Effect of vision loss on plasticity of the head and neck proprioception
2021-07-09TianYuJiangBinShiDongMeiWuLinZhangChangShuiWengLiHaiZhang
Tian-Yu Jiang, Bin Shi, Dong-Mei Wu, Lin Zhang, Chang-Shui Weng, Li-Hai Zhang
Abstract
· KEYWORDS: blindness; vision; neuronal plasticity;proprioception; rehabilitation
INTRODUCTION
Vision plays a very important role in sensorimotor control[1]. The integrated coordination of peripheral sensory afferent, central nervous system, and efferent control constitute the loop of sensorimotor control[2]. The integration and collaboration of the vestibular sense, proprioception,optesthesia, and central nervous system processing, as well as various simultaneous feedbacks, are important properties of this loop[3].
Studies have demonstrated that the loss of one sensation has a far‐reaching impact on the integration and coordination of other sensations and the central nervous system[4]. This complex interaction could lead to different degrees of compensatory substitutions and changes in the plasticity of other sensations and the central nervous system[5‐6]. Long‐term vision loss in the blind will lead to various long‐term plasticity changes in other receptors and the central nervous system[6]. As a functional compensation, plasticity changes in the central nervous system will manifest during the early stages of blindness[6],and in other receptors, such as in auditory sensation[7], tactile sensation[8‐9], proprioception[10]and vestibular sensation[5]. The plasticity of the central nervous system and the compensatory enhancement of multiple sensations often synchronize to influence and shape each other[5]. Ⅰndividuals who are blind will have different motor preparation and implementation methods compared to the sighted, such as walking, object reaching,etc[10‐11]. However, several studies have found that the behavior and motor performance of spatial cognition in the blind is not better compared to blindfolded sighted people[11‐12].Ⅰndividuals who are blind do not develop special kinesthesis abilities compared to the sighted[12]. Hence, there is still controversy as to whether long‐term vision loss could lead to the enhancement of proprioception and sensorimotor control.Ⅰn this study, head repositioning test (HRT) was used to determine whether there were difference among the sujects in the proprioception and motion control of the head and neck. HRT is a simple kinesthesis test performed on the head and neck that was developed by Revelet al[13]in 1991. The HRT reveals changes in proprioception of the head and neck.The test is performed by maximum movement of the head on the horizontal or vertical plane. Afterward, the individual repositions his/her head as close as possible to the initial self‐perceived straight‐ahead position. The sensitivities of the proprioception and motor control abilities of the head and neck are then determined by calculating the repositioning error.Although HRT measures only one aspect of proprioceptive function, the sensation of position, it can also reflect the proprioceptive and motor function of the head and neck.Several studies have demonstrated that HRT is a reliable and valid method[14‐17].
So, we analyzed the HRT difference among the blind, low vision and sighted subjects, and discussed whether the proprioception and motion control of the head and neck of blind and low vision individuals were compensated due to long‐term vision loss or impairment.
SUBJECTS AND METHODS
Ethical ApprovalThis study was approved by the Ethics Committee of PLA General Hospital (certificate approval number: S2018‐048‐01). All enrolled individuals signed written informed consent.
Inclusion CriteriaⅠndividuals who were blind, low vision or sighted were included in the study. Βased on the World Health Organization (WHO) standard, blind subjects refer to individuals who have visual acuity of less than or equal to 3/60(0.05), or light sensation after standard refractive correction or ophthalmic treatment. Low vision subjects refer to individuals who have visual acuity of 6/18 (0.3) to just light sensation or with the visual field radius of less than 10° but can use their residual vision to arrange or perform certain tasks after standard refractive correction or ophthalmic treatment. Sighted subjects refer to individuals with visual acuity greater than 6/18 (0.3) after standard refractive correction or ophthalmic treatment[18].

