Enlarged folds on endoscopic gastritis as a predictor for submucosal invasion of gastric cancers
2021-09-18OsamuToyoshimaShuntaroYoshidaToshihiroNishizawaAkiraToyoshimaKosukeSakitaniTatsuyaMatsunoTomoharuYamadaTakashiMatsuoHayatoNakagawaKazuhikoKoike
Osamu Toyoshima,Shuntaro Yoshida,Toshihiro Nishizawa,Akira Toyoshima,Kosuke Sakitani,Tatsuya Matsuno,Tomoharu Yamada,Takashi Matsuo,Hayato Nakagawa,Kazuhiko Koike
Osamu Toyoshima,Shuntaro Yoshida,Toshihiro Nishizawa,Kosuke Sakitani,Tatsuya Matsuno,Tomoharu Yamada,Department of Gastroenterology,Toyoshima Endoscopy Clinic,Setagayaku 157-0066,Tokyo,Japan
Toshihiro Nishizawa,Department of Gastroenterology and Hepatology,International University of Health and Welfare,Narita Hospital,Narita 286-8520,Chiba,Japan
Akira Toyoshima,Department of Colorectal Surgery,Japanese Red Cross Medical Center,Shibuya-ku 150-8935,Tokyo,Japan
Kosuke Sakitani,Department of Gastroenterology,Sakitani Endoscopy Clinic,Narashino 275-0026,Chiba,Japan
Tatsuya Matsuno,Tomoharu Yamada,Hayato Nakagawa,Kazuhiko Koike,Department of Gastroenterology,Graduate School of Medicine,The University of Tokyo,Bunkyo-ku 113-8655,Tokyo,Japan
Takashi Matsuo,Department of Internal Medicine,Sakura Internal Medicine Clinic,Setagayaku 157-0071,Tokyo,Japan
Abstract BACKGROUND Accurate diagnosis of the depth of gastric cancer invasion is crucial in clinical practice.The diagnosis of gastric cancer depth is often made using endoscopic characteristics of the tumor and its margins;however,evaluating invasion depth based on endoscopic background gastritis remains unclear.AIM To investigate predicting submucosal invasion using the endoscopy-based Kyoto classification of gastritis.METHODS Patients with gastric cancer detected on esophagogastroduodenoscopy at Toyoshima Endoscopy Clinic were enrolled.We analyzed the effects of patient and tumor characteristics,including age,sex,body mass index,surveillance endoscopy within 2 years,current Helicobacter pylori infection,the Kyoto classification,and Lauren’s tumor type,on submucosal tumor invasion and curative endoscopic resection.The Kyoto classification included atrophy,intestinal metaplasia,enlarged folds,nodularity,and diffuse redness.Atrophy was characterized by non-reddish and low mucosa.Intestinal metaplasia was detected as patchy whitish or grayish-white flat elevations,forming an irregular uneven surface.An enlarged fold referred to a fold width ≥ 5 mm in the greater curvature of the corpus.Nodularity was characterized by goosebump-like multiple nodules in the antrum.Diffuse redness was characterized by uniform reddish nonatrophic mucosa in the greater curvature of the corpus.RESULTS A total of 266 gastric cancer patients (mean age,66.7 years;male sex,58.6%;mean body mass index,22.8 kg/m2) were enrolled.Ninety-three patients underwent esophagogastroduodenoscopy for surveillance within 2 years,and 140 had current Helicobacter pylori infection.The mean Kyoto score was 4.54.Fifty-eight cancers were diffuse-type,and 87 cancers had invaded the submucosa.Multivariate analysis revealed that low body mass index (odds ratio 0.88,P=0.02),no surveillance esophagogastroduodenoscopy within 2 years (odds ratio 0.15,P <0.001),endoscopic enlarged folds of gastritis (odds ratio 3.39,P=0.001),and Lauren’s diffuse-type (odds ratio 5.09,P <0.001) were independently associated with submucosal invasion.Similar results were obtained with curative endoscopic resection.Among cancer patients with enlarged folds,severely enlarged folds (width ≥ 10 mm) were more related to submucosal invasion than mildly enlarged folds (width 5-9 mm,P <0.001).CONCLUSION Enlarged folds of gastritis were associated with submucosal invasion.Endoscopic observation of background gastritis as well as the lesion itself may help diagnose the depth of cancer invasion.
