Femoral lengthening in young patients: An evidence-based comparison between motorized lengthening nails and external fixation
2021-11-22MohamedHafezNicolasNicolaouAmakaOffiahStephenGilesSanjeevMadanJamesFernandes
Mohamed Hafez, Nicolas Nicolaou, Amaka C Offiah, Stephen Giles, Sanjeev Madan, James A Fernandes
Mohamed Hafez, Department of Oncology and Metabolism, Sheffield University, Sheffield S10 2TN, United Kingdom
Mohamed Hafez, Nicolas Nicolaou, Stephen Giles, Sanjeev Madan, James A Fernandes,
Department of Paedaiatric Limb Reconstruction, Sheffield Children Hospital, Sheffield S10 2TH, United Kingdom
Amaka C Offiah, Department of Radiology, Sheffield Children Hospital, Sheffield S10 2TH, United Kingdom
James A Fernandes, Department of Trauma and Orthopaedics, Sheffield Children Hospital, Sheffield S10 2Th, United Kingdom
Abstract BACKGROUND Femoral lengthening is a procedure of great importance in the treatment of congenital and acquired limb deficiencies. Technological advances have led to the latest designs of fully implantable motorized intramedullary lengthening nails. The use of these nails has increased over the last few years.AIM To review and critically appraise the literature comparing the outcome of femoral lengthening in children using intramedullary motorized lengthening nails to external fixation.METHODS Electronic databases (MEDLINE, CINAHL, EMBASE, Cochrane) were systematically searched in November 2019 for studies comparing the outcome of femoral lengthening in children using magnetic lengthening nails and external fixation. The outcomes included amount of gained length, healing index, complications and patient reported outcomes.RESULTS Of the 452 identified studies, only two (retrospective and non-randomized) met the inclusion criteria. A total of 91 femora were included. In both studies, the age of patients treated with nails ranged from 15 to 21 years compared to 9 to 15 years for patients in the external fixation group. Both devices achieved the target length. Prevalence of adverse events was less in the nail (60%-73%) than in the external fixation (81%-100%) group. None of the studies presented patient reported outcomes.CONCLUSION The clinical effectiveness of motorized nails is equivalent or superior to external fixation for femoral lengthening in young patients. The available literature is limited and does not provide evidence on patient quality of life or cost effectiveness of the interventions.
Key Words: Lengthening nails; Motorized nails; Distraction ostepgenesis; Lengthening
INTRODUCTION
Limb length discrepancy (LLD) is a common finding in multiple congenital and acquired disorders. LLD may lead to significant consequences such as changes in gait biomechanics, back pain, lower limb osteoarthritis, psychological problems, and poor function and lifestyle. It is accepted that LLD below 2 cm can be treated with appropriate orthotics. LLD of 2 to 5 cm can be managed with growth modification (epiphysiodesis) of the longer side. For a LLD greater than 5 cm, limb lengthening is indicated[1].
Gavrill Ilizarov introduced the concept of distraction osteogenesis (DO) and circular external fixators for management of trauma and deformities[2]. For decades, the Ilizarov technique was the most effective method of limb lengthening. It is cheap, reproducible and allows correction of angular deformities and spanning of joints if required[3]. However, external fixation significantly limits the patient’s activities and life style and has a high risk of complications[4]. The preference of external fixation for bone lengthening has started to decline since the introduction of motorized lengthening nails.
Lengthening nails are intramedullary telescopic devices that securely fix within the intramedullary canal and telescope to produce the desired length (Figure 1). The older designs of lengthening nails relied on a ratchet mechanism that was activated by rotating the leg to produce lengthening[2]. Recent designs of lengthening nails provide distraction by activation of a motor inside the nail with external remote control (ERC) applied externally to the limb. Motorized nails include the PRECICE nail (PRECICE lengthening nail: Nuvasive, CA, United States) and Fitbone nail [FITBONE Telescope Active Actuator (TAA) nail: Wittenstein Intens, Igersheim, Germany].
