Physical activity and its relationship with COVID-19 cases and deaths:Analysis of U.S.counties
2021-10-09GeorgeCunningham
George B.Cunningham
Center for Sport Management Research and Education,Department of Health and Kinesiology,Texas A&M University,College Station,TX 77843,USA
Abstract Purpose:The study was to examine county-level associations of physical activity with coronavirus disease 2019(COVID-19)cases and deaths,per 100,000 county residents.Methods:Data were collected from publicly available data sources for 3142 counties and equivalents,including the District of Columbia.Subjective health ratings,percentage uninsured,percentage unemployed,median household income,percentage female residents,percentage White residents,percentage of residents 65 years of age or older,and rural designation served as controls.Results:The two-level random intercept regression showed that physical activity rates at the county level were statistically and negatively associated with COVID-19 cases and deaths.Additional analyses showed that physical activity rates moderated the relationship between cases and deaths,such that the relationship was strongest when physical activity rates were low.Conclusion:The results presented here offer empirical evidence of the benefits of county-level physical activity during a pandemic.Implications for public health and physical activity provision are discussed.
Keywords: Coronavirus disease 2019;Deaths;PA
1.Introduction
Given the physical,social,psychological,and economic tolls of the coronavirus disease 2019(COVID-19)pandemic,1-5scientists around the world have staunchly pursued an understanding of factors contributing to virus-related morbidity, hospitalizations, and mortality.Personal characteristics,including age,gender,and race,as well as comorbidities,including diabetes,obesity,respiratory illnesses, and hypertension, are salient predictors.6,7These effects noted,health behaviors and outcomes are not just a function of the individual but,instead,are also shaped by environmental determinants.8,9Consistent with this perspective, social and community factors that contribute to COVID-19 cases and deaths include public health ordinances,10structural inequalities,11collective racial biases,12and socioeconomic disparities,13among others.
Missing from the examination of social and environmental factors potentially related to COVID-19 cases and deaths is a focus on physical activity (PA) among community members.Systematic reviews show that most of the scholarship in this area has focused on PAduringthe pandemic amongindividuals.14For example,people around the world were more likely to lead sedentary lives,especially during lockdowns;and these findings were prevalent among countries hit hardest by the pandemic.15-17PA decreases were linked with corresponding reductions in psychological well-being18and subjective health.15Such inactivity has the potential to have lasting negative effects on people’s physical health.19As a result, sport managers and public health officials have identified creative solutions for being active at home or in otherwise physically distanced settings.20
Though examination of individual PA during the pandemic is important, a sole focus on that level of analysis necessarily ignores the impact of community norms and behaviors.21This is an important distinction because community-level PA is associated with better health and lower obesity rates among members of a community as a whole.22-24These findings are consistent with related research showing that PA can help reduce the incidence of many COVID-19 risk factors, including obesity, hypertension, heart disease, and respiratory illnesses.25,26Recognizing this possibility, Simpson and Katsanis25noted,“the available scientific evidence from other viral infections would indicate that physically active people will have less severe symptoms, shorter recovery time, and may be less likely to infect others they come into contact with.”25
Applied to the aggregate level, these suppositions25suggest that communities with higher levels of PA might also see fewer COVID-19 cases and deaths.The purpose of this study was to examine these possibilities through an analysis of county-level data in the US.Specifically,it was hypothesized that county-level PA rates would be negatively related to COVID-19 cases(Hypothesis 1)and COVID-19 deaths(Hypothesis 2).
2.Methods
2.1.Data sources and variables
Data were collected for counties and county-equivalents(boroughs,parishes,and the District of Columbia;n=3142)in the US.A county,or equivalent,represents a major administrative unit within a given state,27and there are 3243 such units in U.S.states and territories.The current analysis focused only on counties in U.S.states, and all 50 states were represented.All data were gathered from publicly available sources,as outlined in the following sections.The study met the research guidelines of Texas A&M University.
