Evidence summaries for nutritional screening of head-and-neck cancer patients
2021-10-12YeLIYiYuanLIUYaJuanTIANLingTANG
Ye LI,Yi-Yuan LIU,Ya-Juan TIAN,Ling TANG
Department of Nursing,Dongfang Hospital of Beijing University of Chinese Medicine,Beijing,China
ABSTRACT The guidelines for nutritional screening of head-and-neck cancer patients were systematically searched and screened from BMJ Best Practice,National Comprehensive Cancer Network,Britain's National Institute for Health and Clinical Excellence,National Guideline Clearinghouse,Scottish Intercollegiate Guidelines Network,Guidelines International Network,New Zealand Guidelines Group,Australian National Health and Medical Research Council,Medlive,PubMed,Embase,CINAHL,China Biology Medicine,VIP,Chinese National Knowledge Infrastructure,and Wanfang.Four researchers evaluated the quality of the included literature and extracted evidence from the literature that met the quality standards.Finally,a total of six guidelines were included and ten best evidences were concluded.As only one guideline in this study is from China,and the rest are from other countries,the applicability and effectiveness of some evidence in the Chinese population still need to be further explored and studied.Therefore,when using evidence,medical staff should make appraisal on working environment in their hospital,factors that facilitate or hinder the use of evidence,and willingness of patients,and thus scientifically provide the best evidence for the management of clinical nutrition for head-and-neck cancer patients and provide a reference for the establishment of the standard process of nutritional screening for head-and-neck cancer patients.
Keywords:Evidence summaries,head-and-neck cancer,nutritional screening
INTRODUCTION
Malnutrition and nutritional risks often adversely affect tissue repair and immune function of the body,delay functional recovery,increase the risk of infection,prolong hospital stay and increase re-hospitalization rate,and even lead to increased complications and mortality.[1]The incidence of malnutrition is as high as 88% in patients with head-and-neck cancer,[2]which includes nasopharyngeal carcinoma,laryngeal cancer,stomach cancer,and tongue cancer.Patients with those cancer require surgical treatment and/or radiation and chemotherapy treatment,so patients are not eating properly after surgery,meanwhile concurrent radiation and chemotherapy can have some side effects (such as increasing patient’s pain,reducing patient’s quality of life,eating,and sleep) which can further lead to deterioration of nutritional status to have to break off the tumor treatment and thus lose treatment time.Hence,the nutritional problems for head-and-neck cancer patients are worthy of attention.The guidelines released by the American Society for Parenteral and Enteral Nutrition in 2011 pointed out that nutrition screening,nutrition assessment,and nutrition intervention are the three steps of nutrition treatment,of which nutrition screening is the basis of nutrition assessment and nutrition intervention.[3]Nutritional status of patients with head-and-neck cancer can seriously affect the patient’s disease outcomes and the occurrence of complications so that medical personnel accurately determine the patient’s nutritional status is the key to the nutritional therapy.At present,the content about nutritional screening is diverse,but there are no specific methods on nutritional screening for head-and-neck cancer patients,therefore this study aimed at providing references for specific nutritional screening methods for head-and-neck cancer patients and standardization of clinical nutrition screening and nutrition management through systematical retrieval and extraction of the relevant evidence of nutritional screening in patients with head-and-neck tumor.
MATERIALS AND METHODS
Retrieval strategy
Guidelines for nutritional screening of patients with head-and-neck tumors was searched on computer from BMJ Best Practice,National Comprehensive Cancer Network,Britain's National Institute for Health and Clinical Excellence (NICE),National Guideline Clearinghouse,Scottish Intercollegiate Guidelines Network,Guidelines International Network,New Zealand Guidelines Group,Australian National Health and Medical Research Council,Medlive,PubMed,Embase,CINAHL,China Biology Medicine,VIP,Chinese National Knowledge Infrastructure,and Wanfang.The search terms were“head and neck tumor patients”“nutritional risk/nutritional screening”and“guidelines,”and the retrieval time was from January 1,2014 to January 1,2020.