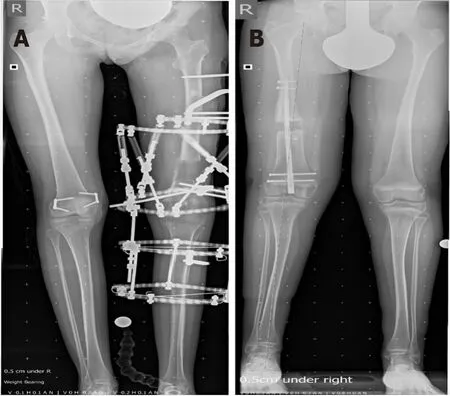
Figure 1 Left femoral lengthening with external fixation (A) and right femoral lengthening with magnetic lengthening nail (B).
The initial designs of lengthening nails were associated with failure of the telescoping mechanism[5]. The newer generation of motorized lengthening nails have improved results[6-9]. Lengthening nails were reported to offer more active postoperative life styles, fewer post-operative infections and less metal work failures compared to earlier designs and external fixation[10]. Motorized lengthening nails have been used initially for femoral lengthening, however their applications have increased to include other long bones such as tibia[7] and humerus[11].
The average cost of the motorized nail implants is £12000-£13000 (€14000–€15000/$15000-$16000) while the average cost of external fixators varies from £3000 to £9000 (€3500–€10500/$3500-$11500)[12].
Within the limited resources available to the National Health Service (NHS) and the United Kingdom being a welfare state, increasing emphasis has been placed on costeffectiveness. The assessment of health-related quality of life (HR-QoL) and cost utility analysis have become the foundation of economic evaluation of health technologies and gained importance in supporting the decision for allocation of NHS resources.
The recent shift to use motorized nails for bone lengthening in children despite the significant difference in implant costs compared to traditional treatment with external fixation necessitated this systematic review. This review is focused on femoral lengthening only because the initial lengthening nails were designed for femoral lengthening and the femur is the most frequently lengthened bone with motorized nails.
We present a systematic review of the studies comparing femoral lengthening in children using motorized nails to external fixation. We aimed to identify the most clinical and economic effective technique of femoral lengthening in children.
MATERIALS AND METHODS
Review question
Is the extra cost of the motorized intramedullary nails compared to external fixation in children justified?
This question can be divided to the following questions: (1) What is the clinical effectiveness of motorized lengthening nails in comparison to external fixation for femoral lengthening in children? (2) Is there a difference in the HR-QoL between the two techniques? and (3) What is the cost effectiveness of the two techniques?
Methods
Eligibility criteria:All studies, irrespective of design, that compared the outcomes of both techniques for femoral lengthening in children (less than 18 years old). All indications for femoral lengthening were included. Use of a motorized lengthening nail was the intervention and any type of external fixation was considered the comparator. The outcomes included clinical, radiological and HR-QoL.
Literature search strategy:Literature search on Healthcare Database Advanced Search (HDAS) was conducted on Medline and EMBASE databases. The HDAS search was supplemented with a complementary search on PubMed (NCBI) database. Medical subject heading (MeSH) was identified from the available studies and searched separately. References and citations from the identified studies were screened to identify further eligible papers. Terms “limb lengthening”, “bone lengthening”, “distraction osteogenesis’, “external fixation”, Ilizarov”, intramedullary nails”, “lengthening nails”, “magnetic nails”, “quality of life”, “cost-benefit analysis”,” Health care cost” and “quality adjusted life years” were used for the HDAS search, A thesaurus was used to further identify the MeSH on different databases. Different results were combined with “and’ or “or” where applicable. The reference lists of all relevant articles were screened to find other potentially relevant articles. Titles, abstracts and when relevant the full texts of the relevant studies were reviewed. Only studies published in English were retrieved. No time limit was selected.
Data extraction:Study design, methodology, country, number and age of participants, type of intervention and outcome of treatment (clinical, radiological, and quality of life) were recorded.
Quality assessment of eligible papers was performed using the Critical Appraisal Skills Program (CASP) checklist.