2.1.1.COVID-19 cases and deaths
Data related to COVID-19 cases and deaths were gathered from the USAFacts Website: https://usafacts.org/visualizations/coronavirus-covid-19-spread-map/.The website’s data are used by a variety of agencies and organizations,including the Centers for Disease Control and Prevention and Google, and other researchers examining predictors of COVID-19 cases and deaths have also used this database.28,29The site offers details on the data collection process (https://usafacts.org/articles/detailedmethodology-covid-19-data/), which involves collecting daily data from state and county websites and dashboards.The data are collected through scraping or manual entry.Used in this study were the cumulative COVID-19 cases and deaths, respectively,from January 20, 2020 to November 30, 2020 (a period of 314 days).Each count was then converted to reflect the number of cases(Cases)or deaths(Deaths)per 100,000 county residents.
2.1.2.PA
PA data were gathered from the 2020 County Health Rankings and Roadmaps (https://www.countyhealthrankings.org), a Robert Wood Johnson Foundation-supported initiative that provides health data for all U.S.counties.Drawing from the Behavioral Risk Factor Surveillance Survey, the site provides the percentage of people age 20 or older who reported no PA in the previous month.The specific item reads: “During the past month, other than your regular job, did you participate in any PAs or exercises such as running, calisthenics, golf, gardening,or walking for exercise?”30For this study, that measure was reverse scored and labeledPercent Activeto represent the percentage who had any level of activity.As discussed in more detail in the limitations section,this measure represents the lowest possible threshold of PA and should not be interpreted as meeting activity guidelines.
2.1.3.Controls
A number of controls were also included,all of which either impact residents’health in general or are related to COVID-19 prevalence.These data were collected from the aforementioned County Health Rankings and Roadmaps website.A number of comorbidities are associated with COVID-19 risks and mortality,31so subjective health ratings (PoororFair Health) served as the first control.Others have also used this measure when examining residents’ health.32,33The lack of insurance is also linked with COVID-19 risks,34soUninsuredserved as a control.Relatedly,economic instability is a health risk factor,35so the percentage of unemployed county residents(Unemployed) and the natural log of the median householdIncome(log income)served as controls.Finally,a host of personal demographics are related to health outcomes and COVID-19 risk and mortality.12,36,37Thus, the percentage of residents who were female (Female residents), White (White residents), and age 65 or older (65 or older), as well as the rural designation of the county(Rural)all served as controls.
2.2.Empirical strategy
Means, SDs, and bivariate correlations were computed for all variables.As counties are nested within states, the observations are not independent.That is,even though counties are independent administrative units,state policies and characteristics might influence health behaviors and outcomes at the county level.38Multilevel modeling is appropriate in such instances.21,39Other options,such as ordinary least squares regression,result in a misestimation of SEs and inflated Type I error.40Therefore, two-level random effect regression models using SPSS (Version 27.0; IBM Corp.,Armonk, NY,USA)were used to test the hypotheses.Restricted maximum likelihood estimation was used to estimate the models.41,42The state level(as represented by the Federal Information Processing Standard code)was specified as a random effect,and all other variables were specified as fixed effects.Finally,in presenting the results,the intraclass correlation is included,as well as Akaike’s information criterion and Schwarz’s Bayesian criterion.
3.Results
3.1.Descriptive statistics
Descriptive statistics are shown in Table 1.Results indicate that counties had, on average, 4577.97 ± 2410.86Casesper 100,000 residents and 78.54±71.46Deathsper 100,000 residents through the end of November 2020.Many of the county residents reported being physically active: 72.63% ± 5.70%.Finally, county-levelPAheld a significant, negative bivariate correlation with bothCases(r=-0.14)andDeaths(r=-0.23).
3.2.Hypothesis testing
Results of the two-level random intercept regression models are shown in Table 2.Focusing onCases, the unconditional means model demonstrated both county-level(Level 1)and statelevel (Level 2) differences in the intercepts, suggesting that the cumulative COVID-19 cases per 100,000 residents varied based on the state and the counties within a state.The intraclass correlation (ρ=0.54) illustrates the appropriateness of including the state in the model as a random second-level variable.