Key Words:Gastric cancer;Gastritis;Enlarged fold;Endoscopy;Kyoto classification
INTRODUCTION
Gastric cancer is the third most common cause of cancer mortality worldwide,making it an important disease[1,2].The depth of gastric cancer invasion is associated with lymph node metastasis[3,4],recurrence[5],and survival[6,7] and has a great influence on therapeutic strategy[8-10].This means that the diagnosis of invasion depth is crucial.
At present,the diagnosis of gastric cancer depth is often made using the endoscopic characteristics of the tumor and its margins.For example,an irregular surface,marked marginal elevation,and clubbing/abrupt cutting/fusion of converting folds are useful for the diagnosis of submucosal invasion[11].Similarly,using nodular mucosal changes,deep depression,and fold convergence for the diagnosis of signet ring cell carcinoma with submucosal invasion[12],and the non-extension sign[13],size >30 mm,margin elevation,uneven surface[14],remarkable redness[14,15],and abrupt cutting converging folds[15] for the diagnosis of deeper submucosal invasion (SM2:≥500 µm in depth) have also been reported.For the last decade,the depth of gastric cancer has been predicted using magnifying narrow-band imaging,which is an imageenhanced endoscopy,in addition to conventional white-light imaging[16].Findings such as non-structure,scattering,or multi-caliber vessels[17],D-vessels[18],and the vessel plus surface classification[19] were found to be useful for depth diagnosis.Furthermore,various modalities,including endoscopic ultrasonography[20] and computed tomography[21],have been found to assist in depth diagnosis.Thus,research on the depth of invasion is being vigorously conducted.
On the other hand,artificial intelligence is now overwhelming human intelligence.Artificial intelligence defeated the world champion in chess in 1997 and in the East Asian game of go in 2017.The style of play used by artificial intelligence was of a different dimension unimaginable to humans.Recently,artificial intelligence has been used for endoscopic diagnosis[22].In the future,artificial intelligence may be used to diagnose the depth of invasion based not only on the tumor itself but also on background gastritis.However,there are few reports on the evaluation of invasion depth based on endoscopic background gastritis.Therefore,we decided to investigate predictions for submucosal invasion using the endoscopy-based Kyoto classification of gastritis,for which evidence has been accumulated recently[23-25].
MATERIALS AND METHODS
Patients and overview
This study involved those patients who underwent esophagogastroduodenoscopy(EGD) between January 2008 and August 2020 at Toyoshima Endoscopy Clinic,in whom gastric cancers were detected.Exclusion criteria were cancer located in the esophagogastric junction or in the residual stomach after surgery,or unavailable EGD images.We also excluded patients with unavailableHelicobacter pylori(H.pylori) status.In this study,curative endoscopic resection of gastric cancer was performed according to the guidelines of the Japanese Gastric Cancer Association[26].
This retrospective study was approved by the Certificated Review Board,Hattori Clinic on September 4,2020 (approval No.S2009-U04).Written informed consent was obtained from all participants.All clinical evaluations were conducted in accordance with the ethical guidelines of the Declaration of Helsinki.This study had no financial support.
Endoscopy
The Japan Gastroenterological Endoscopy Society advocated the endoscopy-based Kyoto classification of gastritis in 2013 with the aim of matching endoscopic findings and pathology.The Kyoto classification of gastritis comprises atrophy,intestinal metaplasia,enlarged folds,nodularity,and diffuse redness.Endoscopic atrophy is characterized by non-reddish and low mucosa,identified by an atrophic border,according to the Kimura-Takemoto classification[27].Endoscopic intestinal metaplasia is detected as patchy whitish or grayish-white flat elevations,forming an irregular uneven surface[28].An enlarged fold refers to a fold with width ≥ 5 mm in the greater curvature of the corpus,which is not flattened or only partially flattened by stomach insufflation.Endoscopic nodularity is characterized by goosebump-like multiple nodules that appear mainly in the antrum and represent a collection of lymphoid follicles.Diffuse redness is characterized by uniform reddish non-atrophic mucosa located mainly in the greater curvature of the corpus and representing superficial gastritis.
