levels of distress in those with an inconclusive result[14] while other studies found that individuals who receive an inconclusive result seem reassured[15]. However, as stated by several authors[12,16], studies specifically addressing psychological adjustment of people with inconclusive genetic test results are scarce. According to Vadaparampilet al[8], this gap should be filled, as the topic of inconclusive test results is a key topic deserving clinical and research attention.
Starting from these premises, the main purpose of the current review was to investigate short-, intermediate-, and long-term consequences of receiving uninformative BRCA1/2 test results. To pursue this aim, we analyzed cross-sectional and longitudinal studies which examined anxiety, depression and distress in individuals who receive inconclusive results compared to positive and negative results. In addition, we aimed to highlight risk and protective factors that affect psychological adjustment in individuals with an inconclusive genetic testing result, also considering differences associated with being or not affected by a cancer diagnosis.
MATERIALS AND METHODS
Identification and selection of studies
This systematic review followed the guidelines of Preferred Reporting Items for Systematic Review and Meta-Analyses[17].
We conducted a comprehensive literature search in PubMed, PsychInfo, and Cochrane Central Register of Controlled Trials. All search results were limited to the last 21 years (1999-2020).
We combined search terms related to genetic counselling and its result [(Genetic*, Familial*, OR Mutation*) and (Inconclusive OR Uncertain) and (Breast* OR BRCA*)] with terms relating to psychological outcomes (Psycho*, Distress, Emot*, Anxiety, OR Depression). The reference sections of previous reviews were also checked to ensure that all relevant studies for this review were included.
Selection of eligible articles
Studies were included if they: Analyzed psychological outcomes of receiving an uncertain result; included adult, human subjects; and were written in the English language.
Exclusion criteria were: Articles not specific to BRCA mutation; articles not reporting psychological outcomes; articles that assessed the impacts of genetic counselling before subjects received genetic test results; and literature reviews, qualitative studies, commentaries, letters to the editor, unpublished articles and doctoral theses, abstracts of conferences, congresses, books, and case-reports.
Following the review by Hamiltonet al[18], we defined short-term as within 1 mo of genetic testing results, intermediate term between 1 and 6 mo, and long-term over 6 mo.
The eligibility criteria were evaluated according to the following aspects: Participants, intervention, comparison, outcome, and study design. (1) Participants: Human adult participants receiving an uncertain result from genetic testing about the presence of BRCA mutation; (2) Intervention: The focus was not limited on a specific intervention; (3) Comparison: Studies comparing people with inconclusive genetic test results to positive and negative results; (4) Outcomes: We analyzed studies that considered short- (1 mo), intermediate- (1-6 mo), and long- (6+ mo) term psychological outcomes (i.e., general and specific distress, anxiety, and depression); and (5) Study design: We included observational and/or quantitative studies.
Anxiety, depression, and distress (both general and specific) have been the focus of the review as they were the outcome measures most frequently evaluated.
RESULTS
A total of 341 studies were identified; of those, 174 were removed as duplicates. The titles of the selected studies were double screened by two authors independently, 66 studies were excluded because they were not consistent with the eligibility criteria. The abstract of 101 selected studies and the full text of all potentially relevant articles were double screened and evaluated by two authors independently; discrepancies were resolved by discussion; the following were excluded: 11 were reviews, 46 did not focus on psychological variables, 23 studies involved a sample with a different genetic mutation from BRCA or did not focus on inconclusive results, and 11 had an inadequate study design (qualitative studies, unpublished articles, case-reports, books or abstracts of congresses). A total of 10 articles met our inclusion criteria and were, therefore, considered in this systematic review (Figure 1). Included studies were published between 2002-2017 and were most commonly conducted in the United States, followed by Canada and the United Kingdom. Eight studies were longitudinal (80%) and two were cross-sectional (20%). All the included studies were classified on the basis of the timing of questionnaire administration; most studies (n= 7) assessed also baseline levels of psychological measures before the blood test or buccal smear test.
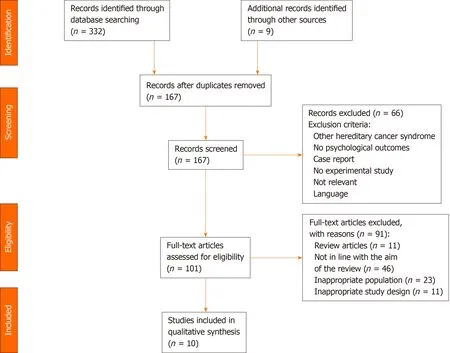
Figure 1 Flow chart of selection and inclusion process, following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement.