Many of the controls had significant effects.Counties with a high proportion of people in fair or poor health,with many uninsured residents, with lower household incomes, with more men,with more racial minorities,and in urban settings saw more cases per 100,000 residents.In terms of hypothesis testing, results of the full model show thatPAheld a significant,negative association withCases(estimate=-21.95, SE=7.11,p< 0.01); thus,Hypothesis 1 was supported.
Table 2 also provides the results forDeaths.The unconditional means model is examined first, with results showing both county-level and state-level differences in intercepts.That is, COVID-19 deaths per 100,000 county residents varied based on the state and the counties within the states.The intraclass correlation (ρ=0.28) demonstrates that the state should be included as a random second-level variable in the model.
Many of the covariates were significantly related toDeaths.Counties where residents had lower household incomes, were employed, were racial minority, and age 65 or older were all related to increased COVID-19 deaths.Further, results of the full model support Hypothesis 2:after taking into account the controls and state-level effects,PAheld a significant, negative association withDeaths(estimate=-0.72,SE=0.27,p<0.01).
3.3.Supplemental analysis
Table 1 shows that the relationship betweenCasesandDeathsis moderate to high (r=0.45), suggesting that other factors might influence this relationship.Physical activity levels of county residents are one such factor.In this case,PAwould serve as a moderator, or a variable that potentially affects the relationship between an independent and dependent variable.43To examine this possibility, another two-level random intercept regression was computed.BothCasesandPAwere standardized to reduce the effects of multicollinearity,44and theCases×PAproduct term was then computed.As with the other analyses,restricted maximum likelihood estimation was used to estimate the models,and the state level was specified as a random effect.The controls, standardizedCasesandPAvariables, and theCases×PAproduct term were all included as fixed effects.
As shown in Table 3,results indicate thatCasesheld a significant, positive relationship withDeaths(estimate=36.37,SE=1.46,p<0.001).The main effects ofPAwere not significant in this model (estimate=-2.26, SE=1.40).However,these effects were qualified by a significantCases×PAinteraction(estimate=-5.50,SE=1.12,p<0.001).Simple slopes analysis was then computed,44and an illustrative summary of the interaction is available in Fig.1.The relationship betweenCasesandDeathswas stronger whenPAwas low (estimate=23.29, SE=1.79,p< 0.001) than when it was high(estimate=30.87,SE=1.88,p<0.001).
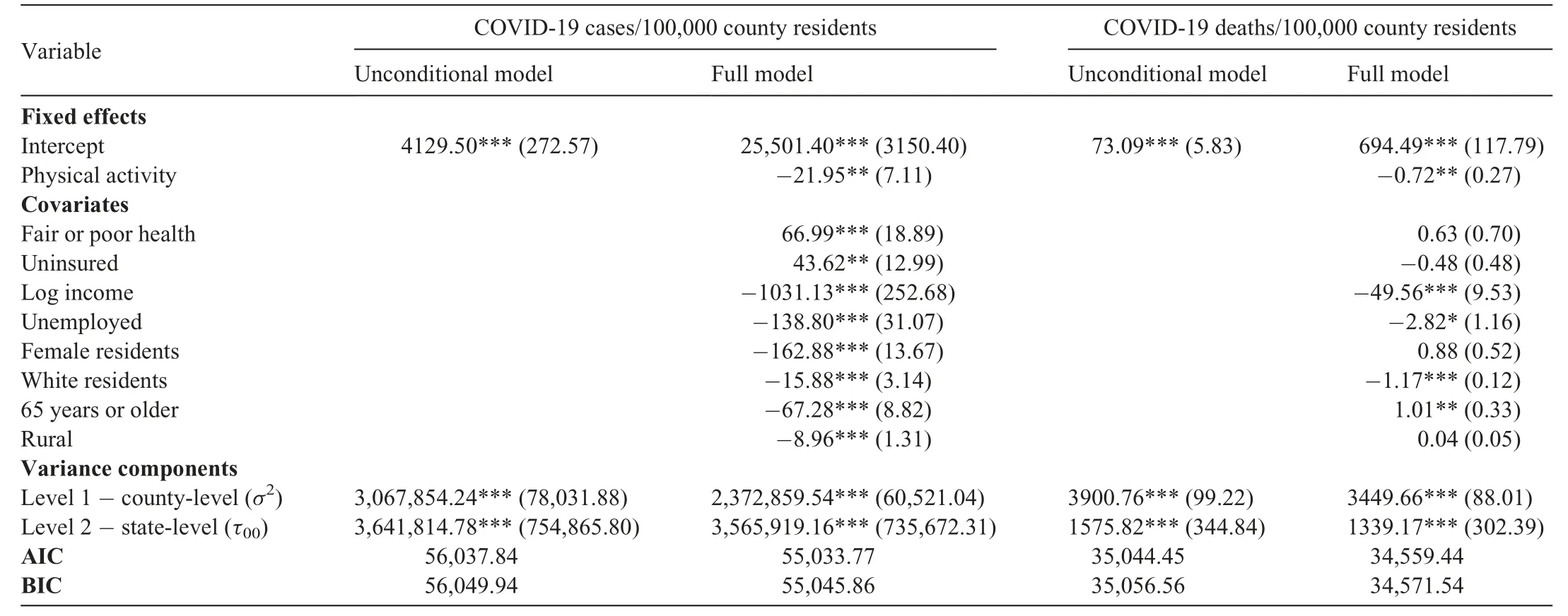
Table 2Results of two-level random intercept models with county-level physical activity predicting COVID-19 cases and deaths.
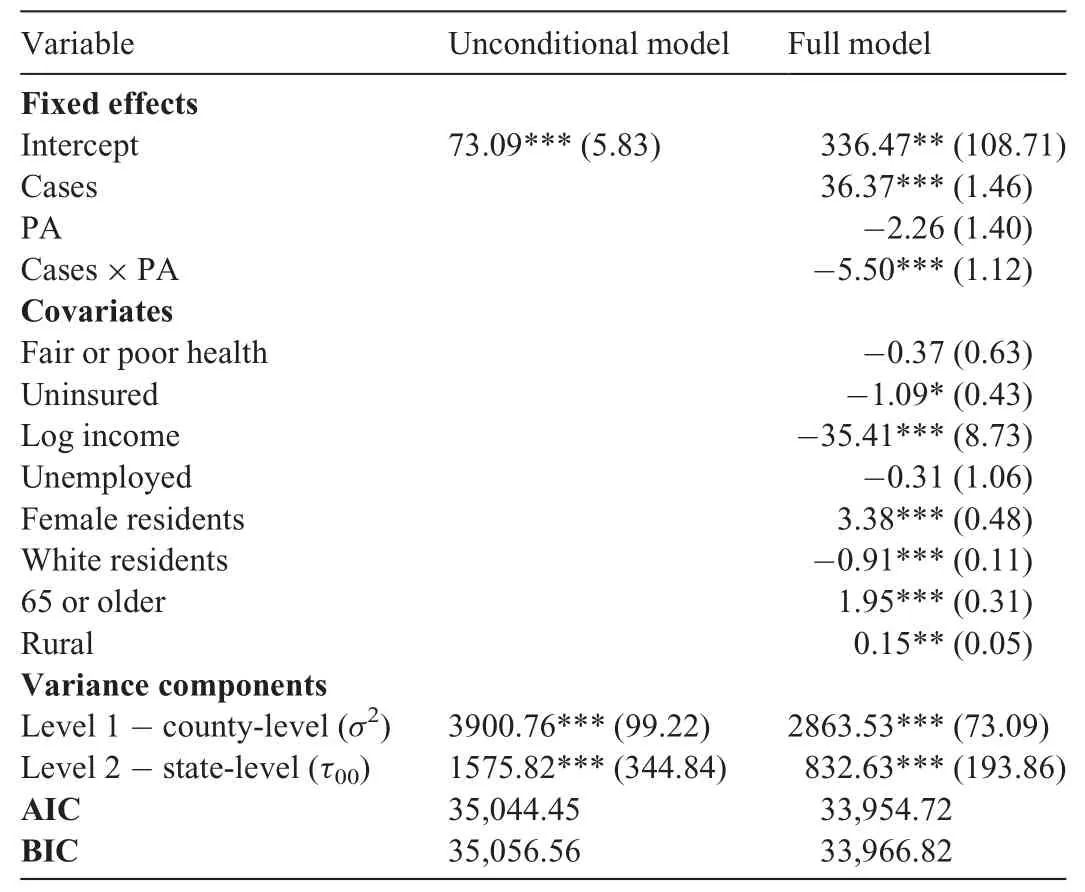
Table 3Results of two-level random intercept models examining the moderating effects of county-level physical activity PA and COVID-19 cases on COVID-19 deaths.