Data synthesis:Given the small number of papers retrieved, we provide a narrative summary of findings and a description of their strengths and limitations rather than calculating summary scores/statistical analysis.
RESULTS
A total of 452 studies were identified (Figure 2). After screening the titles and abstracts of these studies, 98 were considered potentially eligible for inclusion. Of these, 30 were excluded because the full texts were not available. Of the remaining 62, 60 were excluded, either because they were not comparative studies (58) or were not in children[2]. Therefore, there were only two studies which met our inclusion criteria.
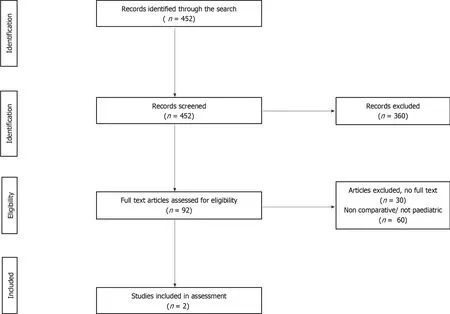
Figure 2 PRISMA flow diagram for the systematic review.
Study design and patient population
Both were non-randomized retrospective studies. Szymczuket al[13] compared the PRECICE nail in 30 femora to 32 cases of femoral lengthening using the LRS (Limb Reconstruction System Orthofix,McKinney,TX,United States)monolateral external fixator. The average ages were 15.4 and 9.4 years for the nail and external fixator groups respectively. Blacket al[14] compared the outcome of femoral lengthening using the retrograde Fitbone nail in 15 femora with the outcome of lengthening using circular fixators in 14 femora. The average ages were 15 and 18 years for the nail and external fixator groups respectively.
Outcomes
Both studies evaluated the outcome based on average length achieved, and complications. Szymczuket al[13] also reviewed range of movement (ROM) and healing index (HI). None of the studies reported children’s quality of life or cost of treatment.
Gain in length and HI
Szymczuket al[13] reported an average length gain of 4.8 cm (range 3.4 to 6.2 cm) with the PRECICE nail and 5.6 cm (range 3.9 to 7.3 cm) with the LRS external fixator. In their study, 26 patients (87%) in the nail and 28 patients (88%) in the fixator group achieved the target length of 4 cm. The healing index (HI) was 34.3 d/cm and 29.3 d/cm for nails and fixators respectively. Length of hospitalisation was not recorded.
Blacket al[14] reported an average length gain of 4.8cm (range 1 to 7.4 cm) and 4.4 cm (range 1.5 to 7 cm) with the external fixator and motorized nails respectively. In Black’s study, 10 patients (71%) in the external fixator group and 11 (73%) patients in the nail achieved the target length of 4 cm. There was no report on HI, however the time to full weight bearing was 7.7 mo with nails and 8.8 mo with external fixators. Length of hospitalisation was 7 and 9.5 d with nails and fixators respectively.
Complications
Szymczuket al[13] reported complications in 18 (60%) of the nails compared to 26 (81%) in the fixator group (P< 0.001). The average complication per lengthening session was 1.0 with nails and 1.8 with external fixators.
By comparison, Blacket al[14] reported complications in 10 (73%) of the nails compared to all 15 (100%) in the circular fixator group. Minor complications such as pin site infections and minimal joint contractures were seen in 5 (33%) of the nail group compared to 12 (79%) in the circular frame group. There was no statistical difference between the rate of types II and IIIA complications between the two groups. Serious complications such as joint dislocations were less common with the nails, 3 (20%) compared to 5 (36%). In the circular fixator group, there was no statistical difference between the two groups for moderate complications such as delayed union. The average complication per lengthening was 1.2 with nails and 2.6 with external fixators. Characteristics of the publications are summarized in Table 1. Results are summarized in Table 2.
Quality of papers:This is summarized in Table 3.
