Genitourinary function and defecation after colorectal cancer surgery with low- and high-ligation of the inferior mesenteric artery:A meta-analysis
2021-09-03XiaoBaiChunDongZhangJunPengPeiDongQiuDai
Xiao Bai, Chun-Dong Zhang, Jun-Peng Pei, Dong-Qiu Dai
Xiao Bai, Chun-Dong Zhang, Jun-Peng Pei, Dong-Qiu Dai, Department of Gastrointestinal Surgery, the Fourth Affiliated Hospital of China Medical University, Shenyang 110032,Liaoning Province, China
Chun-Dong Zhang, Department of Gastrointestinal Surgery, Graduate School of Medicine, The University of Tokyo, Tokyo 113-0033, Japan
Dong-Qiu Dai, Cancer Center, the Fourth Affiliated Hospital of China Medical University,Shenyang 110032, Liaoning Province , China
Abstract BACKGROUND The effect of low ligation (LL) vs high ligation (HL) of the inferior mesenteric artery (IMA) on functional outcomes during sigmoid colon and rectal cancer surgery, including urinary, sexual, and bowel function, is still controversial.AIM To assess the effect of LL of the IMA on genitourinary function and defecation after colorectal cancer (CRC) surgery.METHODS EMBASE, PubMed, Web of Science, and the Cochrane Library were systematically searched to retrieve studies describing sigmoid colon and rectal cancer surgery in order to compare outcomes following LL and HL. A total of 14 articles, including 4750 patients, were analyzed using Review Manager 5.3 software. Dichotomous results are expressed as odds ratios (ORs) with 95% confidence intervals (CIs) and continuous outcomes are expressed as weighted mean differences (WMDs) with 95%CIs.RESULTS LL resulted in a significantly lower incidence of nocturnal bowel movement (OR =0.73, 95%CI: 0.55 to 0.97, P = 0.03) and anastomotic stenosis (OR = 0.31, 95%CI:0.16 to 0.62, P = 0.0009) compared with HL. The risk of postoperative urinary dysfunction, however, did not differ significantly between the two techniques.The meta-analysis also showed no significant differences between LL and HL in terms of anastomotic leakage, postoperative complications, total lymph nodes harvested, blood loss, operation time, tumor recurrence, mortality, 5-year overall survival rate, or 5-year disease-free survival rate.CONCLUSION Since LL may result in better bowel function and a reduced rate of anastomotic stenosis following CRC surgeries, we suggest that LL be preferred over HL.
Key Words: Low ligation; High ligation; Colorectal cancer; Genitourinary function;Defecatory function; Meta-analysis
INTRODUCTION
Colorectal cancer (CRC) ranks third in global cancer incidence, accounting for 10.0% of the total number of cancer cases, and ranks second in mortality[1]. Two techniques,which differ mainly in the level of inferior mesenteric artery (IMA) ligation, are used during curative surgery for cancer of the sigmoid colon and rectum. Which of high ligation (HL), which does not preserve the left colic artery, or low ligation (LL), which does preserve the left colic artery, is the better technique has been controversial since 1908[2]. Compared with LL, HL may allow a greater total number of lymph nodes to be harvested, facilitating more accurate assessment of tumor stage, and guiding adjuvant treatment. HL may be easier to achieve surgically and has been advocated by Girardet al[3]. Because HL will increase urogenital and defecation disorders, others have recently suggested that LL be preferred[4,5]. Some studies, however, showed no significance between LL and HL in terms of surgical or oncological outcomes[6,7].
Because of the ongoing controversy, previous reviews have explored the relationship between the two different approaches to IMA ligation and patient outcomes. Harjinderet al[8] found no difference between the two techniques in terms of rate of anastomotic leakage, total number of lymph nodes harvested, or survival rates. Other meta-analyses[9,10], however, found that LL of the IMA is associated with a lower risk of anastomotic leakage. At present, when completing sigmoid colon and rectal cancer surgery, it remains unclear whether the benefits of LL extend to improved genitourinary and defecatory function.
To address this, we carried out this meta-analysis to systemically compare LL and HL of the IMA in terms of functional outcomes, including urinary, sexual, and bowel function, as well as other surgical and survival outcomes.
MATERIALS AND METHODS
Search strategy
This meta-analysis was conducted according to the guidelines for Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA)[11]. The search terms“ligation” and “colorectal surgery” were used to retrieve all relevant articles from the Cochrane library, PubMed, EMBASE, and Web of Science (search last updated in December, 2020). References cited by articles identified in the initial search were used to identify additional relevant articles.
Primary outcomes
Genitourinary functional outcomes, including sexual function, urinary function, and defecation, were regarded as primary outcomes.
Secondary outcomes
The secondary outcomes were total number of lymph nodes harvested, anastomotic stenosis, anastomotic leakage, postoperative complications, operation time, blood loss,mortality, recurrence, 5-year overall survival, and disease-free survival.
Study selection and data extraction
The following criteria were used for inclusion: (1) Studies having at least one main result; (2) Randomized controlled trials (RCTs) or non-randomized studies in patients with sigmoid colon and rectal cancer; and (3) Studies comparing high and low ligation in radical resection, regardless of surgical approach. Where several reports described the same clinical study, the publication with the most complete data set was included in the meta-analysis. Articles in any language were included.
The exclusion criteria were as follows: (1) Studies having no control group; (2) Full text unavailable; and (3) Review articles, case reports, letters, or meta-analyses.
Two authors independently checked and evaluated the titles and/or abstracts of the articles and excluded any that were obviously irrelevant. The suitability of the remaining articles for inclusion in the analysis was assessed by inspection of the full article. Relevant details on research design, baseline characteristics, and outcomes were then collected. Differences in opinion between the two authors were resolved through discussion. The following data were retrieved from each article: Year of publication, first author’s name, country where the study was conducted, and the number of patients, together with age and gender. If available, supplementary information was obtained for each article included in the study.
