Fluorescent cholangiography: An up-to-date overview twelve years after the first clinical application
2021-10-12AntonioPesceGaetanoPiccoloFrancescaLecchiNicolFabbriMicheleDianaCarloVittorioFeo
Antonio Pesce, Gaetano Piccolo, Francesca Lecchi, Nicolò Fabbri, Michele Diana, Carlo Vittorio Feo
Abstract Laparoscopic cholecystectomy (LC) is one of the most frequently performed gastrointestinal surgeries worldwide.Bile duct injury (BDI) represents the most serious complication of LC, with an incidence of 0.3%-0.7%, resulting in significant perioperative morbidity and mortality, impaired quality of life, and high rates of subsequent medico-legal litigation.In most cases, the primary cause of BDI is the misinterpretation of biliary anatomy, leading to unexpected biliary lesions.Near-infrared fluorescent cholangiography is widely spreading in clinical practice to delineate biliary anatomy during LC in elective and emergency settings.The primary aim of this article was to perform an up-to-date overview of the evolution of this method 12 years after the first clinical application in 2009 and to highlight all advantages and current limitations according to the available scientific evidence.
Key Words: Laparoscopic cholecystectomy; Bile duct injury; Biliary anatomy; Fluorescent cholangiography; Indocyanine green
INTRODUCTION
Laparoscopic cholecystectomy (LC) is one of the most frequently performed gastrointestinal surgeries worldwide.Bile duct injury (BDI) represents the most serious complication of LC, with an incidence of 0.3% to 0.7%, resulting in significant perioperative morbidity and mortality, impaired quality of life, and high rates of subsequent medico-legal litigation[1,2].In most cases, the primary cause of BDI is the misinterpretation of biliary anatomy, leading surgeons to unexpected biliary lesions(71%-97% of all cases)[3,4].Various methods have been proposed and used to prevent iatrogenic biliary tract lesions[4].Among them, near-infrared fluorescent cholangiography (NIRF-C) is widely spreading in clinical practice to delineate biliary anatomy during LC in elective and emergency settings.It is becoming one of the most popular and promising clinical applications in minimally invasive surgery[5,6].In 2006, Stiles BMet al[7] first proposed fluorescent cholangiography in a mouse model by exploiting the unique auto fluorescent properties of bile for the intraoperative identification of the biliary anatomy in mice.The first application in humans was performed and described byIshizawa et al[8] a few years later (2009).This classical method involves the intravenous injection of indocyanine green (ICG) dye before surgery.ICG binds to plasma proteins, with albumin as the principal carrier (95%),and is eliminated exclusively by the liver.The excitation of ICG by means of nearinfrared light causes fluorescence, thereby delineating the anatomy of the biliary elements in real time.This innovative method was introduced as a means to prevent bile duct injuries during LC due to a better visualization of biliary anatomy during dissection.In 2015, we performed a systematic review of available studies by analyzing the efficacy of the novel technique in detecting bile duct structures during surgery.Detection rates of the biliary anatomy in 590 pooled patients were as follows:Cystic duct (CD) 96.2% (94.7%-97.7%), common hepatic duct (CHD) 78.1% (74.8%-81.4%), CD-CHD junction 72.0% (69.0%-75.0%), and common bile duct (CBD) 86.0%(83.3%-88.8%)[9].Overall, these preliminary studies indicated that ICG fluorescence cholangiography is highly sensitive for the detection of extrahepatic biliary anatomy and may facilitate the prevention of bile duct injuries.Over the years, several singlecenter experiences from different countries[10-12] have been published regarding the usefulness of ICG fluorescence cholangiography in detecting biliary anatomy and analyzing patient outcomes after LC.The level of scientific evidence on ICG fluorescence cholangiography remains low.However, recent studies have significantly propelled the literature forward.
The primary aim of this article was to perform an up-to-date overview of the evolution of this method 12 years after its first clinical application and to highlight all the advantages and current limitations according to the available scientific literature.