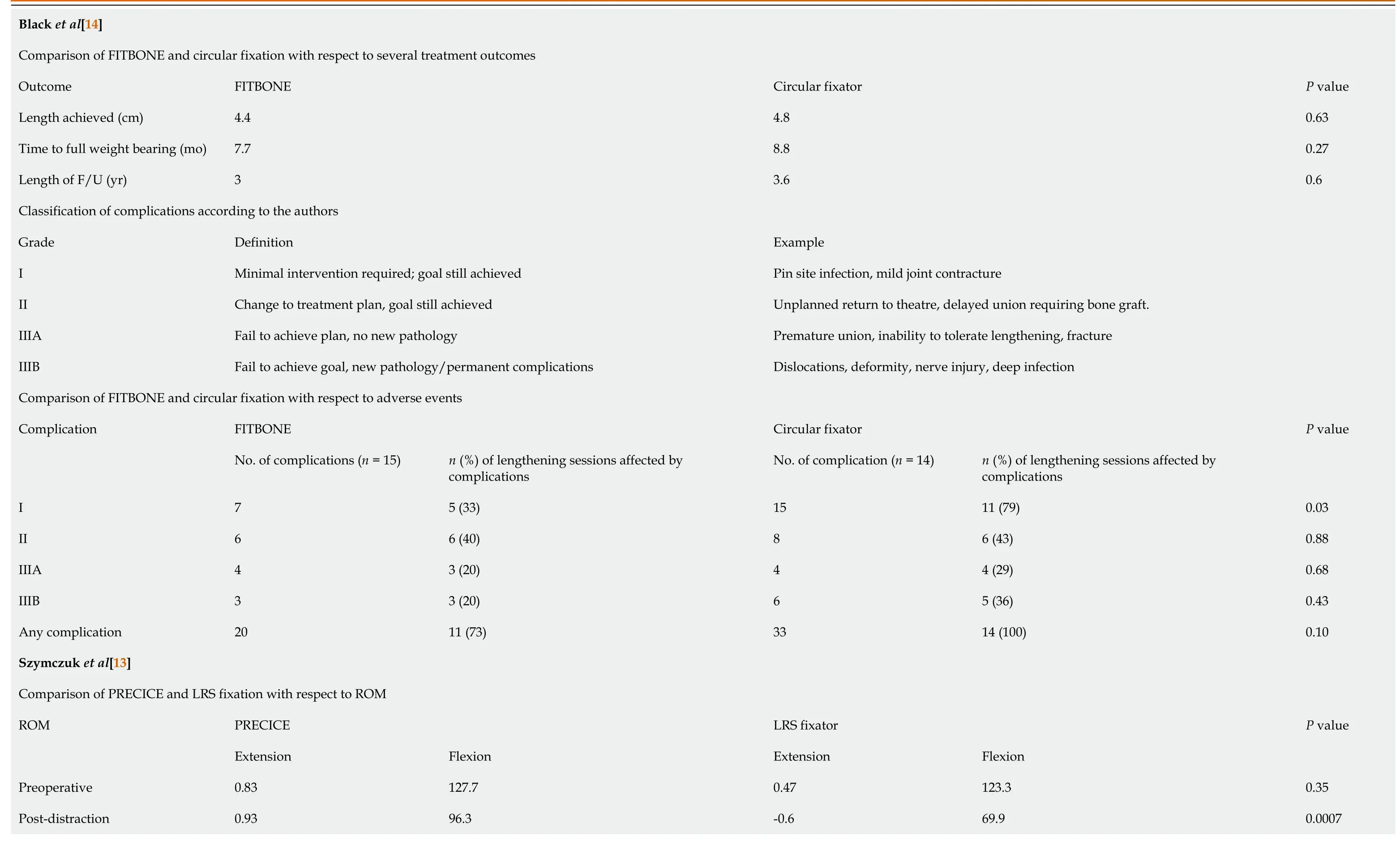
Table 2 Findings of the included publications

Table 3 Quality assessment of included publications
DISCUSSION
The presented literature review identified a lack of comparative studies in children. Two studies combined adults and children in the same group but did not present the data in such a way as to allow extraction of the pediatric data[15,16]. There is no evidence of QOL comparison between these interventions. No cost analysis was presented to support the use of lengthening nails. All these findings mandate further research to cover these points.