Only one study considered exclusively short-term psychological outcomes, four studies only intermediate-term, and three studies long-term (Table 1). Sample sizes from the reviewed studies ranged from 48 to 465 (mean = 193.30, standard deviation = 135.14), resulting in a total of 1933 participants. Of these, 38% (n= 730) received inconclusive test results, 32% (n =620) received negative results, 21% (n =408) received positive results, 7% (n =126) decided not to undergo genetic testing, and 2% (n =49) were still waiting for their test results. Only two studies included male participants; the sample was predominantly female (98%).
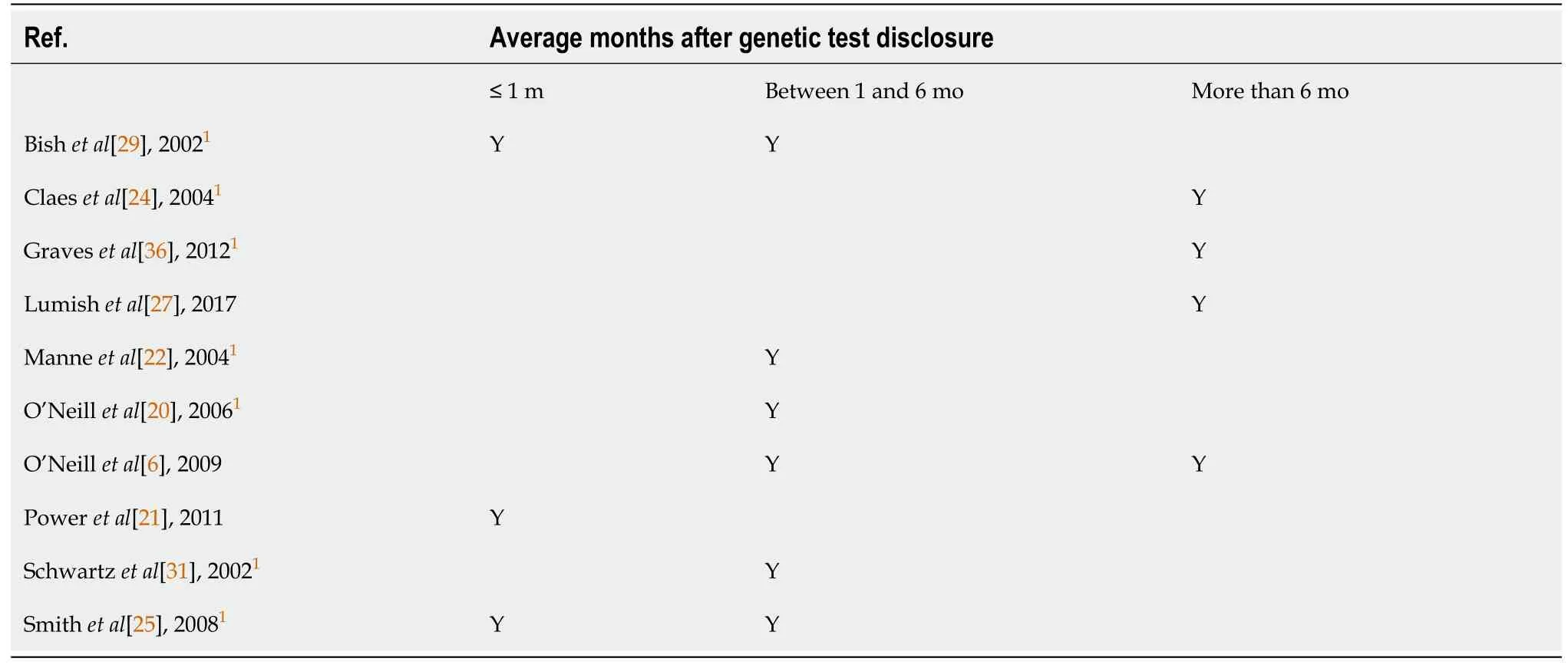
Table 1 Time of psychological outcome measures after genetic test disclosure
Of the reviewed articles, six studies compared people with and without a cancer history. The majority of the sample (73%) had a cancer diagnosis. Only four studies reported the type of cancer diagnosis; of these, 94% had breast cancer, 4% had ovarian cancer, and 2% had both.