4.Discussion
Health behaviors and outcomes are a function of factors at multiple levels, including intrapersonal and interpersonal processes, institutional factors, community factors, and societal laws and statutes.9With respect to COVID-19, most of the scholarship has focused on intrapersonal factors,1-5but there is evidence that community and public policy factors can and do influence the incidence of COVID-19 cases and deaths.11-13,45Nevertheless, scholars have yet to examine the association of PA with COVID-19 cases and deaths.Even though PA among community members is related to better health outcomes for the community as a whole22-24and can reduce many of the comorbidities associated with COVID-19 risk,25,26examination of PA’s relationship with COVID-19 cases and deaths is missing.The purpose of this study was to rectify that gap.Consistent with the 2 study hypotheses,PA at the county level was negatively associated with both COVID-19 cases and deaths per 100,000 county residents.Additional analyses showed that PA moderated the relationship between COVID-19 cases and deaths,such that the relationship was stronger when county-level PA was low.The latter findings suggest PA can have protective effects.
The patterns identified in this study likely manifest from several factors.First, researchers have demonstrated how PA is linked with improved immune markers in several diseases related to COVID-19, including cardiovascular disease, diabetes, and obesity.46-48From this perspective,PA among community members might buffer them against disease.This was demonstrated in the current study, as county-level PA was negatively associated with COVID-19 cases.Importantly, the immune-related benefits of PA might protect county residents against serious illnesses and negative health outcomes associated with COVID-19.Simpson and Katsanis25argued as much,noting the possibility that physically active people have“less severe symptoms,shorter recovery times,and may be less likely to infect others they come into contact with”.25The results of this study offer empirical evidence for their argument: the relationship between cases and deaths decreased when PA levels were high.
From a different, more macro perspective, high county-wide PA levels might signal a culture of health and fitness concern.As a result of this culture of health and fitness,the county is likely to invest in parks,recreational facilities,and a built environment that encouragers active living.49,50The county residents,in addition to being physically active, might also take other steps to promote their health and well-being.51One outcome of a health and fitness culture particularly germane to this study is wearing a mask during the pandemic.Researchers have shown that masks can be an effective tool in combatting the spread of COVID-19;45,52nonetheless, it remains a politicized issue that is shaped, in part, by where one lives.53As such, it is possible that people living in counties where health and fitness are part of the culture or way of life might also be more willing to wear a mask.
This possibility was examined by drawing from theNew York Timescounty-level dataset related to mask-wearingaThe New York Times provided county-level estimates for mask usage,with the data publicly available on GitHub: https://github.com/nytimes/covid-19-data/tree/bde13b021e99c6b4a63fb66a6144e889cc635e31/mask-use.The estimates were based on a survey of 250,000 individuals between July 2 and July 14, 2020.Participants responded to the question: “How often do you wear a mask in public when you expect to be within 6 feet of another person?” The Times then generated estimates for the percentage of people in each county who never,rarely,sometimes,frequently,or always wear a mask in those conditions.These data were merged with the current dataset to explore the influence of physical activity on mask wearing.Bivariate correlations showed that the percentage of county residents who always wore a mask was positively related to the percentage who are physically active (r=0.23), and negatively associated with COVID-19 cases (r=-0.44) and deaths (r=-0.06) per 100,000 residents.and merging it with the current dataset.TheTimesprovides county-level estimates of the percentage of county residents who never, rarely, sometimes, frequently, or always wear a mask when they are outside and within 6 feet of another person.Analysis of these data show that the percentage of county residents who always wore a mask was positively related to the percentage who are physically active—a pattern that is supportive of the culture of health and fitness hypothesis.Even more encouraging,the percentage of people who always wore a mask was negatively associated with COVID-19 cases and deaths per 100,000 residents.