Inclusion and exclusion criteria
The inclusion criteria were as follows:(1) the subjects were patients with head-and-neck tumors;(2) age >18 years old;(3) involved in the nutrition screening study;(4) the study type was clinical practice guidelines published in Chinese or English within the past 5 years.
The exclusion criteria were as follows:(1) guidelines for which full text is not available,(2) guidelines that summarized other guidelines,and (3) guidelines with quality evaluation of Grade C.
Quality evaluation criteria
The Chinese version of Appraisal of Guidelines for Research and Evaluation II (AGREE II)[4]modified by AGREE International Collaboration in 2009 was used to strictly assess the quality of the guidelines.AGREE II is a basic instrument for the quality evaluation of the current international guidelines which can make a relatively objective appraisal on the existing clinical practice guidelines.It consists of 23 items in six domains,and 2 overall assessment items,each of which is graded on a seven-point scale.The maximum possible score=7 points (strongly agreed) × number of items × number of evaluators.The smallest possible score=1 (Strongly disagreed) × Number of items × Number of evaluators.The percentage of standardization in different domains=(Sum of all reviewers evaluation score -The smallest possible score) ÷ (The maximum possible score-The smallest possible score) ×100%.The higher the score,the more qualified the items.The grading of guidelines is as follows:Grade A:There are six domains with the score ≥60%;Grade B:There are more than three domains with the score of ≥30% and <60%;Grade C:There are more than 3 domains with the score <30%.
Quality evaluation process
The evaluation of included guidelines was completed by four members of the research group,including one who has received systematic training of the evidence application project of JBI Evidence-Based Nursing Center of Fudan University,and three nursing master students who have received systematic evidence-based medicine training.When it is difficult to determine whether to include guidelines or if there is a conflict of opinion on quality assessment of guidelines,the decision is made by the Evidence-Based Nursing Group of the hospital.When conclusions from evidence of different sources were in conflict,the inclusion principles followed in this study were evidence-based evidence first,high-quality evidence first,recently published guidelines first,and domestic guidelines first.[5,6]