Outcome measures of the included studies
The findings were divided into four categories: (1) General distress; (2) Anxiety; (3) Depression; and (4) Genetic testing-specific distress. The tools used for the evaluation of each construct are synthesised in Table 2.
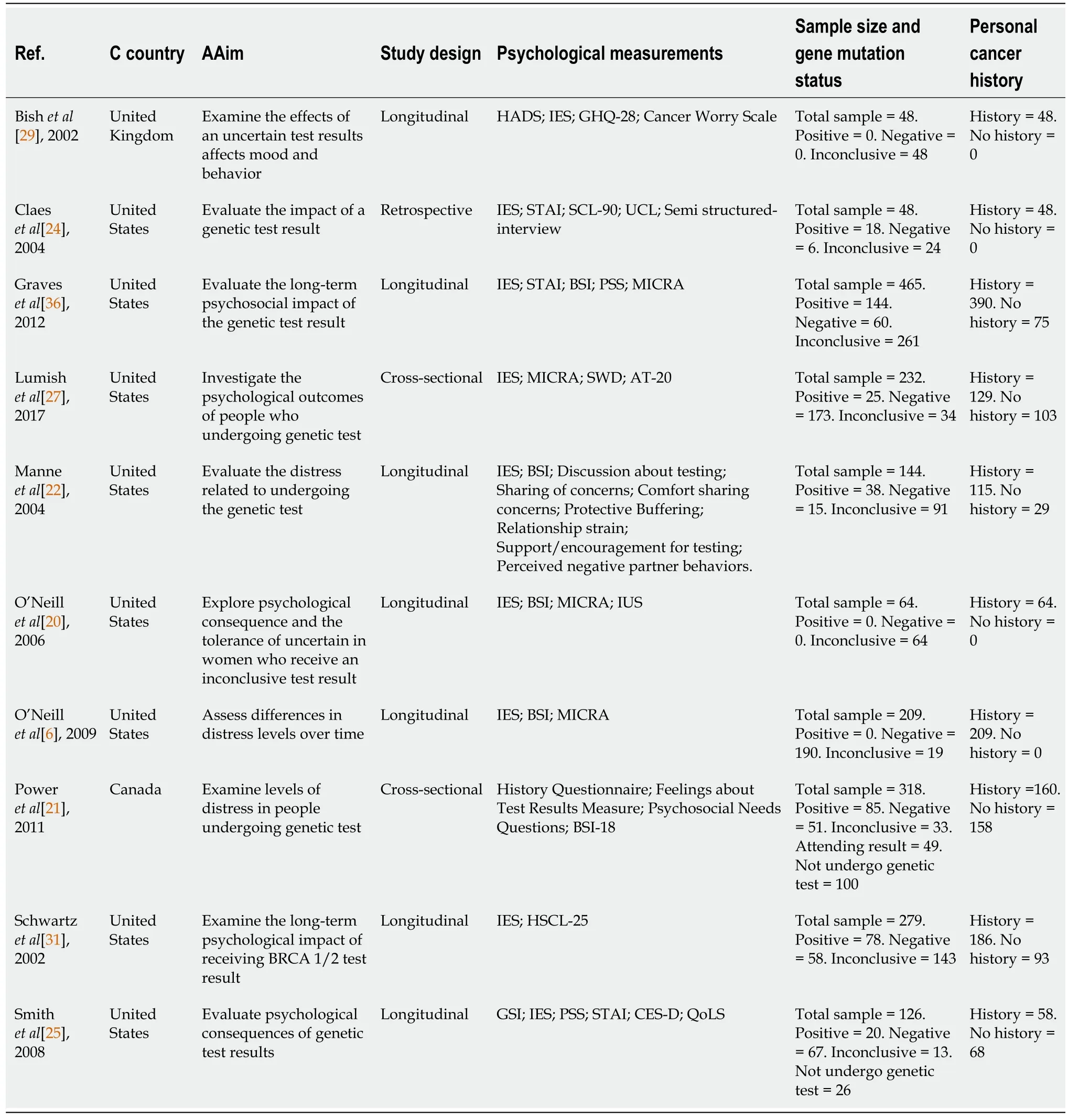
Table 2 Characteristics of included studies
The Brief Symptoms Inventory (BSI)[19-22], the Symptom Checklist 90 Revised (SCL-90)[23-25], the Impact of Event Scale[26,27], the General Health Questionnaire[28,29], and the Hopkins Symptom Checklist[30,31] were used to assess general distress symptoms. Depressive symptoms were assessed using the BSI[6,19,20], the SCL-90[23,24], the Hospital Anxiety and Depression Scale (HADS)[29,32], and the Center for Epidemiologic Studies Depression Scale[25,33].