TECHNIQUES
ICG administration can be performed in two different ways.The classical method described by Ishizawa Tet al[8] in 2009 consists of the intravenous injection of ICG 30 min before surgery.Biliary visualization should be obtained prior to any dissection,during the dissection of the hepatocystic triangle, and after complete dissection according to the critical view of safety (CVS) method[13,14].This approach enables surgeons to check the biliary anatomy intraoperatively at any time.Recently, Dip Fet al[15] summarized 10 important steps for the correct performance of fluorescent cholangiography during LC.The first two steps involve ICG intravenous administration and complete exposure of the hepatoduodenal ligament prior to any dissection.The primary objective of step 3 is the localization of the main biliary structures after the partial dissection of the hepatocystic triangle.Steps 4-7 are characterized by the identification of the CD, gallbladder-CD junction, CD-CHD junction, and CBD; step 8 is the identification of the cystic artery, in some cases by repeating ICG injection for fluorescent angiography to detect any anatomical arterial variations; step 9 is called“time-out”, and it consists of the re-evaluation of the CVS before clipping and cutting any structures (as shown in Figures 1-2).After completing gallbladder removal, nearinfrared (NIR) light should be turned on to identify any potential biliary leaks from the liver bed (step 10).At the current stage, there are two unresolved issues regarding NIRF-C,i.e., the dose and the time required to obtain an optimal bile duct-to-liver fluorescence ratio >1.An elevated background liver signal may hinder the correct visualization of biliary anatomy.The dose and the time of administration of ICG are quite variable, as reported in the literature[16].A recent study with data from the European Fluorescence Image-Guided Surgery (FIGS) registry[17] has shown a wide disparity in ICG dose and timing in NIRF-C across different European countries.Boogerd Let al[18] demonstrated that the highest bile duct-to-liver ratio was achieved 3 to 7 h after administration of 5 mg of ICG and 5 to 25 h after administration of 10 mg of ICG.Another study by Zarrinpar Aet al[19] confirmed that a single dose of 0.25 mg/kg administered at least 45 min prior to visualization of the hepatocystic triangle facilitates intra-operative anatomical identification.Recently, Chen Qet al[20]demonstrated that the optimal effect of fluorescent cholangiography can be achieved by injecting 10 mg of ICG 10 to 12 h prior to surgery.Matsumura Met al[21]recommended the administration of 0.25 mg/kg ICG on the evening before surgery, as it may increase bile duct detectability in fluorescence cholangiography during LC.Based on our experience, we think that the administration of ICG 45 to 60 min before surgery is—from a logistical point of view - more practical since most patients are usually hospitalized on the same day as the surgical procedure.Indeed, the debate remains open, and a consensus conference may help the surgical community.

Figure 1 Intra-operative real-time identification of biliary structures in a cirrhotic patient, with visible light to the left and NIRF-C to the right.A: Pre-dissection visualization of biliary anatomy; B: After complete dissection.One can observe the posterior implantation of the cystic duct on the common hepatic duct.CD: Cystic duct; CHD: Common hepatic duct; CBD: Common bile duct.

Figure 2 Classical extrahepatic biliary anatomy with identification of the right and left hepatic ducts using near-infrared fluorescent cholangiography.CD: Cystic duct; CHD: Common hepatic duct; RHD: Right hepatic duct; LHD: Left hepatic duct.
The direct injection of ICG into the gallbladder is a technique that allows overcoming the strong background signal in the liver.Liu YYet al[22] were the first to describe intracholecystic ICG administration during LC in a porcine model, proving the feasibility and usefulness of this technique to achieve adequate CVS.Few clinical studies of NIR cholecystocholangiography with direct ICG injection into the gallbladder were conducted, namely, two case reports, one case-control study, and a few prospective cohort studies, for a total of 80 patients, of whom 49 underwent surgery for symptomatic cholelithiasis and 31 for acute cholecystitis[22-26], as summarized in Table 1.