The current knowledge in respect to the research questions are summarized as follow: What is the clinical effectiveness of motorized lengthening nails in comparison with external fixation for femoral lengthening in children?
Both motorized nails and external fixators can effectively achieve the target femoral length. Range of motion of the knee was better preserved during the course of lengthening with nails, however there was no significant difference at the final follow up visit[13]. The overall gained length was greater with external fixators compared to motorized nails; 4.8vs4.4 cm[14] and 5.6vs4.8 cm[13] respectively. Blacket al[14] reported a shorter time to union (by 1.1 mo) with motorized nails although Szymczuket al[13] reported a shorter healing index (by 5 d/cm) with the LRS external fixator. Complication rates were lower with lengthening nails however knee subluxation was specifically reported with the nails due to the inability of the technology to span the knee. For this reason a recommendation to reconstruct knee ligaments at preparatory surgery prior to lengthening with nails was suggested[13]. However, the long-term outcome and cost effectiveness of ligament reconstructions prior to lengthening arenot yet clear.
External fixation devices are very versatile, they can be applied in young children with short or deformed femora[2]. External fixators are relatively cheap compared to motorized intramedullary nails, however there were many reported adverse events related to external fixators. Pin site infection, pain, stiffness, fracture, injury to nerves or vessels and psychological problems were frequently reported with external fixation[17]. On the other hand, intramedullary nails can only be used in relatively longer femora with appropriate width of the medullary canal. The presence of an open distal femoral physis in skeletally immature children is generally a contraindication for retrograde nails however, if the femoral canal is wide enough and the femur had normal proximal anatomy a trochanteric entry nail can be used safely[18].
Laubscheret al[15], reported better clinical outcomes and less complications with magnetic nails compared to monolateral fixator for femoral lengthening. This study included paediatric and adult age groups. According to this study 100% of the nail and 68% of the fixator participants chose to have same treatment again. Hornet al[16], compared the outcome of femoral lengthening with motorized nails to external fixation in age and sex matched patients. The mean age of patients was 27 years. HI and knee ROM were better with lengthening nails, while complications were more frequent with external fixators. Morrisonet al[19], compared the outcome of humeral lengthening with lengthening nails in 6 patients to external fixations in 7 patients. Lengthening nails patients had less complications compared to external fixators. Lengthening nails were reported to be safe, well tolerated, and effective for humeral lengthening[19].
Is there a difference in the HR-QoL between the two techniques?
We did not identify any studies which compared the quality of life of children treated with motorized lengthening nails and external fixators. However, HR-QoL was the outcome for two non-comparative studies. The authors concluded that patients have lower quality of life scores during the course of treatment[20]. One study[20] compared patient satisfaction following lengthening nails to a previous session of lengthening using external fixation in 13 patients. Patients reported less pain, more satisfaction, easier physiotherapy, and better cosmetic appearance following magnetic nails compared to previous lengthening using external fixators. It is worth mentioning that this study did not utilize a validated outcome questionnaire and there was high probability of recall bias since the QoL scores were recorded at the time of final interview[21]. The pediatric quality of live inventory (PedsQL) was used in studies for children treated with external fixation. The children and their parents reported significantly lower HR-QoL scores on all PedsQl domains compared with a normal healthy population.
The HR-QoL of motorized nails compared to external fixators for femoral lengthening in children is not known. It is clear that both techniques have a negative impact on HR-QoL. There is limited evidence suggesting that this negative impact is greater for external fixators than for motorized nails.
What is the cost effectiveness of the two techniques?
A cost comparison of the two techniques has not previously been reported. However Richardsonet al[12] did estimate the cost of lengthening with the PRECICE nail to be approximately $44449 (£34650, €40110). This value was calculated after reviewing hospital costs and surgeon fees from the lengthening surgery up until the time of union in 39 femora. This study included adults and children, neither the surgical costs of nail removal nor the costs of loss of income, hospital visits and outpatient medications were included.

1Problems, obstacles, complications: A classification system of adverse events associated with limb lengthening.Problems include incidents that do not need operative intervention. Obstacles were the incidents requiring operative but did not lead to permeant complications. Complications included intraoperative injuries and non- resolved problems before the end of treatment.