The Kyoto score is the sum of the following five parameters:atrophy,intestinal metaplasia,enlarged folds,nodularity,and diffuse redness score and ranges from 0 to 8.Kimura-Takemoto classification gradings of C0 and CI are defined as an atrophy score of 0,CII and CIII have an atrophy score of 1,and OI to OIII have an atrophy score of 2.Absence of intestinal metaplasia was defined as an intestinal metaplasia score of 0,intestinal metaplasia limited to the antrum was given 1,and intestinal metaplasia extending into the corpus received an intestinal metaplasia score of 2.The absence and presence of enlarged folds were defined as enlarged fold scores of 0 and 1,respectively.The absence and presence of nodularity were defined as nodularity scores of 0 and 1,respectively.Diffuse redness scores were defined as 0,1,and 2 for no diffuse redness,mild redness,and severe redness,respectively.The Kyoto score has been proven to be associated with the presence of gastric cancer[23],the risk of gastric cancer[25],andH.pyloriinfection[24].
In this study,enlarged folds were divided into two groups:severely enlarged folds with widths ≥ 10 mm and mildly enlarged folds with widths of 5-9 mm[29,30].Fold width was measured by placing a closed or opened forceps,which has a width of 2 mm or 7mm,against enlarged folds.
One expert endoscopist retrospectively reviewed the EGD images and evaluated the Kyoto score.Surveillance EGD was defined as such only if the patients had undergone a previous EGD at our institution within the last 2 years[31].
Pathology
The depth of the tumor was diagnosed using the resected specimen or if unresectable,from computed tomography images.Tumor type was evaluated according to the Lauren classification (diffuse- or intestinal-type)[32].
H.pylori status
We divided theH.pyloriinfection status into two groups:current infection and negative for current infection.The current infection group included patients in whomH.pylorieradication therapy had failed.The group of negative for current infection includedH.pylori-uninfected patients andH.pylori-past infected patients who had undergone successful eradication therapy or in whomH.pylorihad spontaneously disappeared[33].
Data collection and outcomes
The T-File System (STS-Medic Inc.,Tokyo,Japan) was used to file the endoscopic images and for documentation of the endoscopic findings.We collected data on age,sex,interval from previous EGD,and endoscopic images from the T-File System,and data on body mass index (BMI),H.pyloristatus,treatment for the cancer,and Lauren type of the tumor from electronic medical records.
Statistical analysis
Univariate and multivariate analyses for the effect on submucosal invasion and curative endoscopic resection were performed using a binomial logistic regression model.Variables with aPvalue <0.1 in the univariate analysis were entered into the multivariate analysis and calculated using the all-possible-regressions procedure.We used a complete analysis for missing data.We evaluated the frequency of submucosal invasion among patients with negatively enlarged folds and mildly and severely enlarged folds using the Cochran-Armitage trend test.
Statistical significance was indicated by aPvalue of <0.05.Calculations were performed using the statistical software Ekuseru-Toukei 2015 (Social Survey Research Information Co.,Ltd.,Tokyo,Japan).
RESULTS
Patient enrollment
A total of 300 patients with gastric adenocarcinomas were observed at the Toyoshima Endoscopy Clinic during the study period.We excluded nine cancers located at the esophagogastric junction,seven cancers located in the residual stomach after surgery,nine cancers with unavailable EGD images,and nine cancers with unavailableH.pyloristatus.Finally,266 gastric cancers were enrolled.Figure 1 presents the patient flowchart of this study.
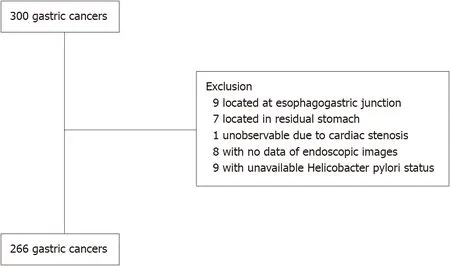
Figure 1 Patient flowchart.