Table 1 Cholecysto-cholangiography with direct intra-gallbladder indocyanine green injection
Liu YYet al[22] and Škrabec Cet al[23] conducted the two widest studies, namely, a prospective cohort study of 46 patients and a case-control study including 20 patients,respectively.The authors described two different routes for intracholecystic ICG injection,i.e., percutaneous transhepatic gallbladder drainage (trans-PTGBD) and intra-operative direct gallbladder puncture.A 1 mL amount of an ICG bile solution was used (ICG concentration = 0.025 mg/mL) made from a combination of 9 mL of bile mixed with 1 mL of a preparation of ICG and sterile water at a concentration of 0.25 mg/mL.NIR cholecystocholangiography with direct gallbladder injection was more successful in acute cholecystitis patients who underwent early or interval LC after the preliminary positioning of a PTGBD.Among all cases reported in the literature, only one patient required conversion to open cholecystectomy due to acute necrotic cholecystitis, which precluded safe laparoscopic dissection.
Intracholecystic ICG injection provides relevant advantages compared to intravenous NIR cholecystocholangiography, such as the real-time visualization of the biliary anatomy, including the gallbladder neck and Hartmann’s pouch, which are safe landmarks to start the dissection.Additionally, the timing of ICG injection is irrelevant, and small dosages can be used.
The downside of direct ICG injection lies in the possibility of ICG bile leakage or lymph spillage during gallbladder dissection for acute cholecystitis, as ICG may enter through the necrotic gallbladder mucosa into the submucosal lymphatic drainage.In regard to the widest experiences reported in the literature[22,23], ICG bile leakage occurred in six patients in whom ICG was directly injected through a fine-needle puncture.Another limitation lies in the absence of progression of the dye into the CD in cases of stone obstruction.
Based on the available data, we suggest that larger studies are necessary to validate the technique of intracholecystic ICG injection for NIR fluorescent cholangiography.
ICG FLUORESCENT CHOLANGIOGRAPHY IN PATIENTS WITH ACUTE CHOLECYSTITIS
Early LC is the gold standard treatment for patients with mild (grade I) and moderate(grade II) acute cholecystitis who have no response to initial (within 24 h) conservative treatment if performed within 72 h from the onset of symptoms according to 2018 Tokyo guidelines[27].
Fluorescent cholangiography may be very challenging in an emergency setting,when inflammation and adhesions at the hepatoduodenal ligament may impair the identification of biliary elements during dissection.Reaching the CVS may be particularly difficult in such situations[28].
In a recent meta-analysis, Dip Fet al[29] suggested that using NIRF-C during elective cholecystectomy led to decreased BDI and conversion to open surgery compared to white light alone.However, there are limited data about its feasibility in an emergency setting.The identification of biliary structures may be challenging,especially in cases where there is an abundance of adhesions and severe inflammation of the gallbladder wall and surrounding tissues[9].
The literature contains four articles that provide data of patients who underwent LC for acute cholecystitis with NIR devices,i.e., two cohort studies[30,31], one international European registry[17], and one randomized controlled trial (RCT)[32] are reported in Table 2.

Table 2 FIuorescent choIangiography in patients with acute choIecystitis
In a large retrospective study involving 184 consecutive patients, Daskalaki Eet al[31] reported the results of 24 patients who underwent robotic cholecystectomies (RCs)with ICG fluorescence for acute and gangrenous cholecystitis.The authors evaluated the detection rate of four biliary structures,i.e., CD, CHD, CBD, and CD-CHD junction.In this subset of challenging surgical cases, the CD, CHD, CBD, and CD-CHD junction were successfully visualized in 91.6%, 79.1%, 79.1%, and 75% of cases, respectively.
Agnus Vet al[17] reported data from the Euro-FIGS database, which enrolled 314 cases from 12 European surgical centers, including patients affected by symptomatic cholelithiasis (n= 248) and patients with acute cholecystitis (n= 58).A 5-point Likert scale was used to evaluate the quality of biliary anatomy visualization before and after the dissection of the hepatocystic triangle during LC with NIR devices.When the two groups (cholelithiasisvsacute cholecystitis) were compared, lower visualization quality scores were obtained in the CD group (2.76 ± 1.9vs3.54 ± 1.6,P= 0.001) and CD-CHD junction (2.43 ± 2vs3 ± 1.9,P= 0.04) before the preliminary dissection.The impact of variable inflammation on the visualization score of the biliary tree was also confirmed by means of multivariate linear regression analysis.
