A Patient with Atezolizumab-Induced Autoimmune Diabetes Mellitus Presenting with Diabetic Ketoacidosis
2021-10-22SharenLeeandGaryTsePhDFACCFRCP
Sharen Lee and Gary Tse,PhD,FACC,FRCP,2,3
1 Cardiovascular Analytics Group,Laboratory of Cardiovascular Physiology,Hong Kong,HKG,China
2 Tianjin Key Laboratory of Ionic-Molecular Function of Cardiovascular Disease,Department of Cardiology,Tianjin Institute of Cardiology,Second Hospital of Tianjin Medical University,Tianjin,300211,China
3 Xiamen Cardiovascular Hospital,Xiamen University,Xiamen,361015,China
Abstract Background:Atezolizumab,an immune checkpoint inhibitor,is a humanized monoclonal,anti-programmed death ligand 1(PD-L1)antibody used for the treatment of metastatic urothelial carcinoma that has progressed after chemotherapy.Case Presentation:We describe a patient with a known history of urothelial carcinoma who presented with diabetic ketoacidosis 6 weeks following his second cycle of atezolizumab.His serum lactate level was slightly elevated(2 mM)and his β-hydroxybutyrate level was elevated(3.9 mM).High anion gap metabolic acidosis secondary to diabetic ketoacidosis was diagnosed.Subsequent testing demonstrated hemoglobin A 1c level of 9.9%,positivity for antiglutamic acid decarboxylase antibody(0.03 nM,reference range <0.02 nM),and suppressed C-peptide level(0.1 μ g/L,reference range 0.9–7.1 μ g/L)in the absence of detectable anti-islet antigen 2(IA-2)or anti-insulin antibodies.His initial management included cessation of atezolizumab treatment,intravenous sodium chloride administration,and insulin pump infusion,after which metabolic acidosis gradually resolved.The insulin pump was subsequently switched to Protaphane at 18 units before breakfast and 8 units before dinner,together with metformin at 1000 mg twice daily.Four weeks later his medication was changed to human isophane insulin plus neutral insulin(70%/30%;Mixtard 30 HM;26 units/4 units).Linagliptin at 5 mg was added 1 month later.His hemoglobin A 1c level declined to 8.1% 1 year later.Conclusions:PD-L1 inhibitors can induce type 1 diabetes,and patients can present with diabetic ketoacidosis.Blood glucose levels should be regularly monitored in patients who are prescribed these medications.
Keywords:Atezolizumab;diabetic ketoacidosis;PD-L1 inhibitors;Type 1 diabetes
Background
Atezolizumab,an immune checkpoint inhibitor,is a humanized monoclonal,anti-programmed death ligand 1(PD-L1)antibody used for the treatment of metastatic urothelial carcinoma that has progressed after chemotherapy[1].It was the first agent approved by the US Food and Drug Administration as secondline treatment for advanced urothelial carcinoma[2].Although immune checkpoint inhibitors are generally well tolerated compared with traditional chemotherapy,they can produce immune-related toxic effects[3].PD-L1 inhibitors are recognized to cause thyroid problems but are now known to induce autoimmune diabetes.In this report,we describe a patient with a known history of urothelial carcinoma who presented with diabetic ketoacidosis 6 weeks following his second cycle of atezolizumab.
Case Presentation
A 75-year old man presented to the emergency department of our hospital with polydipsia,polyuria,nausea,vomiting,and reduced appetite associated with generalized malaise.He also reported increasing dyspnea and a productive cough.On inspection,the patient was dehydrated and showed signs of Kussmaul breathing.Physical examination revealed increased sputum sounds and crepitations on the lower chest bilaterally.His abdomen was soft and nontender.
Table 1 Arterial Blood Gas Parameters at Presentation.