Quality assessment
The Newcastle-Ottawa Scale[12], based on comparability between groups, quality of patient selection, patient results, and determination of exposure, was used to evaluate the quality of non-randomized studies. The Cochrane Collaborative Bias Risk Tool was used to evaluate the quality of RCTs. Research areas covered allocation concealment,selective reporting of results, sequence generation, incomplete results, blinding, and other sources of bias. The bias risk of each study was sorted as high, ambiguous, or low. Differences were settled through consensus discussions.
Statistical analysis
Statistical analyses were performed using Review Manager 5.3 software (The Cochrane Collaboration; Copenhagen, Denmark). Continuous outcomes are expressed as weighted mean differences (WMDs), with 95% confidence intervals (CIs). Dichotomous outcomes are expressed as odds ratios (ORs), with 95%CIs. Heterogeneity between studies was evaluated using theχ2test (CochranQtest) andI2statistics. The random effects model was used for meta-analysis where thePvalue was less than 0.10 orI2was greater than 50%; otherwise the fixed effects model was used.
RESULTS
Study selection
Our initial search identified 458 studies. After removal of duplicates and assessment of eligibility for inclusion, 14 clinical trials, which included an LL treatment group and an HL treatment group, were included in the final analysis (Figure 1). These studies involved a total of 4750 patients, with 1984 patients in the LL group and 2766 patients