Similar data have been reported in a single-blinded randomized controlled trial[32]comparing the efficacy of NIR fluorescent cholangiographyvswhite light alone.The primary objective was the structure detection rate, defined as the total number of patients in whom a particular biliary structure was detected, both before and after dissection, in each study arm, divided by the total number of patients in each arm.The authors found that the degree of gallbladder inflammation was the most important variable, affecting the detection of CD and CBD before and after dissection,respectively, and of the CD-gallbladder junction only after dissection.
The usefulness of NIRF-C was also confirmed by Yoshiya Set al[33] during LC after PTGBD in patients with severe acute cholecystitis.The ICG fluorescence cholangiography group showed a significantly shorter operative time, a lower conversion rate, and a lower proportion of subtotal cholecystectomies[33].
NIR fluorescence cholangiography in emergency cholecystectomies is a safe and useful tool to prevent BDI during LC.However, the available data require further elaboration in randomized controlled studies in larger numbers of patients with acute cholecystitis undergoing LC with the aid of intra-operative fluorescent cholangiography.
DETECTION OF BILIARY VARIANTS USING ICG FLUORESCENCE
Various reports have underlined the importance of fluorescence image-guided cholecystectomy in detecting biliary variants.Fluorescent cholangiography allows the intraoperative identification of subvesical Luschka’s ducts[34,35], aberrant bile ducts[36-38], anatomical CD variations[39], and gallbladder aberrations[40,41].
In specific studies, the diagnostic accuracy of NIRF-C in the evaluation of CD anatomy has been compared to that of magnetic resonance cholangiopancreatography(MRCP), which is the gold standard radiology diagnostic tool for the preoperative study of the biliary tree[42,43].Pesce Aet al[44] evaluated the ability of the two imaging methods to identify three selected features, namely, the insertion of CD, CDCHD junction, and CD course.The level of insertion, course, and wall implantation of the CD were achieved by means of NIRF-C with diagnostic accuracy values of 65.2%,78.3%, and 91.3%, respectively, in comparison with MRCP data.
In 2017, Diana Met al[45] prospectively evaluated the combination of three imaging modalities during robotic cholecystectomy,i.e., virtual reality 3D modeling of MRCP,NIRF-C, and intraoperative cholangiogram (IOC).Surprisingly, expert hepatobiliary radiologists missed 5 out of 8 anatomical variants on preoperative MRCP, while surgeons were able to identify all variants through a virtual surgical exploration complemented with intraoperative fluorescent cholangiography.
In another observational study in 65 patients by Hiwatashi Ket al[46], the authors found a statistically significant correlation between the delineation of CD using ICG cholangiography and preoperative MRCP.
Based on the current scientific literature (RCTs shown in Table 3), we strongly believe that NIRF-C is a useful tool to detect biliary variants that could guide surgeons during dissection to prevent any major bile duct lesions.

Table 3 Recruiting randomized controIIed triaIs using indocyanine green fIuorescence choIangiography
FLUORESCENT CHOLANGIOGRAPHY VS STANDARD INTRAOPERATIVE CHOLANGIOGRAPHY
NIRF-C has been recognized as providing some advantages over conventional radiographic IOC, such as feasibility and safety, real-time visualization of biliary anatomy with safer dissection of the hepatocystic triangle, the lack of a learning curve,reduced X-ray exposure, and reduced costs and operative times[5,47-49].In a Danish randomized controlled single-blind clinical trial[50], the authors compared NIRF-CvsIOC.They demonstrated that fluorescent cholangiography has the same capacity to identify the CVS, and is significantly faster and easier to perform than X-ray cholangiography[50].In a recent meta-analysis by Lim SHet al[51], the authors concluded that there was no difference in the visualization of the CD, CBD, and CD-CBD junction using ICG fluorescence cholangiography compared to IOC.However, the ICG group reported increased rates of CHD visualization.
Dip Fet al[52] analyzed medical costs and stated that the median cost of ICG fluorescence cholangiography was cheaper than that of IOC (13.97 ± 4.3vs778.43 ± 0.4 USD per patient,P= 0.0001).