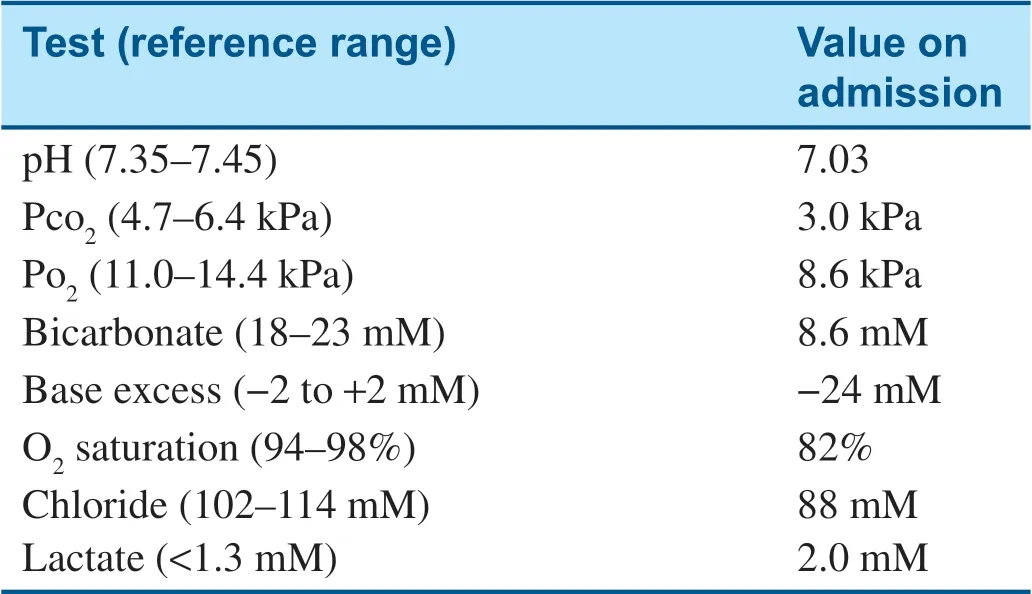
Test(reference range)Value on admission pH(7.35–7.45)7.03 P co 2(4.7–6.4 kPa)3.0 kPa P o 2(11.0–14.4 kPa)8.6 kPa Bicarbonate(18–23 mM)8.6 mM Base excess(−2 to +2 mM)−24 mM O 2 saturation(94–98%)82%Chloride(102–114 mM)88 mM Lactate(<1.3 mM)2.0 mM
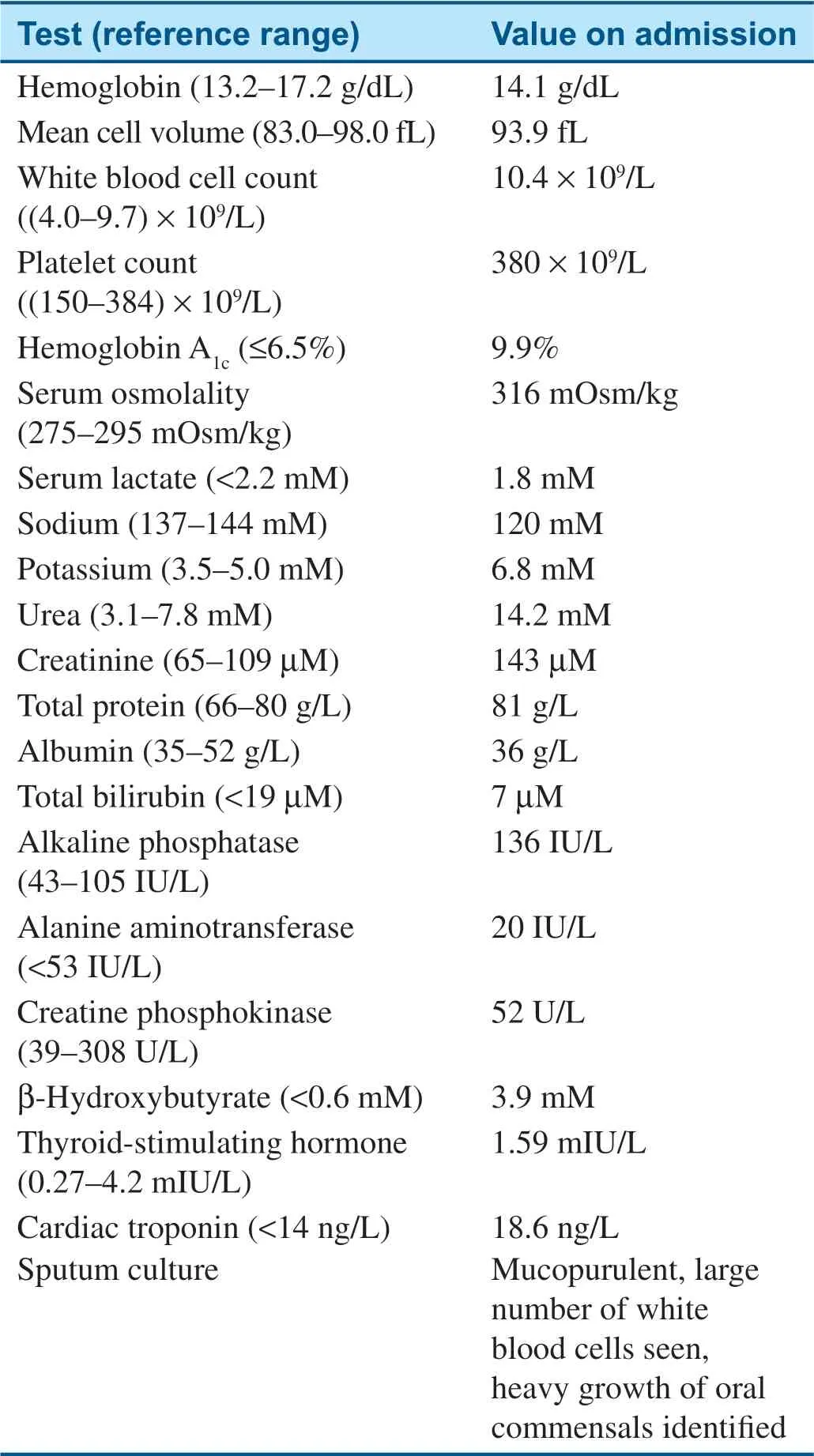
Table 2 Laboratory Test Results at Presentation.