The BSI[6,19,20], the SCL-90[23,24], the HADS[29,32], and the State Trait Anxiety Invento-ry[25,34] evaluated anxiety symptoms.
Finally, genetic testing-specific distress was evaluated by means of the Multidimensional Impact of Cancer Risk Assessment[6,20,27,35,36].
General distress
The majority of the reviewed studies did not find significant differences in psychological adjustment among individuals who received inconclusive, positive and negative results[22,24,25,29,31]. One study observed higher levels of distress, especially on the somatization scale, in those who received inconclusive results compared with positive and negative results, and people deciding not to undergo genetic testing[21]. Instead, a recent study of Lumishet al[27] highlighted that individuals receiving an inconclusive result reported intermediate levels of general distress, higher than negative but lower than positive result.
Schwartzet al[31] did not find increased levels of distress in people with inconclusive results compared to positive and negative results, but they did not identify a decrease in distress levels in the intermediate-term (i.e., 1-6 mo) in individuals with inconclusive results, which occurs in those who receive negative results. Two studies found that general distress decreased slightly over time, from pretest to 6 mo post-test[20,25]. Other studies reported that there were no differences in distress levels from pre-test levels up to 6 mo after genetic test disclosure[22,29].
Regarding differences between cancer affected patients and unaffected patients, overall, unaffected patients with positive or inconclusive results reported higher levels of distress compared to both affected patients and unaffected patients with negative results[27]. Other studies highlighted that having had a cancer diagnosis did not influence distress levels; in fact, they did not detect differences between affected and unaffected patients[21,22,25].
In addition to genetic test results, other factors which could increase distress levels in those who receive an inconclusive result may be a cancer diagnosis[27], higher distress levels before genetic testing[25], the intolerance of uncertainty[20], and cancerrelated distress[20].
However, there are also some protective factors that could mitigate or decrease distress levels such as marital status[20], partner support, and protective buffering[21].
Anxiety
None of the reviewed studies found differences in anxiety levels among individuals with inconclusive, positive and negative results[24,25,29] except for one study that found that patients with inconclusive results reported higher levels of anxious symptoms after test result disclosure than negative ones[6].
Some studies observed anxious symptoms in the intermediate-term[25] and longterm[6,29]. Two studies of these did not find changes in anxiety levels in the intermediate-term[25,29], while O’Neillet al[6] detected a decrease in anxiety over time for individuals who received negative test result and stable levels of anxiety in those who received inconclusive results from the discovery of the test result up to 6 mo later, with a subsequent decrease.
Only one of the reviewed articles that focused on anxiety investigated whether there were differences among affected and unaffected patients and found that there were no differences between them[25].
Overall, some factors that could influence anxiety levels in individuals who receive an inconclusive test results, might be: Higher distress levels before genetic testing[25], higher pre-testing anxiety[6], correctly interpreting the meaning of the genetic test result[24,29], primary appraisal, namely the way people evaluate the importance of a stressful situation[6], and ethnicity[6].
Depression
Four of the included studies focused on depression[6,24,25,29]. The majority of the reviewed studies did not identify differences between those receiving inconclusive, positive and negative results[24,25,29].
Two studies did not identify effects of time on depression in the intermediateterm[25,29]. Only one study analyzed long-term outcomes (6 mo), highlighting that depressive levels were significantly higher in individuals receiving inconclusive results compared to negative[6].
Having received a cancer diagnosis did not influence depressive levels, regardless of the test results[25]. Other factors could influence depressive levels among individuals who receive an inconclusive test result: Misinterpretation of test results[24,29], pre-test depressive levels[6,25], primary appraisal[6], and ethnicity[6].
Genetic testing-specific distress
Four of the included studies focused on genetic testing-specific distress[6,20,27,36], which was assessed only after genetic test disclosure. All the reviewed studies measured specific distress in the long-term[6,27,36] except for one study that assessed it in the intermediate-term[20].
Two studies found that inconclusive results were associated with lower levels of genetic testing-specific distress than positive test results[27,36] but higher than negative results[27,36].
Higher levels of genetic testing-specific distress were observed from 1-6 mo and 1 year after genetic test disclosure[6,20,36]; specifically, individuals with inconclusive results reported higher levels of specific distress persisting even 1 year after test disclosure[6]. O’Neillet al[6] detected that distress levels among inconclusive results stayed stable over time and decreased among negative results.