in the HL group. The baseline characteristics of the 14 eligible studies[4,5,7,13-23] are shown in Table 1. Quality assessments of the included studies are shown in Table 2 and Figure 2, and all endpoints are listed in Table 3.
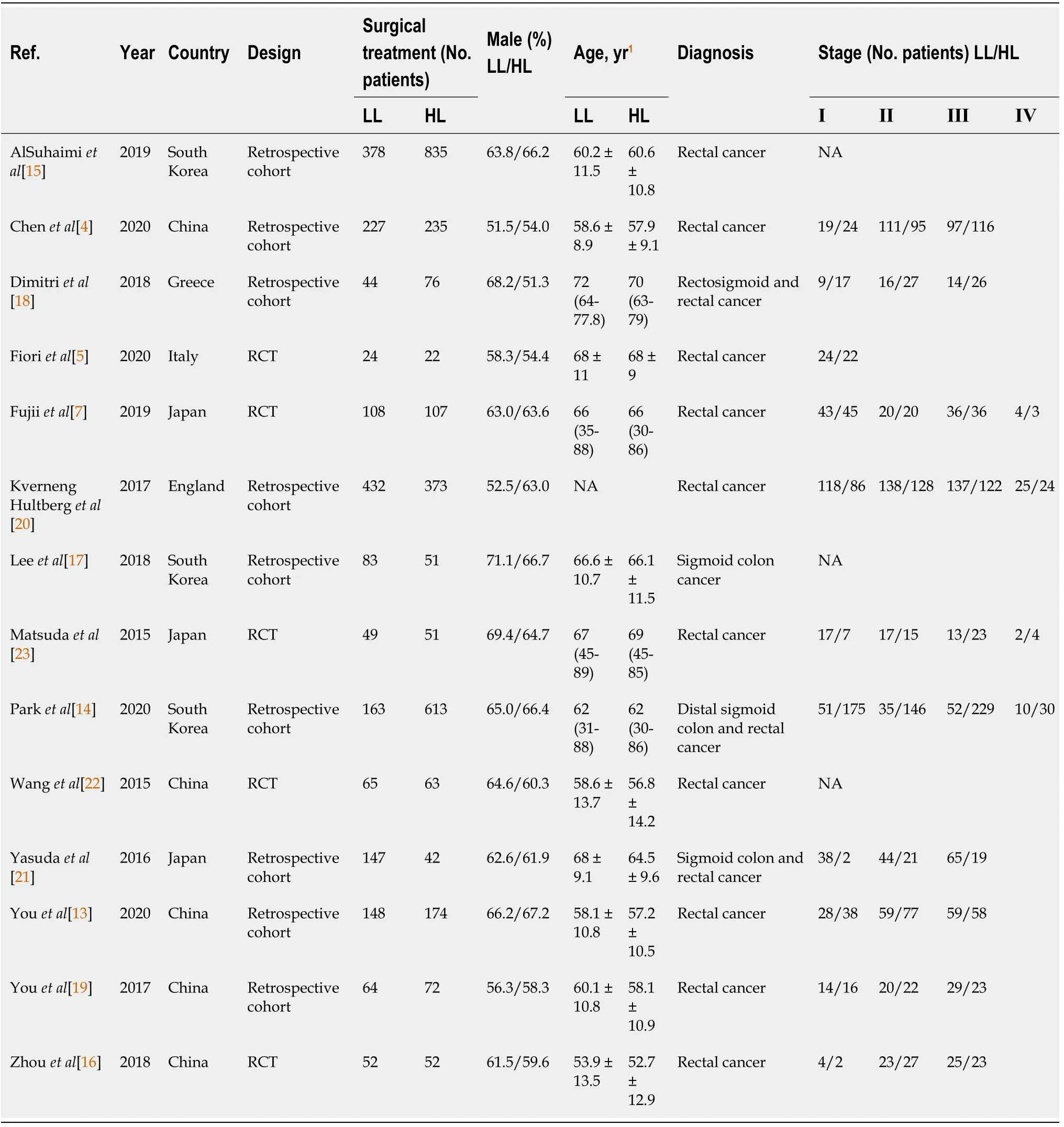
Table 1 Characteristics of studies included
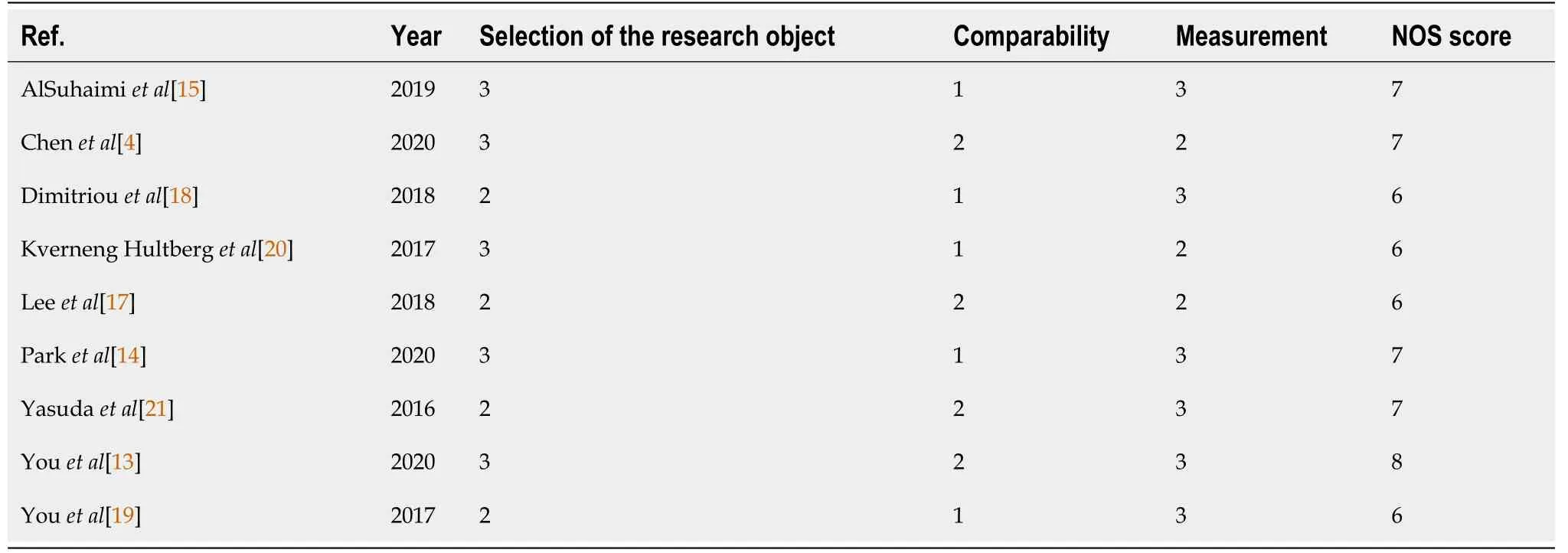
Table 2 Quality assessment of included non-randomized trials based on Newcastle-Ottawa scoring system
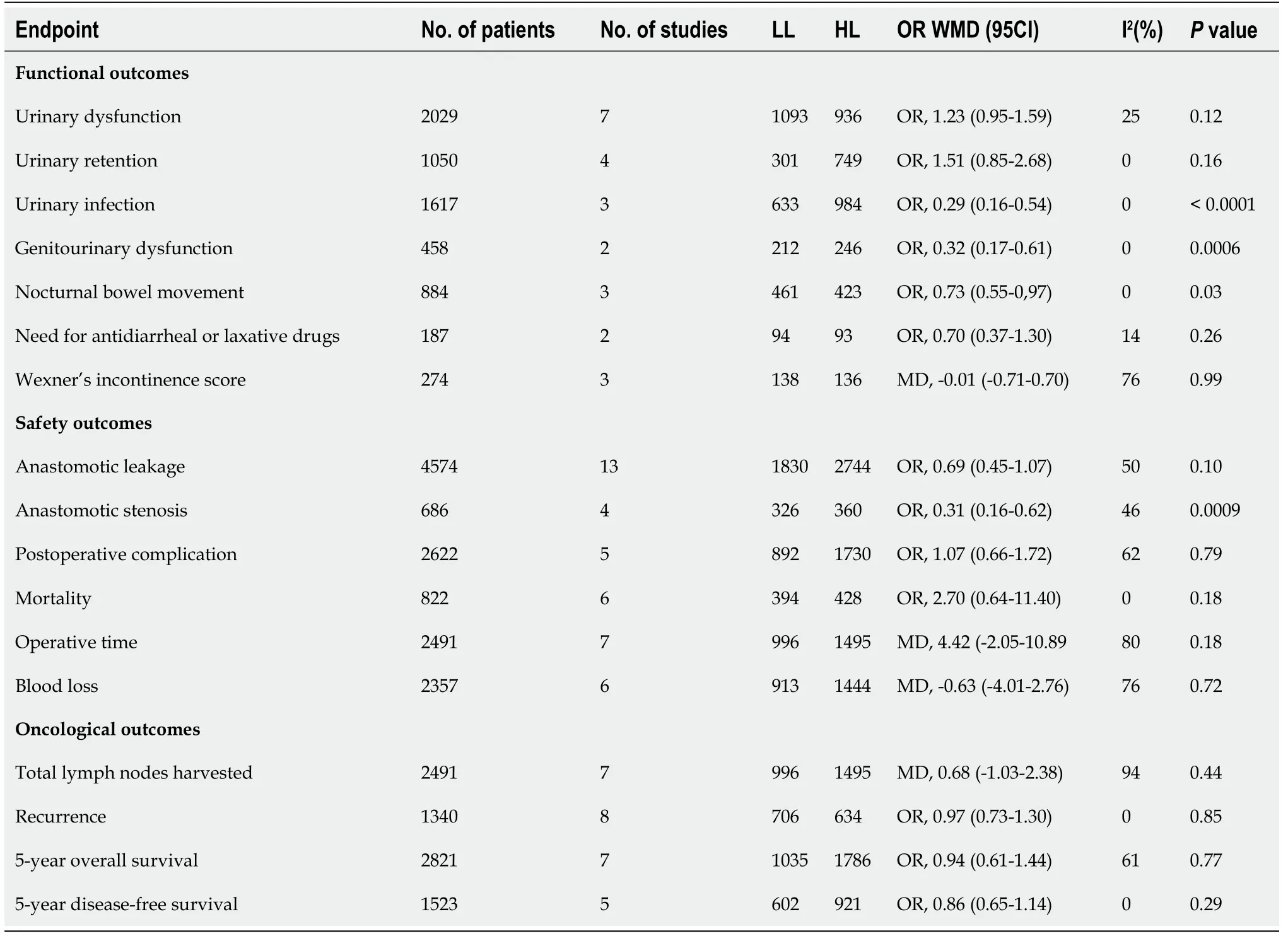
Table 3 Endpoints of this meta-analysis
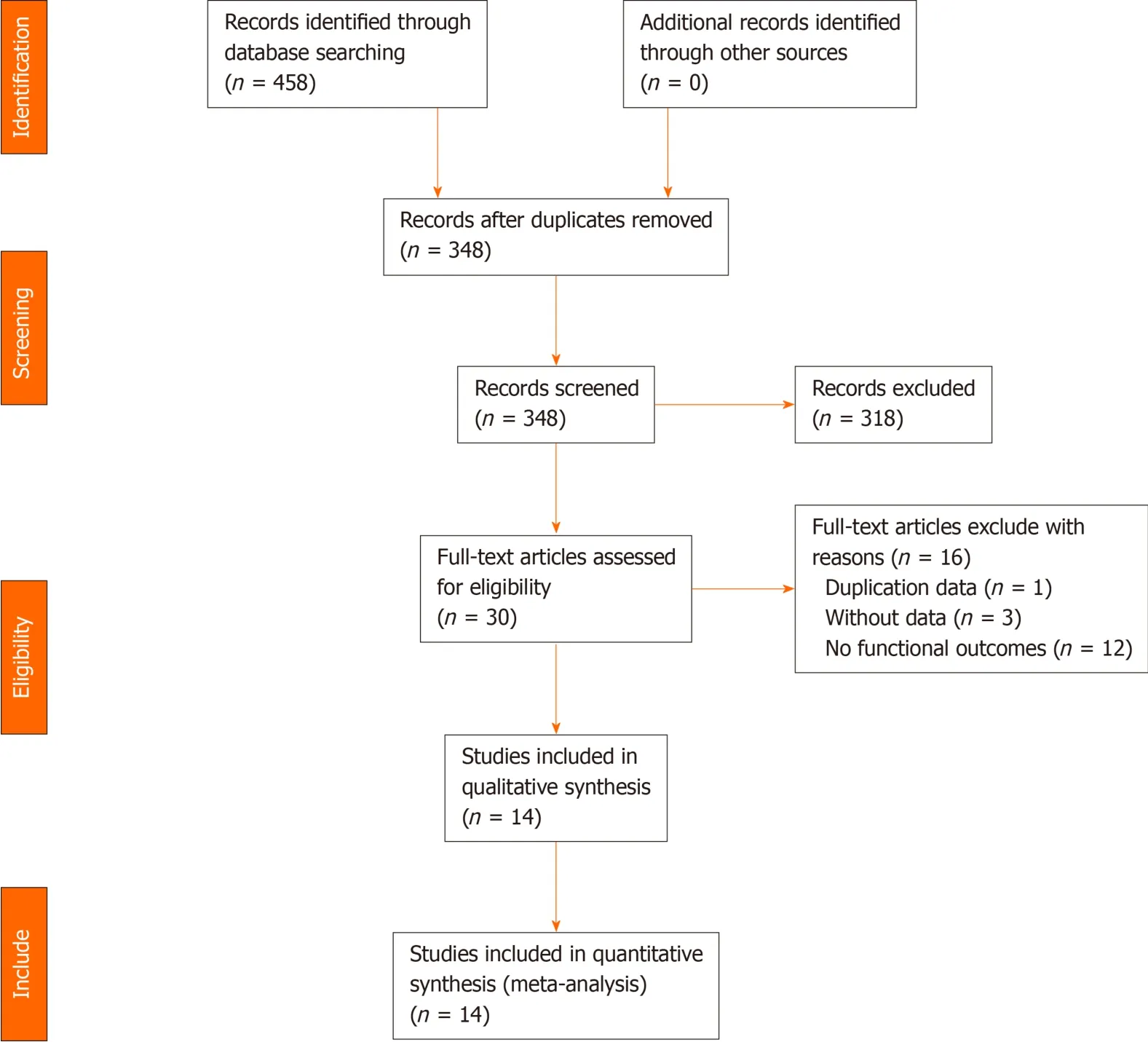
Figure 1 Flow diagram of literature search.
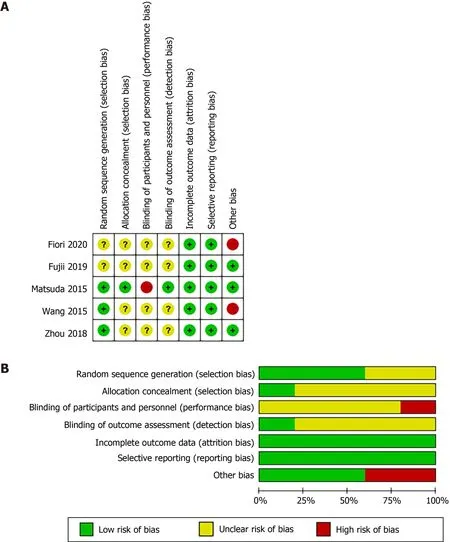
Figure 2 Summary of methodologic quality assessment. A: Risk of bias summary; B: Risk of bias graph.