Quaresima Set al[53] proposed that NIRF-C is a safe and effective procedure for the early recognition of anatomical biliary landmarks, with an important reduction in operative times compared to LC with intraoperative cholangiography.
In an article by Prevot Fet al[54], the authors analyzed the ability to identify the CD,the CD-hepatic duct junction, and the CBD using fluorescence in comparison with standard IOC.The results of this study suggested that ICG fluorescence cholangiography is more effective than IOC in identifying the biliary tract after dissection.
In conclusion, we believe that there is considerable scientific evidence supporting the usefulness of NIRF-C with important advantages over conventional intraoperative cholangiography.NIRF-C represents a powerful real-time diagnostic tool for the detection of extrahepatic biliary anatomy during LC.Advantages and current limitations are summarized in Table 4.
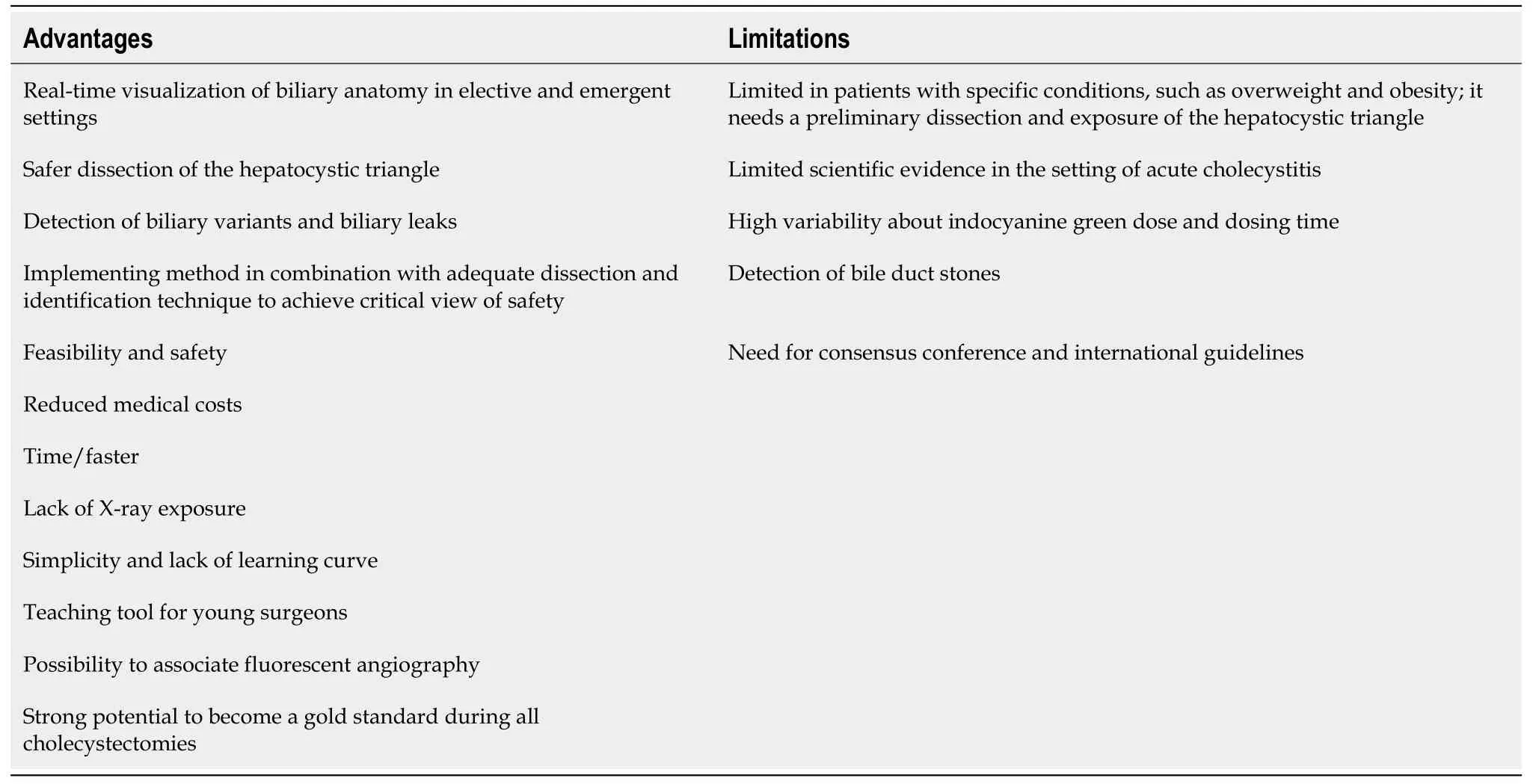
Table 4 Advantages and current limitations of fluorescent cholangiography in comparison to intraoperative cholangiogram and laparoscopic ultrasonography
FLUORESCENT CHOLANGIOGRAPHY IN OBESE PATIENTS
As reported in previous studies[9,31,55-57], the presence of dense adipose tissue surrounding the hepatocystic triangle may negatively affect the visualization of extrahepatic biliary tract using fluorescence.Obesity may represent a limitation of NIRF-C because NIR light has a penetration capability of only 5 to 10 mm[7-9].In 2016,Dip Fet al[58] conducted a prospective study to evaluate the accuracy of NIRF-C in obesevsnon-obese patients.The results showed no difference in hepatic duct, CBD, or accessory duct detection rates between the two groups (P= 0.09, 0.16, and 0.66,respectively) before and after dissection of the hepatocystic triangle.
On the other hand, a German study[59] suggested that a BMI > 25 kg/m² and male sex significantly reduced the identification rate of CD before dissection of the hepatocystic triangle.
In a randomized controlled multicenter trial[32] comparing ICGvswhite light alone,an increased BMI was associated with a reduced detection of most biliary structures in both groups, especially before dissection.
In general, our opinion is to use fluorescence to perform a complete dissection of the hepatocystic triangle in overweight and obese patients to obtain a good quality visualization of the biliary anatomy.In difficult cases where the surgeon is not able to clearly check the biliary anatomy, the surgeon should respect a sufficient thickness between the dissecting site and the main bile duct by working close to the gallbladder infundibulum to avoid unexpected biliary lesions.NIR imaging cannot be considered a substitute for good dissection and structure identification.