The arterial blood gas and blood test results on admission are shown in Tables 1 and 2,respectively.Of note,his capillary glucose level was more than 27.8 mM(500.4 mg/dL).His fasting glucose level was 4.5 mM(81.0 mg/dL)3 months before admission,and his random glucose level was 5.4 mM(97.2 mg/dL)2 months before admission.Serum biochemistry showed hyponatremia(120 mM)and hyperkalemia(6.8 mM).His liver enzyme levels were normal but urea and creatinine levels were raised(6.8 and 14.2 mM,respectively).His arterialblood gas test results showed a severe metabolic acidosis.The uncorrected anion gap was 30 mM,but after correction for albumin(23 g/L)a significantly elevated anion gap of 34 mM was revealed.His serum lactate level was slightly elevated(2 mM)and his β-hydroxybutyrate level was elevated(3.9 mM).High anion gap metabolic acidosis secondary to diabetic ketoacidosis was diagnosed.Subsequent testing demonstrated hemoglobin A1c(HbA1c)level of 9.9%,positivity for anti-glutamic acid decarboxylase antibody(0.03 nM,reference range <0.02 nM),and suppressed C-peptide level(0.1 μ g/L,reference range 0.9–7.1 μ g/L)in the absence of detectable anti-islet antigen 2(IA-2)or anti-insulin antibodies.
His initial management included cessation of atezolizumab treatment,intravenous sodium chloride administration,and insulin pump infusion,after which metabolic acidosis gradually resolved.Insulin pump was subsequently switched to Protaphane at 18 units before breakfast and 8 units before dinner,together with metformin at 1000 mg twice daily.Four weeks later his medication was changed to human isophane insulin plus neutral insulin(70%/30%;Mixtard 30 HM;26 units/4 units).Linagliptin at 5 mg was added 1 month later.His HbA1clevel declined to 8.1% 1 year later.
Discussion
Programmed cell death 1(PD-1)is a coreceptor that is expressed predominantly by T cells in many cancers[4].It interacts with PD-L1 and PD-L2 of antigen-presenting cells and tumor cells.Normally,binding of PD-1 to its effectors inhibit T cells and prevents immune activation.Blocking this binding leads to activation of cytotoxic T cells,thereby triggering an immune response to target tumor cells.Anti-PD-1 or anti-PD-L1 monoclonal antibodies have been increasingly used to treat different cancers,including urothelial cancers[5].To date,33 cases of diabetes have been reported as a result of anti-PD-1 or anti-PD-L1 antibody treatment[6–26].Of these,only four cases were due to PD-L1 inhibitor treatment.The first case concerned a 70-year old man with adenocarcinoma of the lung without a history of diabetes who presented with hyperglycemia 15 weeks after treatment with an anti-PDL-1 antibody(the name of the drug was not reported)[13].The second case concerned a 57-year old man with recurrent metastatic urothelial cancer who presented with incomplete diabetic ketoacidosis before his sixth cycle of the anti-PD-L1 antibody atezolizumab[18].The third case involved a 63-year old woman with a history of hypothyroidism and irondeficiency anemia with reactive thrombocytosis and leukocytosis who initially presented with hematuria and who subsequently underwent transurethral removal of a bladder tumor and was treated with atezolizumab but developed diabetic ketoacidosis after 6 weeks[25].The fourth case concerned an 84-year-old woman with metastatic squamous cell carcinoma of the nasopharynx and no history of diabetes who was given the anti-PD-L1 antibody durvalumab and developed diabetic ketoacidosis 4 months later[26].Here we report,to the best of our knowledge,the first case in an Asian male patient and the f ifth case published thus far showing that atezolizumab can precipitate diabetic ketoacidosis.Our patient had a history of transitional cell carcinoma of the renal pelvis and presented with full diabetic ketoacidosis 6 weeks after his second cycle of atezolizumab.His C-peptide level was low,consistent with type 1 diabetes mellitus.