Genitourinary function outcomes
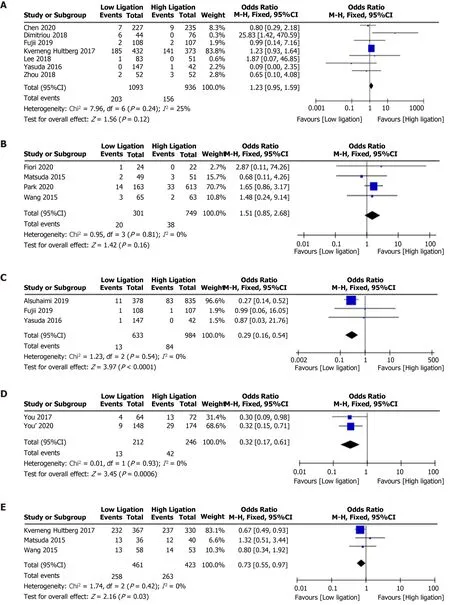
No significant differences in urinary dysfunction (OR = 1.23, 95%CI: 0.95 to 1.59,P=0.12; Figure 3A)[4,7,16-18,20,21] or urinary retention (OR = 1.51, 95%CI: 0.85 to 2.68,P= 0.16; Figure 3B)[5,14,22,23] were found between the LL and HL groups. The LL group did, however, have a lower risk of urinary infection (OR = 0.29, 95%CI: 0.16 to 0.54,P< 0.0001; 3C)[7,15,21] and a decreased risk of genitourinary dysfunction (OR =0.32, 95%CI: 0.17 to 0.61,P= 0.0006; Figure 3D), compared with the HL group[13,19].
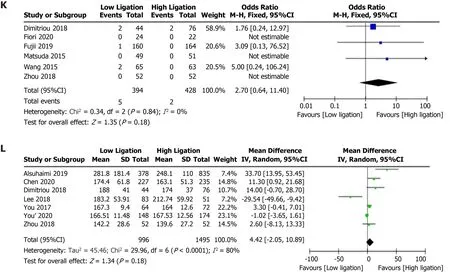
Figure 3 Forest plots for various function parameters with low ligation and high ligation. A: Urinary dysfunction; B: Urinary retention; C: Urinary infection; D: Genitourinary dysfunction; E: Nocturnal bowel movement; F: Need for antidiarrheal or laxative drugs; G: Wexner’s incontinence score; H: Anastomotic stenosis; I: Anastomotic leakage; J: Postoperative complications; K: Mortality; L: Operative time.
Defecatory function outcomes
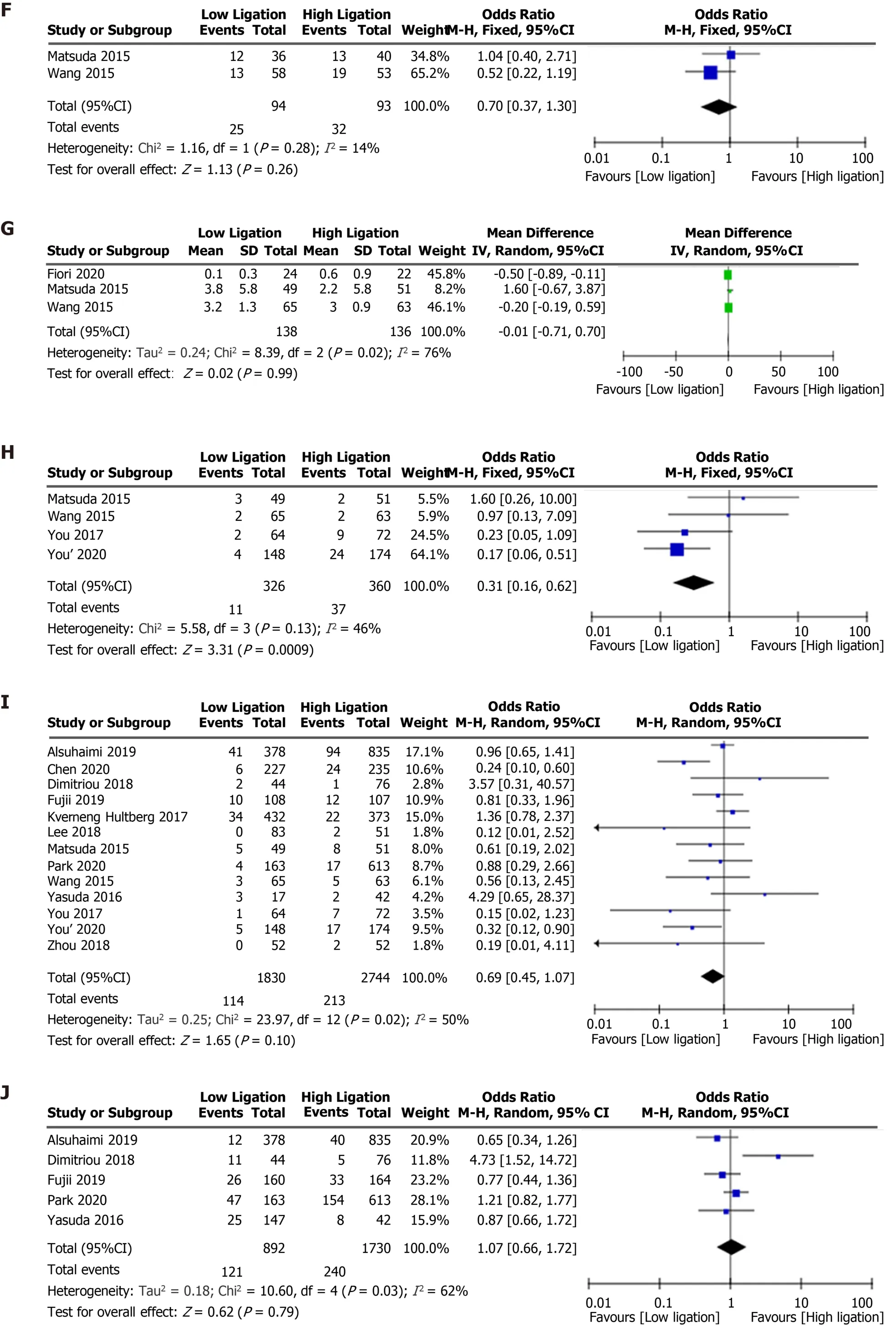
Nocturnal bowel movement was lower in the LL group than in the HL group (OR =0.73, 95%CI: 0.55 to 0.97,P= 0.03; Figure 3E)[20,22,23], but there was no difference between the two groups in terms of need for antidiarrheal or laxative drugs (OR =0.70, 95%CI: 0.37 to 1.30,P= 0.26; Figure 3F)[22,23] or Wexner’s incontinence score(WMD, -0.01, 95%CI: -0.71 to 0.70,P= 0.99; Figure 3G)[5,22,23].