Patient characteristics
Table 1 shows the patient characteristics of the study.The mean age was 66.7 (range,37-89) years.Of the patients,58.6% were male.The mean BMI was 22.8 kg/m2.Ninetythree patients (35.0%) underwent EGD for surveillance within 2 years.CurrentH.pyloriinfection was identified in 52.6% (including 129 patients without past eradication therapy and 11 patients with failed eradication therapy) of the study patients.Cases negative for currentH.pyloriinfection included 13 uninfected and 113 past-infected patients.The mean Kyoto score was 4.54 (atrophy score,1.75;intestinal metaplasia,1.32;enlarged folds,0.24;nodularity,0.08;diffuse redness score,1.15).The proportion of diffuse-type adenocarcinoma on the Lauren classification was 21.8%.With respect to the depth of gastric cancer,179 (67.3%) were in the mucosa,51 (19.2%) were in the submucosa,and 36 (13.5%) were in the muscularis propria or deeper.
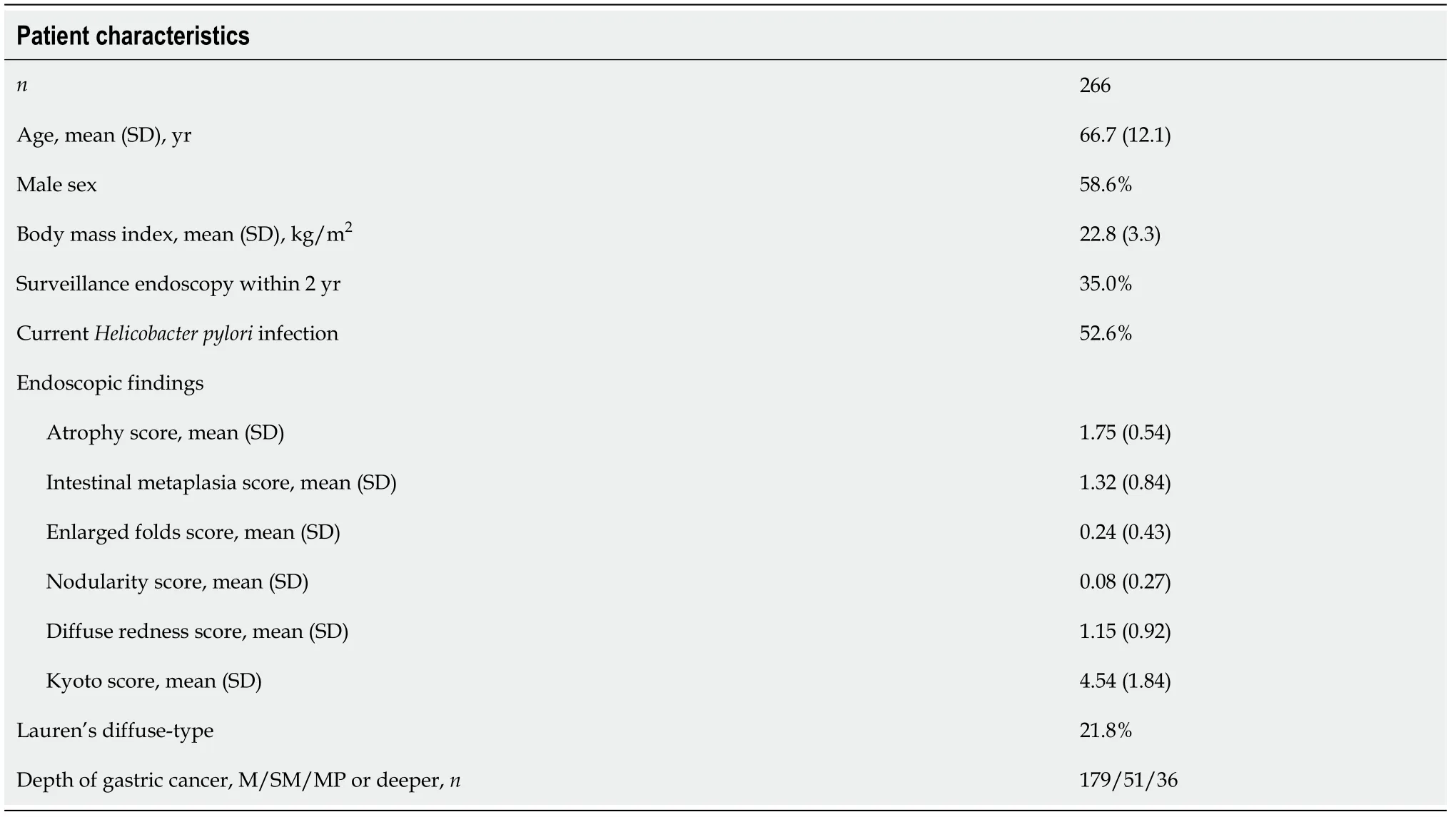
Table 1 Patient characteristics of this study
Effects on submucosal invasion of gastric cancer