The preceding discussion should also be couched within a discussion of intersectionality and existing inequalities.54Counties with the highest percentage of residents who were at least minimally active also had higher incomes and lower unemployment rates (Table 1).In this way, some counties might have more opportunities to develop a culture of health and well-being than do others.This discussion also points to just one of the many ways in which the COVID-19 pandemic has exacerbated existing inequalities and health disparities.55,56
The results presented here offer empirical evidence of the benefits of county-level PA during a pandemic.Fortunately,with several vaccines developed and being administered as of December 2020, there appears to be a light at the end of the COVID-19 pandemic tunnel.However, other pandemics can and will occur.For their part, communities can engage in a number of steps to promote PA and related health benefits.Hood and colleagues51offer a potential framework, showing how the physical environment, social and economic factors,clinical care, and health behaviors all combine to influence a host of health outcomes, including quality of life and mortality.Hood et al.’s51work (a) demonstrates the importance of considering factors at multiple levels of analysis—consistent with a social ecological approach; and (b) identifies specific levers that public health officials can utilize in seeking to improve health.
In addition, public health experts can promote PA during the pandemic.Certainly,physical distancing requirements and lockdowns curtail many activities, but other options exist.Examples include exercising more at home,using home fitness machines, walking and running outdoors in open spaces, and practicing yoga in open spaces such as parks, among other options.20,57
Although the study makes several contributions, there are potential limitations.First, the study is cross-sectional, so results are discussed in terms of associations instead of causation.Second, the PA data measured the percentage of county residents who were physically active.However, the measure does not capture the amount or type of PA and,thus,represents the lowest threshold of activity.The data likely capture some people who were minimally active but not at levels that could provide health benefits.If this is the case, then the results underestimate the associations among PA and COVID-19 outcomes.That is, the reported associations are likely conservative.Related to this point, and recognizing that some activity is better than no activity,58it is also possible that the benefits identified in this study could vary based on the type,intensity,and duration of the PA.Future researchers should explore these possibilities.Third, though there is value in considering health and PA data at the county level,there is also variability within counties.59,60As data become available, more finegrained analyses are warranted.In addition, some health officials believe COVID-19 cases and deaths are under-reported.61Though such under-reporting would not necessarily change the pattern of findings reported here, the reader should remain mindful that the COVID-19-related mean scores might be less than those in society at large.Finally, the analyses did not include mitigation efforts occurring at county or state levels,and it is possible that the pattern of results would differ were such variables included.
Finally, there are a number of future research possibilities.As previously noted, a more fine-grained analysis of the type and nature of the county-level PA might yield fruitful insights.Second, in drawing from the social ecological perspective,researchers have identified a host of community and societal factors associated with COVID-19 cases and deaths,but additional possibilities exist.Hood et al.’s51framework offers a model from which researchers could draw.Finally,though the benefits of community-level PA are demonstrated here and in previous research, there is considerable variability among counties.More work is needed to understand how to promote and sustain PA among community residents.
Competing interests
The author declares that he has no competing interests.
杂志排行

Journal of Sport and Health Science的其它文章
- A systematic review of running-related musculoskeletal injuries in runners
- Most ankle sprain research is either false or clinically unimportant:A 30-year audit of randomized controlled trials
- Effects of plyometric vs.resistance training on skeletal muscle hypertrophy:A review
- Pacing profiles and tactical behaviors of elite runners
- Exercise attenuates bone mineral density loss during diet-induced weight loss in adults with overweight and obesity:A systematic review and meta-analysis
- Adverse associations of sedentary behavior with cancer incidence and all-cause mortality:A prospective cohort study