Safety outcomes
Although the LL group had a lower incidence of anastomotic stenosis than the HL group (OR = 0.31, 95%CI: 0.16 to 0.62,P= 0.0009; Figure 3H)[13,19,22,23], there were no significant differences in the anastomotic leakage rate (OR = 0.69, 95%CI: 0.45 to 1.07,P= 0.10; Figure 3I)[4,7,13-23], postoperative complication rate (OR = 1.07, 95%CI:0.66 to 1.72,P= 0.79; Figure 3J)[7,14,15,18,21], or mortality (OR = 2.70, 95%CI: 0.64 to 11.40,P= 0.18; Figure 3K)[5,7,16,18,22,23] between the two groups. There were no differences in operative time (WMD, 4.42, 95%CI: -2.05 to 10.89,P= 0.18; Figure 3L)[4,13,15-19] or blood loss (WMD, -0.63, 95%CI: -4.01 to 2.76,P= 0.72; Figure 4A)[4,13,15,16,18,19] between the two groups.
Oncological outcomes
There were no differences in the total number of lymph nodes harvested (WMD, 0.68,95%CI: -1.03 to 2.38,P= 0.44; Figure 4B)[4,13,15-19], recurrence rate (OR = 0.97,95%CI: 0.73 to 1.30,P= 0.85; Figure 5)[7,13,17-19,21-23], 5-year overall survival (OR =0.94, 95%CI: 0.61 to 1.44,P= 0.77; Figure 6A)[7,14,15,17,18,21,23], or 5-year disease-free survival (OR = 0.86, 95%CI: 0.65 to 1.14,P= 0.29; Figure 6B)[7,14,17,21,23] between the LL and HL groups.
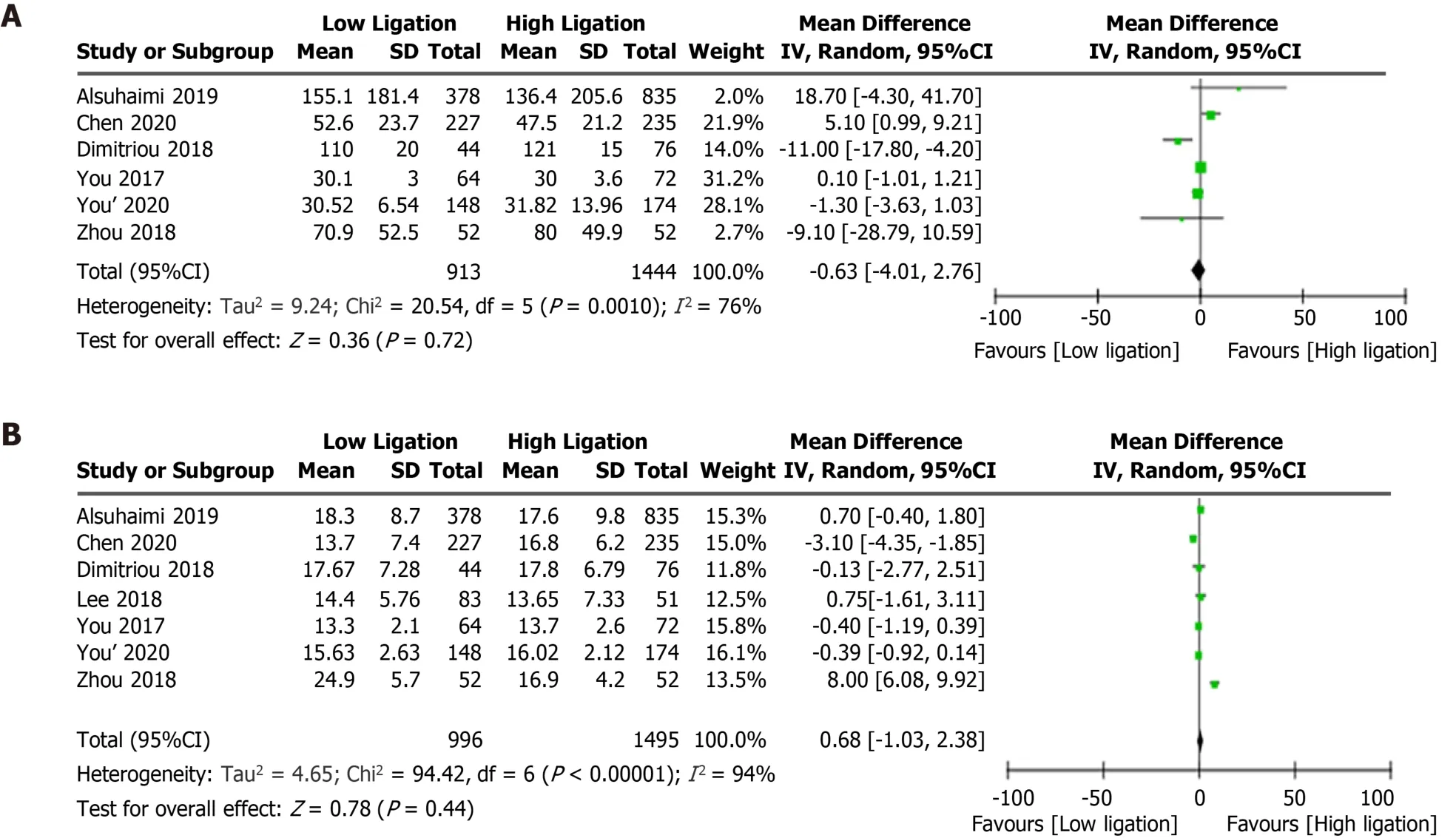
Figure 4 Forest plots for intraoperative indexes of low ligation and high ligation. A: Blood loss; B: Total lymph nodes harvested.