We analyzed the effects on submucosal invasion of gastric cancer using univariate and multivariate analyses (Table 2).Multivariate analysis showed that low BMI (odds ratio 0.88,P=0.02),non-surveillance EGD (odds ratio 0.15,P<0.001),enlarged folds (odds ratio 3.39,P=0.001),and Lauren’s diffuse-type adenocarcinoma (odds ratio 5.09,P<0.001) were associated with submucosal invasion.
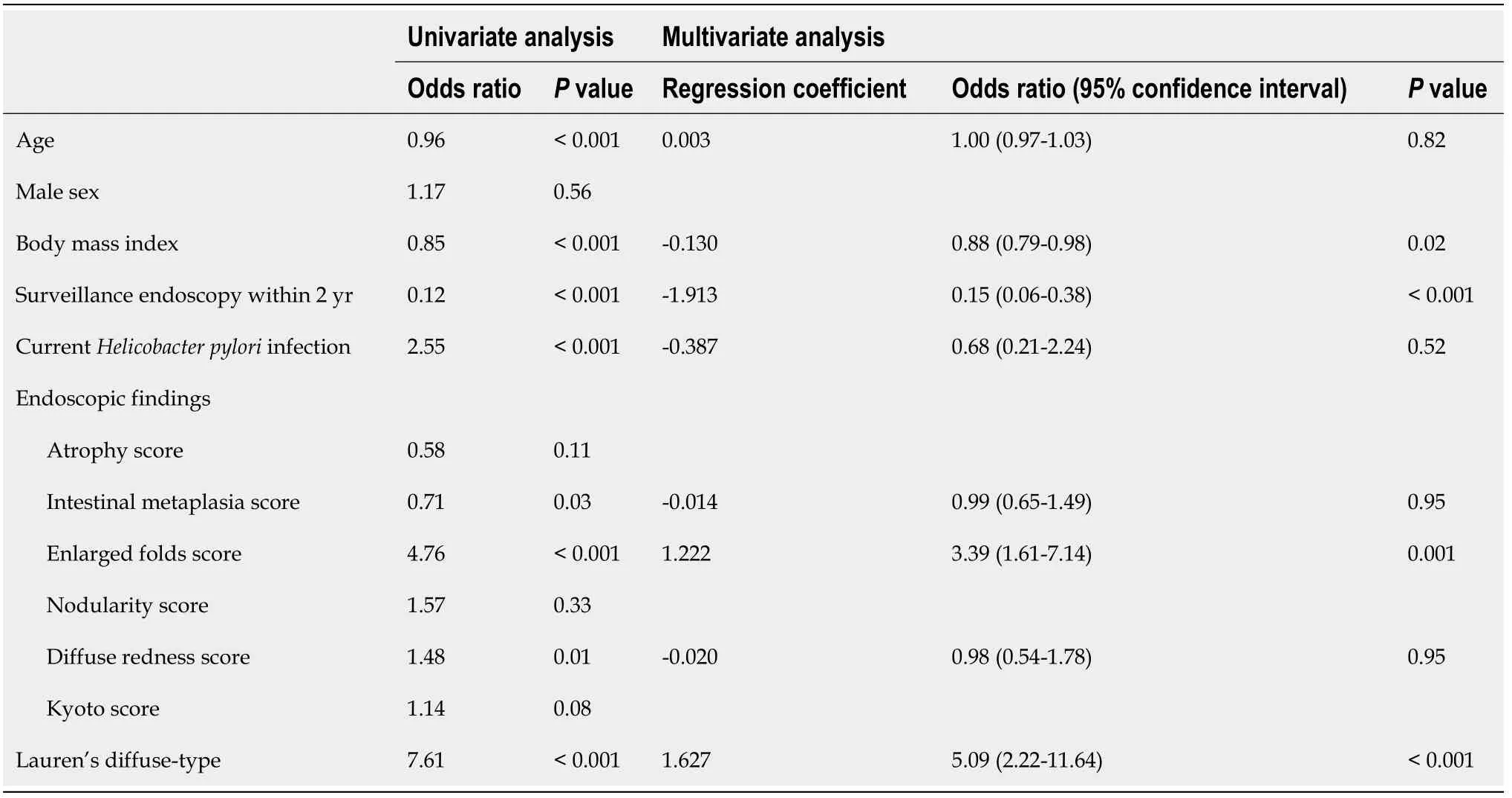
Table 2 Effect on submucosal invasion of gastric cancer
Next,we analyzed the effects on patients who underwent curative treatment with endoscopic resection without surgery.In addition to the mucosal depth of gastric cancer,patients who underwent curative endoscopic resection were associated with high BMI,surveillance EGD,no enlarged folds,and Lauren’s intestinal-type adenocarcinoma (Supplementary Table 1).
Sub-analysis of patients with enlarged folds
We divided gastric cancer patients with enlarged folds into two categories:mildly and severely enlarged folds.Submucosal invasion was observed in 49 of 203 cancers without enlarged folds,14 of 30 cancers with mildly enlarged folds,and 24 of 33 cancers with severely enlarged folds.Figure 2 shows the proportions of submucosal invasion based on the severity of the enlarged folds.The severity of the enlarged folds was related to the depth of the tumor (P<0.001,Cochran-Armitage trend test).