Statistical method
SPSS 20.0 was used to test the consistency of the evaluation results of the guidelines which was determined by calculating the intraclass correlation coefficient (ICC).ICC >0.75 indicates high consistency.[7]
RESULTS
Guidelines general information
A total of 6 guidelines[8-13]were finally included,and the publication period was from 2016 to 2017,including 1 guideline in Chinese and 5 in English.The literature screening process was shown in Figure 1,and the screening results were shown in Table 1.
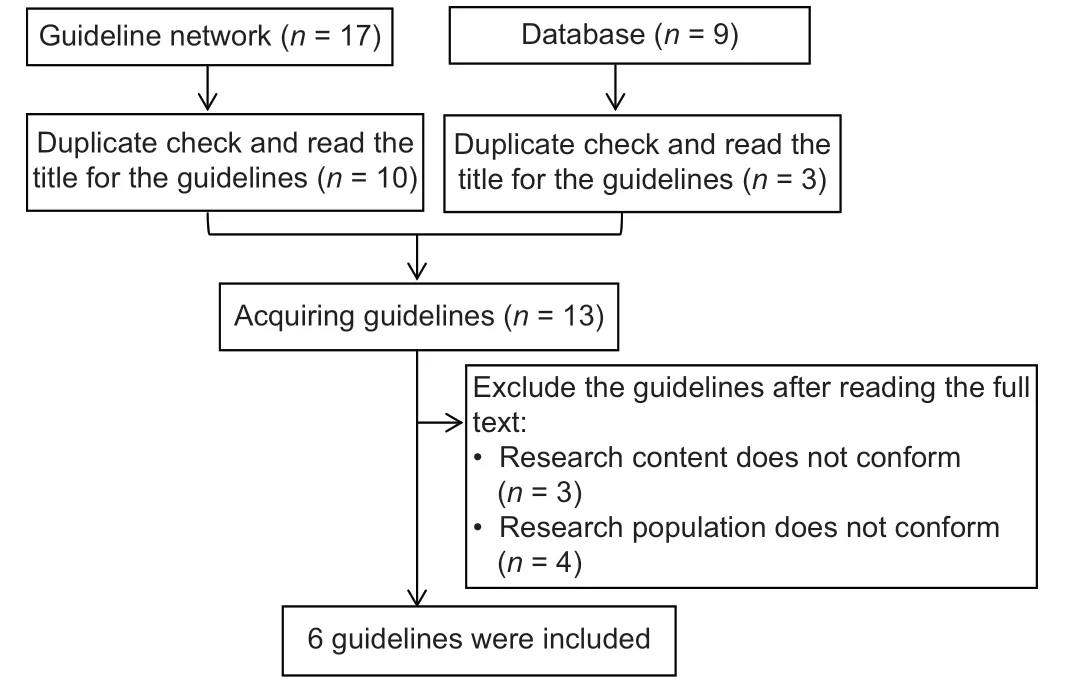
Figure 1:Screening process of guidelines
Results of consistency test among evaluators
The consistency test was conducted on the guideline evaluation results of four evaluators [Table 2].ICC values in all six guidelines were >0.75 (P< 0.001),indicating good consistency among evaluators.
The quality evaluation results of the guidelines
It can be seen from the standardized scores and quality evaluation results of the guidelines in different domains that the quality of each guideline was relatively high and recommended to be used [Table 3].
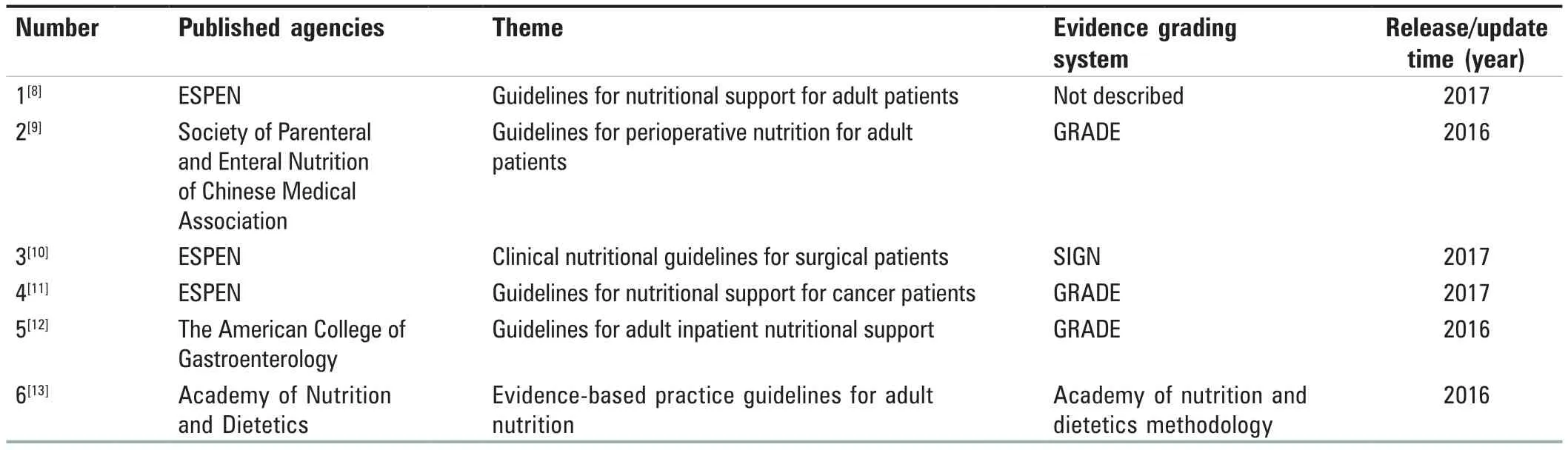
Table 1:Basic information of evidence

Table 2:Consistency test of the included guidelines
Level of evidence
Because the final included guidelines come from different agencies,the evidence grading system varies.In this study,the 2014 JBI evidence pregrading and evidence recommendation level system[14]was used to evaluate the level of the included evidence and classify the strength of recommendation.According to different research design types,evidence is classified into levels 1-5,and the recommendation level of evidence is determined based on the effectiveness,feasibility,suitability,and clinical significance of the evidence:Level A indicates strong recommendation and Level B indicates weak recommendation.[15]Through the induction and summary of relevant evidence of nutrition screening for head-and-neck tumor patients,ten items of best evidence were finally formed [Table 4].