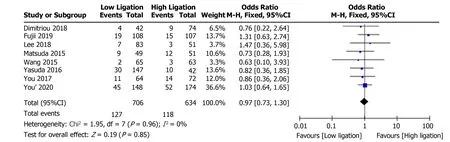
Figure 5 Forest plot for tumor recurrence following low ligation and high ligation.
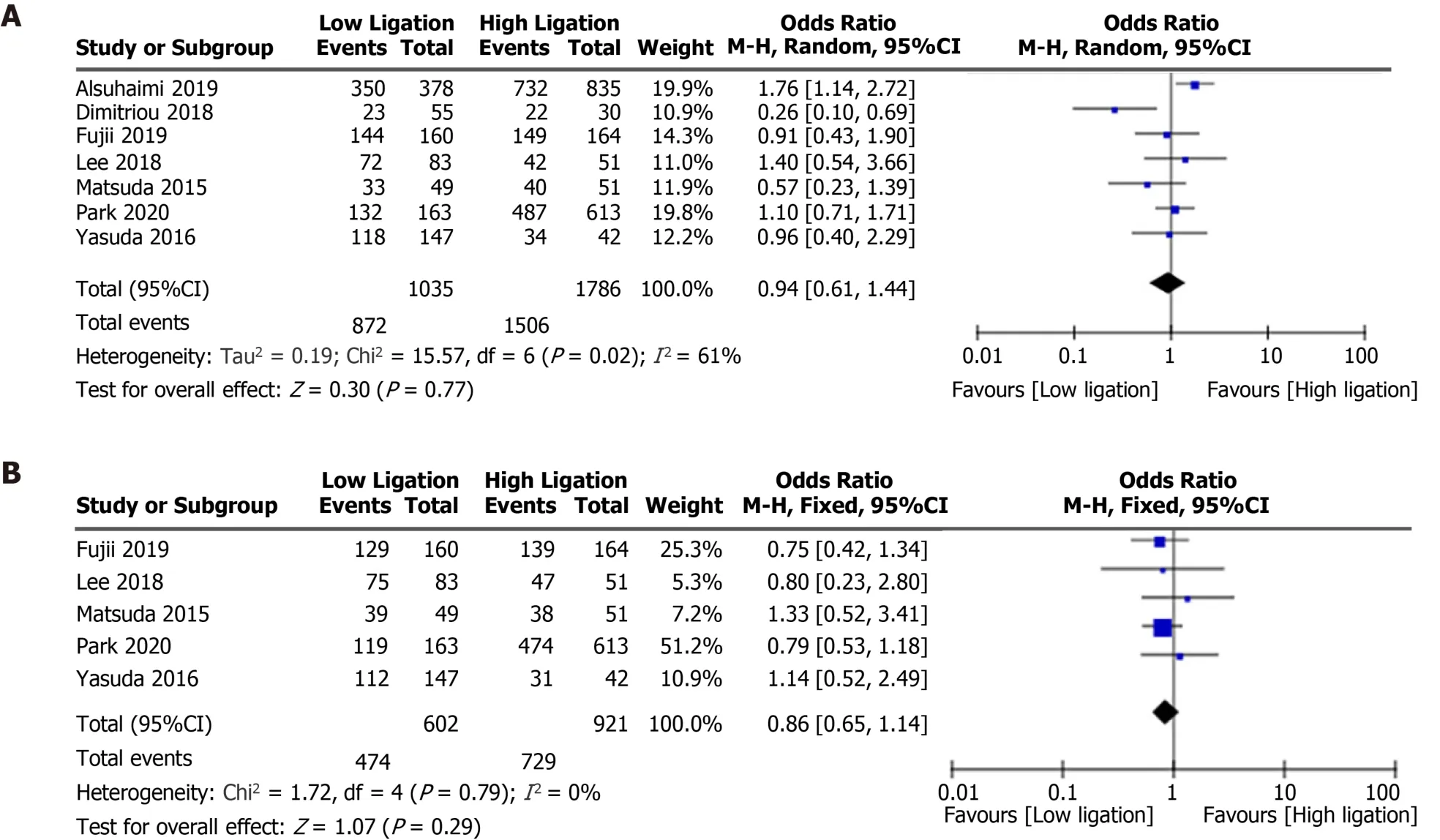
Figure 6 Forest plots for 5-year overall survival following low ligation and high ligation. A: 5-year overall survival; B: 5-year disease-free survival.
DISCUSSION
Radical resection is the most efficient way to surgically treat sigmoid colon and rectal cancer. However, the best ligation site of the IMA has been controversial for more than 100 years. The current controversy mainly involves the influence on lymph node dissection, anastomotic blood supply, postoperative autonomic function, and prognosis. Some safety and oncological outcomes following LL and HL have been investigated in previous reviews[8-10,24,25], all of which reported that LL decreased the incidence of anastomotic leakage, except for one meta-analysis that included only RCTs. A meta-analysis carried out by Hajibandehet al[8] demonstrated that there was no significant difference in anastomotic leakage rate between the two ligation positions of the IMA. These earlier reviews also found no difference in terms of the number of lymph nodes harvested or the survival rate. Our meta-analysis, on the other hand,mainly evaluated functional outcomes and found that LL was associated with a lower risk of anastomotic stenosis, which was also related to anastomotic tension and anastomotic blood supply.
Urinary and sexual dysfunction after CRC surgery are inevitable problems,associated with injury to the superior hypogastric plexus[26]. Some studies[5,6]demonstrated that LL was associated with a lower risk of postoperative genitourinary dysfunction. One randomized study, however, found that LL was not superior to HL in preserving urinary function in an anterior resection and the authors believed that LL was a more complex procedure[7]. Although we found that LL was associated with a decreased risk of urinary infection, we found no difference between the two techniques regarding urinary dysfunction and urinary retention. Our conclusion is opposite to that of Siet al[10], who found that LL was associated with less postoperative urinary dysfunction. Two clinical trials used genitourinary dysfunction to evaluate both sexual and voiding dysfunction; this limitation did not allow us to draw a definitive conclusion on sexual dysfunction.