Of the previous 33 cases,31 patients underwent autoantibody testing,of whom 18 showed positive results.Our patient was positive for antiglutamic acid decarboxylase antibody,albeit only at a low level of 0.03 nM(reference range <0.02 nM).Previously,it was noted that the time between initiation of PD-1/PD-L1 inhibitor treatment and the onset of autoimmune diabetes was related to anti-glutamic acid decarboxylase antibody status[19].Gauci et al.[19]calculated that the duration was shorter,with a median of 3 weeks,for positive status but was 12–13 weeks for negative status.These observations are in agreement with those of our patient,who had positive but low levels of antiglutamic acid decarboxylase antibody,presenting 6 weeks after treatment.Although the use of PD-1 and PD-L1 inhibitors is mostly associated with type 1 diabetes,it can also worsen glucose control in those patients with established type 2 diabetes[27].Moreover,it has been suggested that PD-1 and PD-L1 inhibitors may also predispose to type 2 diabetes[28].
The mechanisms underlying precipitation of diabetes mellitus by PD-1 or PD-L1 inhibitors remain incompletely understood.Type 1 diabetes mellitus involves autoimmune-mediated damage of the pancreas by the body’s own immune system[29].This can be triggered by different antigens,leading to reduced central or peripheral tolerance[30],and thus activation of the T lymphocytes.T lymphocytes can then infiltrate into the pancreatic islets and mediate destruction of the pancreatic β cells,leading to uncontrolled hyperglycemia.It is well established that coinhibitory PD-1/PD-L1 interactions provide the molecular signals that regulate autoreactive T-lymphocyte responses[31].Indeed,the interaction between PD-1 expressed on autoreactive T cells and PD-L1 expressed on pancreatic islet cells leads to the development of tolerance.By contrast,when either protein is inhibited,autoreactive T cells are relieved from inhibition and can induce cell death of the islet cells,leading to the development of autoimmune diabetes.Significantly,the available evidence suggests that even after discontinuation of immunotherapy,insulin therapy was required,which would indicate that the diabetes is irreversible[24].In our case,the patient required long-term insulin therapy with adjunct hypoglycemic agents,which led to a decline of HbA1clevel from 9.9%to 8.1% 1 year later.These findings are in keeping with the notion ofirreversible pancreatic damage.
The use of experimental animal models has provided some insights into possible mechanistic pathways.Thus,Pdcd1−/−mice,which are deficient in PD-1,demonstrate an accelerated onset and frequency of type 1 diabetes[32].These findings are consistent with the notion that PD-1/PD-L1 interactions are important for the regulation of autoreactive T-lymphocyte responses by mediating peripheral tolerance[33],which suppresses diabetes.Indeed,clinical studies have reported the association between PD-L1 gene haplotype[34],its polymorphisms,and low serum PD-L1 levels[35]and type 1 diabetes.Together these findings demonstrate the importance of PD-1/PD-L1 pathways in pancreatic cell function and that treatment modalities targeting these proteins can exert adverse effects on glucose control,thereby precipitating or inducing diabetes.Thus,activating the PD-1 pathway may help to induce immune tolerance and prevent type 1 diabetes but increase the risk of cancer or metastasis.This is supported by experimental observations that PD-L1-driven tolerance reverses diabetes in nonobese diabetic(NOD)mice,a model for autoimmune type 1 diabetes[36].There thus appears to be a balance of risk of cancer on the one hand and risk of diabetes on the other.Indeed,epidemiology studies clearly demonstrate the high rates of cancer and type 2 diabetes in developing areas where autoimmune type 1 diabetes is rare.
Conclusion
PD-L1 inhibitors,like PD-1 inhibitors,can induce type 1 diabetes,and patients can present with diabetic ketoacidosis.Blood glucose levels should be regularly monitored in patients who are prescribed these medications.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case.
Conf licts ofinterest
None declared.
Author Contributions
Both authors drafted and critically revised the manuscript and approved the final version.
杂志排行

Cardiovascular Innovations and Applications的其它文章
- Running with Face Masks or Respirators Can Be Detrimental to the Respiratory and Cardiovascular Systems
- CTO(Chronic Total Occlusion)
- In-Hospital Cardiac Arrest after Emotional Stress in a Patient Hospitalized with Gastrointestinal Symptoms and Chronic Anxiety Disorder
- Junctional Pacemaker May Replace the Sinoatrial Node
- Clinical Characteristics and Durations of Hospitalized Patients with COVID-19 in Beijing:A Retrospective Cohort Study
- Similarities and Differences of CT Features between COVID-19 Pneumonia and Heart Failure