The cost effectiveness of motorized nails compared to external fixators for femoral lengthening in children is not known.
Critical appraisal of the included publications
The objectives of and interventions used in both studies were clearly mentioned and inclusion and exclusion criteria were specified. The measured outcomes were mentioned clearly in the methods and in the results sections. Statistical analysis was clear with appropriate statistical test (t-test) in Szymczuket al[13]. Authors of both studies classified the complications according to severity and reported the complications accurately.
Limitations were also identified in both studies. Both focused on one indication for femoral lengthening (congenital femoral deficiency), excluding all other causes of femoral shortening such as trauma and infection. There was a high possibility of selection bias in both studies, given their non-randomized retrospective designs. At the time of the study, the Fitbone nail did not have FDA (Food and Drug Administration agency) approval for use in the United States; therefore patients recruited to the study by Blacket al[14] were treated on a compassionate-use basis. This suggests that the selection of patients was based on meeting the criteria for inclusion on a compassionate basis rather than matching the nails and external fixator groups. Szymczuket al[13] did not specify their selection criteria. Neither study was blinded; this would have been difficult given the nature of the interventions being compared.
The age of patients both groups in the study by Szymczuket al[13] were not matched. Nails were used for children over 9 years and fixators for children as young as 3 years. This policy might have affected the overall complication rates due to increased use of fixators in the higher risk group of younger children. Blacket al[14] included patients of matched age groups, however all the patients who were treated with nails were skeletally mature and all of the nails were inserted retrograde sparing the trochanteric region. This might suggest that although the participants of this group were younger than 18 years, they had adult bones and the results might not be representative for children.
CONCLUSION
There is no literature comparing the cost effectiveness and patient satisfaction of femoral lengthening with motorized lengthening nails and external fixators in children. Further research is necessary in order to ascertain the efficacy of these treatment methods, to optimize patient outcomes and to ensure health care resources are spent appropriately.
ARTICLE HIGHLIGHTS
Research background
For decades external fixation was the only reliable, safe, and reproducible technique for bone lengthening. The use of external fixation declined recently due to the development of motorized lengthening nails. Lengthening nails are expensive.
Research motivation
Is the extra cost of the motorized intramedullary nails compared to external fixation in children justified?
Research objectives
The main objective was to review the literature to compare the clinical effectiveness of motorized lengthening nails to external fixation. Other objectives were to identify differences in the health-related quality of life between the two techniques in current literature.
Research methods
Electronic databases (MEDLINE, CINAHL, EMBASE, Cochrane) were searched, and all relevant studies were considered for analysis based on predetermined inclusion/exclusion criteria. The subject headings “distraction osteogenesis”, “motorized nails”,‘’ external fixation’’ and their related key terms were used.
Research results
Only 2 studies out of 452 studies met the inclusion criteria. The ages of the patients ranged from 9 to 21 years. Lengthening nails were effective in achieving the target length with less prevalence of adverse events.
Research conclusions
The clinical effectiveness of lengthening nails was comparable to external fixation. No report on the quality-of-life difference between the 2 techniques during lengthening. No reports on the cost effectiveness of lengthening nails compared to external fixations.
Research perspectives
Further research is necessary in order to ascertain the efficacy of these treatment methods, to optimize patient outcomes and to ensure health care resources are spent appropriately.
杂志排行

World Journal of Orthopedics的其它文章
- Revisiting Pauwels' classification of femoral neck fractures
- Paraspinal strength and electromyographic fatigue in patients with sub-acute back pain and controls: Reliability, clinical applicability and between-group differences
- Preseason elimination impact on anterior cruciate ligament injury in the national football league
- Risk of methicillin-resistant staphylococcus aureus prosthetic joint infection in elective total hip and knee arthroplasty following eradication therapy
- Reliability of a simple fluoroscopic image to assess leg length discrepancy during direct anterior approach total hip arthroplasty
- Anthropometric method for estimating component sizes in total hip arthroplasty