FLUORESCENT INCISIONLESS CHOLANGIOGRAPHY AS A TEACHING TOOL FOR YOUNG SURGEONS
It is well established that the risk of BDI correlates with the quality of the procedure performed, rather than the number of cases seen by the surgeon[1,2].A clear identification of the biliary anatomy is crucial to perform a safe cholecystectomy and achieving CVS is now being taught as a key step of the operation to young surgeons[4,13].In a recent randomized controlled trial[60], the time to achieve CVS from the gallbladder fundus retraction was measured by analyzing different levels of difficulty.The mean time, expressed in minutes, to achieve CVS was 22.3 ± 12.9 in the ICG-LC group (n= 30) and 22.8 ± 14.3 in the conventional LC group (P= 0.867).The authors concluded that fluorescent cholangiography may be a useful tool in difficult LC and in surgical training.A randomized controlled multicenter Dutch trial (FALCON trial)regarding the time to visualize CVS with NIRF-C compared to white light alone is still ongoing[61].However, biliary structures are not always easily visualized laparoscopically.Fluorescence incisionless cholangiography may be a promising tool for training new surgeons in safe laparoscopic cholecystectomies by helping with biliary anatomy identification.To date, few studies have been conducted regarding the potential role of this technique in surgical training programs[62-64].
In 2016, Roy Met al[62] tested the ability of surgical students and residents to identify major biliary structures at NIR light.Participants were shown pictures taken at the same stage of hepatocystic triangle dissection in 10 cases of LC, first with NIR light and then with Xenon white light.Both students and residents had a higher success rate of biliary tree identification with NIR fluorescence cholangiography.The authors also underlined the importance of NIRF-C to achieve appropriate intraoperative communication to guide residents, as it allows us to point out glowing structures in real time.
Similarly, in 2020, Rungsakulkij Net al[63] conducted a study to investigate the beneficial impact of fluorescence cholangiography on the ability of surgical residents to identify biliary structures.Participants were asked to identify the CD and artery,CBD and CHD in five LC videos, first without fluorescence, and then with NIRF-C.The results showed a higher misidentification rate among surgical residents in the without-FC modality than in the with-FC modality, proving the benefit of the technique among trainees.