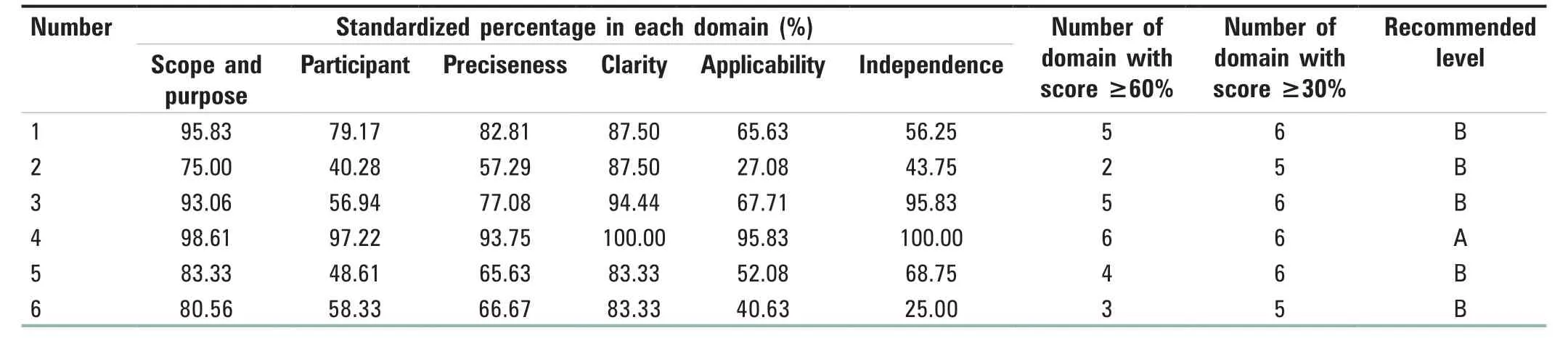
Table 3:Appraisal of guidelines for research and evaluation ll evaluation results of the included guidelines

Table 4:Best evidence for nutritional screening in patients with head and neck tumors
DISCUSSION
Qualification of nutrition screening personnel in China
Nutritional screening should be carried out by health-care professionals with appropriate skills and training.This evidence comes from European Society Of Parenteral Enteralnutrition (ESPEN)’s 2017 guidelines for cancer patients,which emphasize the qualifications of nutritional screeners.[7]This may be because nutritional screening methods are mainly based on anthropometric indicators and clinical diagnosis,and their reliability depends on the professional knowledge and level of the screeners.However,despite the high level of the AGREE II comprehensive rating in the NICE guidelines,there is no explicit reference to the evidence grading criteria in the guidelines,because of which the actual situation of the health-care providers should be taken into account when using guideline recommendations.In the United States,Canada,Australia,and other countries,nutritional screening is performed by professional nutritionists.[16]In China,the profession of registered dietitians is just emerging,and no standards have been formed in terms of the definition of nutritionists’ ability,so the level of nutritionists varies greatly.[17,18]Ravishankar and Ennaliza[19]believed that the current nutrition knowledge education and training of resident physicians were insufficient,which could not meet the nutritional needs of clinical patients.Huanget al.[20]believe that there are great differences in the development of nutrition specialist nurses,and there is no unified management and recertification mechanism,so it is necessary to further clarify the work content and ability standards of clinical nutrition specialist nurses.Thus,although the guidelines recommend that nutrition screening should be conductedby health-care professionals who have received relevant training,there is still a lack of systematic learning and practice in nutrition education for both physicians and nurses in clinical practice.It is necessary to continue to practice and explore the qualification of nutrition screening personnel according to China’s national conditions.