Impaired bowel function is also a common complication after CRC surgery. Factors affecting bowel function are complex and include rectal compliance, anal sphincter function, and pelvic floor muscle contraction. The regulation of defecatory function is closely controlled by the sympathetic and parasympathetic nerves from the superior and inferior hypogastric plexus[26]. Although previous trials acquired the data at different months after surgery, acute peripheral nerve injury may take up to 6 mo to heal[27]. We therefore used Wexner’s incontinence score[28], nocturnal bowel movement, and the number of patients using antidiarrheals and laxatives 1 year after surgery to compare bowel function following the two ligation techniques.
Motility of the neorectum is closely associated with defecatory function and it has been suggested that long denervation of the neorectum following HL leads to impaired bowel function[29]. Less propagated contraction and more spastic microcontraction were observed in patients with long denervation. Although other indicators related to bowel function were difficult to analyze because of the limitation of data extraction, we found that the LL may result in better bowel control.
Anastomotic stenosis, which is one factor used to evaluate the quality of life of patients who have undergone colorectal surgery, is similar to anastomotic leakage.When the diameter of the anastomosis is less than 12 mm, with or without intestinal obstruction, it is defined as an anastomotic stenosis, whose pathological basis is the hyperplasia of fibrous tissue caused by hypoxia[30]. Anastomotic leakage is also regarded as an essential cause of anastomotic stenosis[31]. Our results showed no difference in the incidence of anastomotic leakage, but LL was associated with a lower incidence of anastomotic stenosis. Although the analyses of anastomotic leakage and anastomotic stenosis included 13 studies and 4 studies, respectively, they did not have high heterogeneity.
From an oncological perspective, some surgeons believe that HL during radical resection of sigmoid CRC can allow removal of more lymph nodes and improve the prognosis of patients. Others, however, believe that metastasis of apical lymph nodes is rare, and that the survival rate following LL is not inferior to that following HL.There was little difference in total recurrence rate, number of lymph nodes harvested,5-year overall survival, or 5-year disease-free survival between the two levels of ligation of the IMA in our meta-analysis.
Since autonomic function could greatly affect the quality of life of patients, we compared the outcomes of two levels of ligations of the IMA on postoperative urinary,sexual, and defecatory function. This meta-analysis can provide surgeons with suggestions for the best IMA ligation technique during radical resection of sigmoid CRC. Our meta-analysis has some limitations and there are several confounding factors, such as neoadjuvant therapy, adjuvant therapy, tumor stage, operative approach, surgical technology, and preventive stoma. Functional outcomes were not completely clear because some studies did not evaluate the preoperative genitourinary and bowel function of the patients and functional outcomes were not determined at a consistent time after surgery. Both of these factors may affect the judging of functional outcomes and we hope that future studies will address these issues.
CONCLUSION
LL may result in better bowel function and reduce the rate of anastomotic stenosis.The risk of urinary dysfunction and anastomotic leakage, however, seems to be equivalent between the two IMA ligation techniques. Since LL is less invasive and does not increase operative time, we recommend LL of the IMA in sigmoid colon and rectal cancer surgery. Future studies are needed to confirm our conclusions.
ARTICLE HIGHLIGHTS
Research background
Whether the benefits of low ligation (LL) of the inferior mesenteric artery (IMA)during colorectal cancer (CRC) surgeries extend to improved genitourinary and defecatory function is still controversial.
Research motivation
Previous studies have demonstrated that LL was associated with a lower risk of postoperative genitourinary and defecatory dysfunction in patients with CRC. One randomized study, however, found that LL was not superior to high ligation (HL) in preserving urinary function. Therefore, we carried out a meta-analysis to systemically compare functional outcomes of patients with CRC between LL and HL of the IMA.
Research objectives
To evaluate the effect of LL of the IMA on genitourinary function and defecation for patients after CRC surgeries.
Research methods
The meta-analysis methods were adopted to realize the objectives. And statistical analyses were performed using Review Manager 5.3 software.
Research results
LL resulted in a significantly lower incidence of nocturnal bowel movement (OR =0.73, 95%CI: 0.55 to 0.97, P = 0.03) and anastomotic stenosis (OR = 0.31, 95%CI: 0.16 to 0.62, P = 0.0009) compared with HL. The risk of postoperative urinary dysfunction,however, did not differ significantly between the two techniques. The meta-analysis also showed no significant differences between LL and HL in terms of anastomotic leakage, postoperative complications, total lymph nodes harvested, blood loss,operation time, tumor recurrence, mortality, 5-year overall survival rate, or 5-year disease-free survival rate.
Research conclusions
Since LL may result in better bowel function and a reduced rate of anastomotic stenosis following CRC surgeries, we suggest that LL be preferred over HL.
Research perspectives
Some limitations in this meta-analysis should be addressed carefully. First, since both randomized controlled trials and non-randomized studies were included, the randomization in the original research was limited. Second, several studies did not evaluate the preoperative genitourinary and bowel function of the patients and functional outcomes were not determined at a consistent time after surgery. In addition, there were differences in the neoadjuvant therapy, adjuvant therapy, surgical approach, and preventive stoma in this analysis. All of these factors may affect the results. Future studies are needed to address these issues.
ACKNOWLEDGEMENTS
We thank all the previous study authors whose work is included in this meta-analysis.
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- Paradigm shift in gastrointestinaI surgery - combating sarcopenia with prehabiIitation: MuItimodaI review of cIinicaI and scientific data
- Impact of COVID-19 on presentation, management, and outcomes of acute care surgery for gallbladder disease and acute appendicitis
- Reappraisal of surgical decision-making in patients with splenic sclerosing angiomatoid nodular transformation: Case series and literature review
- Robotic transanal total mesorectal excision: Is the future now?
- Persistent bowel dysfunction after surgery for Hirschsprung’s disease: A neuropathological perspective
- Associating liver partition and portal vein ligation for staged hepatectomy in the treatment of colorectal cancer liver metastases