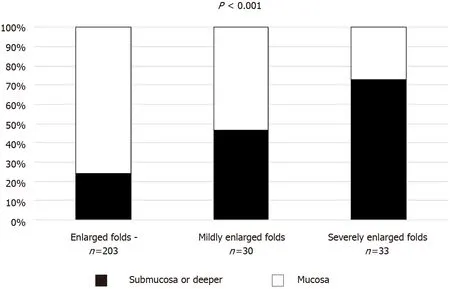
Figure 2 Proportion of submucosal invasion based on severity of enlarged folds.
Representative images of enlarged fold gastritis and coexisting gastric cancer are shown in Figure 3.
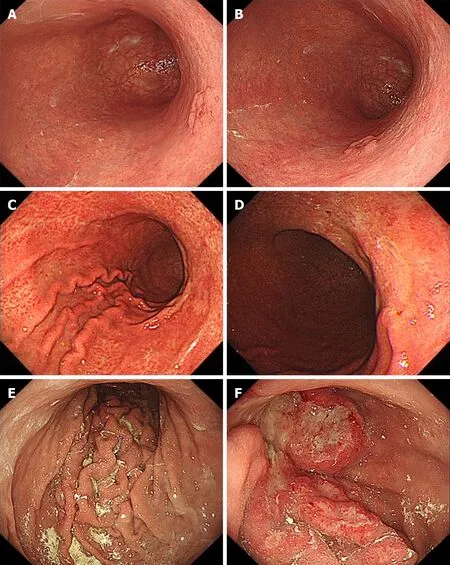
Figure 3 Representative images of enlarged folds and coexisting gastric cancer.
DISCUSSION
In this study,we found that the enlarged folds of background gastritis were related to submucosal invasion of gastric cancer.Furthermore,the severity of the enlarged folds was associated with the depth of the tumor.We showed that cancer invasion may be predicted based on background gastritis.The strength of this study is that background gastritis,under the new criterion of the Kyoto classification,is related to the depth of invasion and not limited to observation of the lesions themselves.However,comprehensive endoscopic diagnosis is required in clinical practice because of advances in technology such as artificial intelligence.