In a study by Pesce Aet al[47] on the usefulness of fluorescent cholangiography for biliary anatomy identification, surgical residents completed a survey on the perceived benefits of the technique.Responses were measured with a Likert scale.All participants agreed that NIRF-C facilitates the dissection of the hepatocystic triangle,hence being a useful adjuvant to training programs; 92% of respondents found the method easy to perform; 88% declared that it was effective in visualizing the biliary tree, and 84% found that the image quality was good.Consequently, residents consider the novel method a useful tool to visualize biliary anatomy and perform a safe dissection of the hepatocystic triangle, decreasing the risk of BDI.
From these experiences, it is safe to conclude that there is a large consensus regarding the beneficial role of NIRF-C in the training process of young surgeons.However, larger studies proving the benefits on the skills of surgical residents are required for the technique to be routinely performed in a teaching setting.
FLUORESCENT CHOLANGIOGRAPHY AND DETECTION OF BILIARY STONES
To date, there is no evidence that FC can effectively identify CBD stones by replacing IOC[64,65].Intraoperative laparoscopic ultrasound (IOUS) could well represent a valid alternative to IOC in the detection of CBD stones[66,67].Current limitations are related to the difficult learning curve and the lack of randomized controlled trials[66].According to Daskalaki Met al[27], ICG fluorescence cholangiography can help to detect CD dilation and gallbladder stones (as shown in Figure 3), but it cannot rule out the presence of CBD stones.In a recent correspondence by Labil PL and Aroori S published inBr J Surg[65], the authors suggested performing an RCT comparing IOUS with X-ray and/or fluorescence cholangiography in LCto detect a difference in the rate of bile duct stone identification, as well as viewing the critical junction.

Figure 3 Identification of cystic duct stones by means of fluorescence.
NIRF-C AND ROBOTIC CHOLECYSTECTOMY
Since the introduction of the robotic surgical platform in the 2000s, approximately 10%of all cholecystectomies are performed robotically[68] today.ICG technology was soon incorporated into the robotic platform, and the first case series involved patients who underwent single-incision or multiport robotic cholecystectomy (RC) with NIRF-C, as summarized in Table 5.

Table 5 Studies reporting robotic cholecystectomy and near-infrared fluorescent cholangiography
In a large retrospective cohort study including 184 patients, Daskalaki Det al[31]proved the feasibility of this technique.The four main biliary structures (CD, CHD,CD-CHD junction, CBD) were recognized using fluorescence imaging in 83% of cases.At least one structure was visualized in 99% of cases.Similar data have been reported by other authors[55,69-71].
Spinoglio Get al[70] showed that after dissection of the hepatocystic triangle, the visualization rates for each structure (CD, CHD, CD-CHD junction, CBD) increased to 97%.In addition, the rate of patients with two or three ducts visualized with NIR fluorescent cholangiography increased from 91% to 97% and from 86% to 95% before and after dissection, respectively.
In recent years, some authors compared data of patients who underwent robotic cholecystectomy with the use of ICGvsconventional LC[72,73].In a retrospective cohort study, Sharma Set al[72] analyzed 287 consecutive cases, including 96 RCs and 191 LCs.The authors found a lower open conversion rate in the robotic cohort (2.1%vs8.9% in LC), although this difference was not statistically significant.
Gangemi Aet al[73] conducted a case-control study comparing the outcomes of ICG-aided RCvsLC at the University of Illinois (Chicago, United States).The authors reported a statistically significant difference between RC performed with the help of ICG and traditional LC in terms of the overall open conversion rate (0.15%vs4.5%),open conversion rate in the acute setting (0.76%vs9.57%), mean blood loss during surgery (14.37 mLvs21.08 mL), and minor biliary injury rate (0.15%vs1.04%).Additionally, a biliary tree anomaly was found in 2.07% of patients who underwent ICG-aided RC compared to 0.69% of patients who underwent LC with conventional intraoperative cholangiography.