Population and timing of nutrition screening
The guidelines recommend that inpatients and outpatients should undergo nutritional screening when they enter a hospital to identify their potential nutritional risks.[7]In addition,regular screening should be performed for special conditions,such as head-and-neck cancer patients before and after surgery,those with insufficient expected intake,or those with chronic disease,to prevent malnutrition due to emergencies or changes in disease.At present,nutrition clinics or nutrition metabolism clinics are set up in some hospitals in China,mainly for patients with nutrition-related problems.For most of outpatient patients,routine nutrition screening has not been carried out.Clinical nutrition screening objects are mostly confined to inpatients,[21-23]and less attention is paid to nutrition screening of outpatients and home-based patients in the community.Zhuet al.[24]believed that China’s aging population is becoming increasingly serious and the incidence of malnutrition among the elderly is relatively high.Therefore,nutrition screening for the elderly in communities should be strengthened to improve their health level.However,China’s community health care is in the development stage,and the nutritional assessment and screening of patients at home are also in the exploration stage.[25]In future,it is necessary to strengthen the training of nutrition knowledge for community medical staff,establish relevant nutrition screening mechanism,and gradually improve the community-hospital nutrition screening system.
Nutrition screening tools and indicators
Several guidelines point out that specific screening tools should be used for nutritional risk screening for patients with different disease states.However,there is no specific nutritional screening tool for patients with head-and-neck tumors at present,and simple,reliable,and proven universal tools should be selected as substitutes if no specific tools are available.Currently,NRS 2002[26]is one of the most common nutritional risk screening tools and can be as a universal nutritional screening tool applied to comprehensively evaluate the nutritional risks of patients with head-and-neck cancer from their age,disease status,weight,and other factors.In addition,Malnutrition Universal Screening Tool[27]can be used for nutritional screening in adult patients with tumor.Body weight or body mass index is important indicators of nutrition screening,which can be used alone or as one of the indicators in nutrition screening tools.In addition to the above screening tools and indicators,the ESPEN guidelines also suggest that,when conditions permit,instruments such as dual-energy X-ray absorptiometry or bioelectrical impedance spectroscopy should be used for body composition analysis to help improve patients’ clinical outcomes.
CONCLUSION
This study results show that there is not yet specific guidelines on nutritional screening for patients with head-and-neck cancer formed at present.We summarize the best evidence for nutritional screening for patients with the head-and-neck cancer,with a view to providing evidence-based basis for standardized nutritional management program for patients with head-and-neck cancer formulated or perfected by medical institutions.As only one guideline in this study is from China,and the rest are from other countries,the applicability and effectiveness of some evidence in the domestic population still need to be further explored and studied.The medical institutions need to consider the characteristics of the hospital,the working environment,the obstacles and promoters of the application of evidence,the patient’s will,and other factors,translate the above evidence into quality review indicators,and fully consider whether each item of evidence is feasible and appropriate.Moreover,it is necessary to train medical staff on nutrition screening,early identification of patients with high nutritional risk,ultimately ensure the smooth application of evidence in clinical practice,and guide medical staff to solve the clinical nutritional problems of patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
杂志排行

Journal of Integrative Nursing的其它文章
- Effect of a traditional Chinese medicine theory-based mobile app on improving symptoms in patients with type 2 diabetes mellitus:A randomized controlled trial
- Comparison of in-vial exhaust method versus conventional exhaust method in the injection of COVlD-19 vaccine
- Analysis of licensure examination anxiety and its influencing factors among undergraduate nursing students
- Correlation between psychological resilience and burnout among female employees in a shopping mall in Xi Xian New Area,China:A cross-sectional survey
- Status quo and influencing factors of comfort with touch among nursing staff in rehabilitation department:A cross-sectional study
- Musculoskeletal problems and expressed practices of body mechanics among nursing officers at All lndia lnstitute of Medical Sciences Jodhpur,Rajasthan,lndia