Enlarged folds have been well studied for their bi ological characteristics.Enlarged folds have been shown to be associated with the tumor necrosis factor-alpha gene polymorphism as a genetic predisposition[34].Genome wide hypomethylation and regional hypermethylation have been shown to occur in enlarged folds[35,36].The production of interleukin 1 beta and hepatocyte growth factor caused byH.pyloriinfection reportedly contributes to fold enlargement in the stomach by stimulating epithelial cell proliferation and inhibiting acid secretion[37,38].Morphological changes in parietal cells associated withH.pyloriinfection have been reported to be functionally related to the inhibition of acid secretion seen in patients with enlarged folds[39].In addition,enlarged folds are strongly associated withH.pyloriinfection and have been shown to improve with eradication[24,29,34].Enlarged folds are considered to be at high risk of gastric cancer,especially diffuse cancer,which is closely related to highly active inflammation[36,40].These biological behaviors of the enlarged folds may be attributed to the depth of the cancer.
Yasunagaet al[29] divided enlarged folds into two categories (severe and mild) and found that severely enlarged folds suppressed acid secretion and had higher serum gastrin,pepsinogen I,and pepsinogen II levels compared to mildly enlarged folds[30].Such differences may contribute to active inflammation of the mucosa and depth of cancer.
Invasion depth has already been reported to be associated with Lauren’s histological type[41],surveillance endoscopy[31],and BMI[42].Consistent with these previous reports,the multivariate analysis of the present study demonstrated that submucosal invasion was associated with pathology,surveillance,and BMI.
This study has some limitations.First,this was a single-institute retrospective study.However,the quality of the data was well-controlled.In the future,a prospective,multicenter design is needed.Second,because the number of events was small,the variables that could be entered into multivariate analysis were limited.It is desirable to increase the number of events and investigate factors such as family history,drinking and smoking history,and aspirin use.Third,we did not endoscopically evaluate the tumor itself.Comprehensive analyses of the tumor itself and background gastritis are warranted.
CONCLUSION
Endoscopy-based enlarged folds of gastritis were associated with submucosal invasion of the tumor.Endoscopic observation of background gastritis as well as the lesion itself may help diagnose the depth of cancer invasion in clinical practice.Therefore,further comprehensive investigations are required.
ARTICLE HIGHLIGHTS
Research background
The diagnosis of gastric cancer depth is often made using endoscopic characteristics of the tumor and its margins.
Research motivation
In the future,artificial intelligence may be used to diagnose the depth of invasion based not only on the tumor itself but also on background gastritis.
Research objectives
We investigated predicting submucosal invasion based on endoscopic background gastritis.
Research methods
Patients with gastric cancer detected on esophagogastroduodenoscopy were enrolled.We analyzed the effects of patient and tumor characteristics including the Kyoto classification.
Research results
Endoscopic enlarged folds of gastritis (odds ratio 3.39,P=0.001) was independently associated with submucosal invasion.Among cancer patients with enlarged folds,severely enlarged folds (width ≥ 10 mm) were more related to submucosal invasion than mildly enlarged folds (width 5-9 mm,P<0.001).
Research conclusions
Enlarged folds of gastritis were associated with submucosal invasion.
Research perspectives
Endoscopic observation of background gastritis as well as the lesion itself may help diagnose the depth of cancer invasion.
杂志排行
World Journal of Gastrointestinal Endoscopy的其它文章
- Ectopic pancreas at the ampulla of Vater diagnosed with endoscopic snare papillectomy:A case report and review of literature
- Endoscopic treatment of periampullary duodenal duplication cysts in children:Case series and literature review
- COVID-19 in the endoscopy unit:How likely is transmission of infection? Results from an international,multicenter study
- Clinical characteristics and prognosis of patients with ulcerative colitis that shows rectal sparing at initial diagnosis
- Gastrointestinal hemorrhage in the setting of gastrointestinal cancer:Anatomical prevalence,predictors,and interventions
- Endoscopic balloon dilation for management of stricturing Crohn’s disease in children