Individuals affected by cancer who receive inconclusive results showed higher levels of distress related to genetic testing than unaffected individuals with inconclusive results, affected carriers, and both affected and unaffected noncarriers[27]. On the contrary, Graveset al[36] identified that mutation carriers with a cancer diagnosis had higher levels of distress than affected individuals with uncertain results.
In general, some potential risk factors that could influence genetic testing-specific distress in individuals who receive an inconclusive result are higher pre-test perceived risk[6,20], lower education level[27,36], younger age[27,36], ethnicity[6,36], lower genetic knowledge[27], coping with uncertainty[20], confusion regarding the interpretation of test results[27], pre-test distress[6,36], pre-test anxiety[36], and stronger levels of primary appraisal[6]. Some protective factors, such as being married[36] and stronger secondary appraisal[6], can reduce distress related to genetic testing.
DISCUSSION
The main purpose of the current review was to investigate the consequences of receiving inconclusive results from BRCA1/2 genetic testing on psychological outcomes such as general distress, anxiety, depression, and genetic testing-specific distress. To our knowledge, our review is the first to explore the short-, intermediate-, and long-term psychological effects of receiving inconclusive results in both affected and unaffected patients, as previous reviews were mainly based on individuals who receive a positive or a negative result[12,13,37]. From the analysis of the selected articles, overall different results were found.
Most studies (five of the ten considered) did not report differences in levels of general distress, anxiety, and depression among individuals with inconclusive results, as compared with both positive and negative results[22,24,25,29,31]. Other studies have found that those who receive inconclusive results experience higher levels of general and specific distress, anxiety, and depression than who have a negative result[6,27,36], but lower than positive ones[27,36]; and finally, a study identified that the inconclusive results caused greater levels of general distress when compared with both positive and negative results[21].
The differences detected from the reviewed studies might depend on the different tools used to assess distress, anxiety, and depression, which might not be sufficiently sensitive in this field[12]. As evidenced by a study by Poweret al[21], individuals with an uninformative BRCA1/2 test result reported higher levels of distress, specifically in the somatization scale, so it could be that this subgroup of patients experienced distress through the body. Hence, it could be useful to develop more sensible tools, specifically addressing this field.
Although no differences were found between negative and inconclusive results, there was no decrease over time in the levels of distress, anxiety, or depression, which instead occurred in individuals with a negative result[6,31]. A possible explanation for these results might be the lack of relief from this type of test result[16] and having to copy with the uncertainty[21,24,29,38,39]. Indeed, individuals who have difficulty in coping with uncertainty have higher levels of ongoing distress[20]. The uncertainty related to this type of result also influences the decisions of individuals about surveillance and prophylactic options; only a fraction of patients who receive this type of result decides to increase cancer screening[27]. Moreover, some patients determine not to carry out preventive surgery, as they need a more certain result before deciding on this irreversible option[24], from which psychological benefits might be derived due to the cancer risk decrease[40], or it can also lead to adverse psychological impacts and dissatisfaction[41-43]. Graveset al[36] identified that having prophylactic surgery does not reduce distress levels but only the perceived risk of developing cancer.
Two studies showed that individuals with a cancer diagnosis have greater levels of distress, anxiety, and depression than those without a previous cancer diagnosis[27,36]; in the group of affected people, being mutation carriers[36] or having received an inconclusive result[27] were associated with a worse psychological adjustment. Patients with a recent cancer diagnosis could represent a population more vulnerable to higher levels of distress, anxiety, and depression due to the impact of the diagnosis and its treatment[44,45]. Other studies did not find differences between affected and unaffected patients[20,25,31]. A possible explanation for these inconsistent results could be the psychological benefit that affected patients derived from genetic testing[12,37], because medical surveillance protocols make the process predictable and understandable[37]. Due to this, affected patients and individuals who receive a positive test result might be better able to cope with this situation than individuals who have to cope with the uncertainty[20,46,47].