Recently, Dipet al[29] conducted a meta-analysis evaluating whether NIFC with ICG could reduce conversion to open surgery and bile duct injuries during laparoscopic and robotic cholecystectomy.Patients who underwent ICG-aided RC showed a marked reduction in the rate of conversion to open surgery compared to RC without NIFC (weighted rate: 12/10.000vs322/10.000).Similar data were reported in the ICGaided LC group (weighted rate: 23/10.000vs255/10.000).For BDI, a reduction was reported in the ICG-aided LC group compared to LC without NIFC (weighted rate:23/10.000vs255/10.000), while no difference was noted regarding RC with and without NIFC.In conclusion, we believe that the use of NIRF-C may reduce the conversion rate in both minimally invasive procedures, laparoscopic and robotic cholecystectomy, while the reduction rate only exists in LC for BDI.However, further studies are required.
CONSENSUS CONFERENCES AND GUIDELINES
During the 4th International Congress of Fluorescence-Guided Surgery in Boca Raton,Florida in 2017, Dip Fet al[74] conducted a pilot survey of 51 attending surgeons who routinely performed laparoscopic cholecystectomies to identify their surgical practice and perceptions of intraoperative fluorescent cholangiography.Ten experts in ICG fluorescence-guided LC from North and South America, Europe, and Asia designed the survey for conference attendees.Seventy-eight percent of respondents underlined the importance for surgeons of having a noninvasive, simple, and reproducible diagnostic tool to identify the extrahepatic biliary anatomy in real time.In general,they recommended the routine use of NIRF-C during LC as a complimentary imaging technique, and 93.3% of them felt that the procedure would be useful in surgical training programs.
In a recent state-of-the-art consensus conference on the prevention of BDI during cholecystectomy published inAnnals of Surgery[75], a pool of experts from five surgical societies (Society of Gastrointestinal and Endoscopic Surgeons, Americas Hepato-Pancreato-Biliary Association, International Hepato-Pancreato-Biliary Association,Society for Surgery of the Alimentary Tract, and European Association for Endoscopic Surgery) analyzed the scientific evidence among surgical practices to prevent bile duct injuries.At question 5B,i.e., “Should intraoperative NIR biliary imaging with white light versus white light biliary imaging alone be used to limit the risk or severity of BDI during LC?”, they answered the following question: We suggest that the use of NIR imaging may be considered an adjunct to white light alone to identify the biliary anatomy during cholecystectomy (conditional recommendation, very low certainty of evidence).
However, in a Delphi survey of 19 international experts in fluorescence-guided surgery attending a 1 d consensus meeting in Frankfurt, Germany in September 2019,fluorescence imaging was almost unanimously perceived to be both effective and safe across a broad range of clinical settings[76].No specific recommendations were given for fluorescent cholangiography.Moreover, the safety of ICG dye has been underlined:the risk of adverse reactions to ICG injection, such as anaphylactic shock, is very small(approximately 0.003% at doses exceeding 0.5 mg/kg) according to the literature data[9,77].
CONCLUSION
The results of the current up-to-date overview confirmed the efficacy of ICGfluorescence cholangiography in detecting biliary anatomy, its importance as a teaching tool for young surgeons, and the effects on the reduction of conversion rate and BDI, even if further considerable research remains necessary to optimize its use.This frontier method has enormous potential to become the gold standard during all cholecystectomies in elective and emergency settings due to its safety and limited costs.However, clear clinical guidelines are necessary for the surgical community.
杂志排行

World Journal of Gastroenterology的其它文章
- Histone methylation in pancreatic cancer and its clinical implications
- Hepatitis B virus infection and hepatoceIIuIar carcinoma in sub-Saharan Africa: ImpIications for eIimination of viraI hepatitis by 2030?
- Liver disease in the era of COVID-19: Is the worst yet to come?
- Treatment of hepatitis B virus infection in chiIdren and adoIescents
- Basic Study CircRNA_0084927 promotes colorectal cancer progression by regulating miRNA-20b-3p/glutathione S-transferase mu 5 axis
- Basic Study ExosomaI microRNA-588 from M2 poIarized macrophages contributes to cispIatin resistance of gastric cancer ceIIs