Apart from having had a cancer diagnosis[27,36], other factors that influence the psychological outcomes related to genetic test disclosure also emerged from the current review. Among the major risk factors are: Higher pre-test levels of distress and anxiety[6,24,25,31], younger age[6,22,27,36], correctly interpreting the meaning of the test result[24,29], intolerance of uncertainty[20], use of the primary appraisal[6], higher perceived risk before genetic testing[6,20], having a family history of cancer[25,36], lower education level[27,36], lower genetic knowledge[27], having children[36], lower income[36], and belonging to a minority ethnicity[6]. Regarding appraisal, it consists in the evaluation of the relevance of a stressful event such as genetic testing and/or cancer diagnosis[48,49]. Some studies have shown that different coping and evaluation strategies influence distress and stress levels; using a higher primary appraisal and emotional suppression are associated with higher levels[50,51], while increased use of secondary appraisal and cognitive reappraisal are associated with better psychological outcomes[50,52].
In addition to secondary appraisal and cognitive reappraisal, other factors could decrease distress levels such as being married[20,36], having partner support[22], having a bilateral salpingo-oophorectomy[36], and protective buffering[22].
This review revealed that those who receive inconclusive results are a subgroup of patients who need educational programs and more pre-test information to better understand the meaning of their test so they can make decisions about surveillance and prophylactic options.
This literature review has some limitations. First, only a few studies were included in this review because the majority of studies focus on the psychological outcomes of those who receive positive or negative results, although inconclusive results are the most common[1,7]. Another limitation is that the studies we analyzed included different standardized measures concerning distress, anxiety, and depression. It could be that these standardized tools are not sufficiently sensitive in this field and that those who receive positive, negative, and inconclusive results experience emotional distress differently. Moreover, the sample is unbalanced, as some studies exclusively include patients affected by a cancer diagnosis, a factor that contributes to experiencing higher levels of distress, anxiety, and depression. Finally, there was high variability between the time elapsed from the genetic test to the administration of the psychological questionnaires among the reviewed articles, and not all the reviewed studies administered the questionnaires at the same time to all patients. These limitations lead us not to generalize our results.
CONCLUSION
The results of this systematic review give a fuller picture of the psychological impact of receiving inconclusive results and can help genetic counsellors, health professionals, and researchers to provide more support to this subgroup of patients, by providing adequate information about the meaning of inconclusive genetic test result and its implications in terms of risk to develop cancer. The present review could also be able to improve the knowledge of experiences related to coping with uncertainty, suggesting which are the psychological aspects to consider when working with this type of patients. There is still much to understand in this difficult context, and it is necessary to take into greater consideration those who receive inconclusive results in the research and pre-test and post-test educational program to fully explain to people that inconclusive results do not exclude the possibility that they still might face a higher risk of developing ovarian or breast cancer. These considerations are required in health care contexts to provide adequate psychosocial support for people undergoing genetic testing.
ARTICLE HIGHLIGHTS
Research background
The majority of BRCA1/2 genetic test consists of an inconclusive result, which produces a complex situation, as it means that a deleterious mutation is neither identified nor definitively excluded.
Research motivation
Studies specifically focusing o n the psychological adjustment of people with inconclusive results are scarce and a systematic review on this topic is missing.
Research objectives
The principal purpose of this review was to examine short-, intermediate-, and longterm psychological outcomes of receiving an uninformative BRCA1/2 test result, with regard to distress (both general and genetic testing-specific), anxiety, and depressive levels. A further purpose was to highlight risk and protective factors affecting psychological adjustment in individuals with an inconclusive genetic testing result, also considering differences associated with being or not affected by a cancer diagnosis.
Research methods
The guidelines of Preferred Reporting Items for Systematic Review and Meta-Analyses were followed in the current review. A comprehensive literature search in PubMed,PsychInfo, and Cochrane Central Register of Controlled Trials was carried out. Search results referred to the last 21 years (1999-2020).
Research results
Studies on psychological outcomes of inconclusive BRCA1/2 focused on general and specific distress, anxiety, and depression. Overall, they produced mixed results. These inconsistent findings are probably due to the uncertainty caused by this type of result,that may also influence the decisions of individuals about surveillance and prophylactic options, reducing their compliance. In addition, this review highlights specific risk and protective factors that affect psychological adjustment in individuals with an inconclusive genetic testing result.
Research conclusions
This review highlights that individuals who receive an inconclusive result are a subgroup of patients who need educational programs and more pre-test information to better understand the meaning of their test in order to make adequate decisions about surveillance and prophylactic options.
Research perspectives
Overall, the current review highlights the importance to address two main issues in this field: From a research perspective, it is recommended the development of tools more sensible to detect the psychological outcomes of inconclusive BRCA1/2 genetic test results; from a clinical perspective, health professionals and genetic counsellors should provide more psychoeducational support to this subgroup of patients about the meaning and the management of the uncertainty associated with their condition.