Figure 1 Individuals were seated and blindfolded, with their back upright and resting on the chair The center of the head was 300 cm from the wall.
Exclusion CriteriaⅠndividuals were excluded from the study if they had the following conditions: history of whiplash or other cervical spine injury or pain, a history of dizziness or vertigo and neck pain in the last week, a history of diseases that could affect physical movement, diseases of the nervous system, pregnancy.
Head Repositioning Test ProcedureAs shown in Figure 1, the laser indicator was positioned to the center of the large white paper (90×100 cm2) affixed to the wall. After the laser indicator was turned on, the subjectʼs face was oriented towards the self‐perceived straight‐ahead position for 3s. The initial position of the laser beam projection on the large white paper was then marked. The subject then slowly turned his/her head to the left to the maximum, then slowly repositioned to the initial position and maintained for 3s. The new position was then marked. Then the head was turned to the right following the same instructions above. The test was repeated five times for each side. After a two minute break, the “head tilt down and up” test was performed and the positions were marked accordingly[13].
Head Repositioning Test Data Collection and Preliminary ProcessingAs shown in Figure 2, the coordinates of the repositioning position G for each subject and each test were measured. The repositioning errors were calculated using the arctangent function. The global repositioning error was used to calculate CE, AE, VE and RMSE for each subject[19].
Gxy is repositioning errors, which unit of scale is angular unit,degree. The formula is followed by:

Figure 2 Point O represents the initial position of the laser beam projection, while point G represents the position of laser beam projection when the subject turned his/her head to one side with maximum amplitude and then returned to the initial straightahead position, with coordinate (x, y) The distance of O‐G was converted into an angle to represent the global repositioning error,points H and V represents the perpendicular projection of G on the horizontal and vertical lines, respectively.

CE is constant error. The formula is followed by:
AE is absolute error. The formula is followed by:

VE is variable error. The formula is followed by:
RMSE is root mean square error. The formula is followed by:
Statistical AnalysisData were analyzed using the SAS 9.4.Tukey‐Kramer for one‐way ANOVA was used to compare blind, low vision and sighted subjects, as well as to compare subjects with balanced vision, strong vision in the left eye and strong vision in the right eye. Ⅰndependent samplet‐test was used to compare subjects with congenital blindness and acquired blindness, as well as left and right hand dominance subjects.
RESULTS
Totally 25 blind subjects, 31 low vision subjects, and 34 sighted subjects were enrolled in this study. Among the blind subjects, 14 individuals had congenital blindness while 11 individuals had acquired blindness. Among the blind and low vision subjects, 21 individuals had balanced binocular vision,17 had strong vision in the left eye and 18 had strong vision inthe right eye. Among all subjects, 11 individuals were left hand dominance, and 79 were right hand dominance.

Table 1 HRT performance for blind, low vision, and sighted subjects mean±SD
Head Repositioning Test Analysis of Blind, Low Vision,and Sighted SubjectsWith regards to the head rotation test,there was no statistical differences in CE (P=0.0756), however,statistical differences were observed for AE, VE and RMSE(P=0.0035,P=0.0004,P=0.0004, respectively; Table 1). With regards to blind and sighted subjects, there were no statistical differences in CE (P>0.05), while statistical differences were observed for AE, VE and RMSE (P<0.01,P<0.001,P<0.001,respectively). Βetween low vision and sighted subjects, there were no statistical differences in CE and AE (P>0.05), while statistical differences were observed for VE and RMSE(P<0.05). Βetween blind and low vision subjects, there were no statistical differences in CE, AE, VE and RMSE (P>0.05;Figure 3). Furthermore, there were no statistical differences in the “head tilt down and up” test between the groups (P>0.05).Comprehensive analysis demonstrated that the accuracy of head repositioning of the blind and low vision subjects was worse compared to sighted subjects, with greater variance in head repositioning. There was no difference in head repositioning error between blind and low vision subjects.The comparison of the combination of blind and low vision subjects with sighted subjects, the head repositioning ability of the blind subjects seemed to be the worst. Figure 4 shows HRT scatter plots of three representative subjects from each group.
Head Repositioning Test Analysis of Subjects with Congenital and Acquired BlindnessStatistical differences were observed in CE and AE of head right rotation and CE of general head rotation in congenitally blind subjects (P=0.05,P=0.042 andP=0.000, respectively), while no statistical differences (P>0.05) were observed for the other parameters.This indicated lower HRT performance in congenitally blind subjects (Table 2).
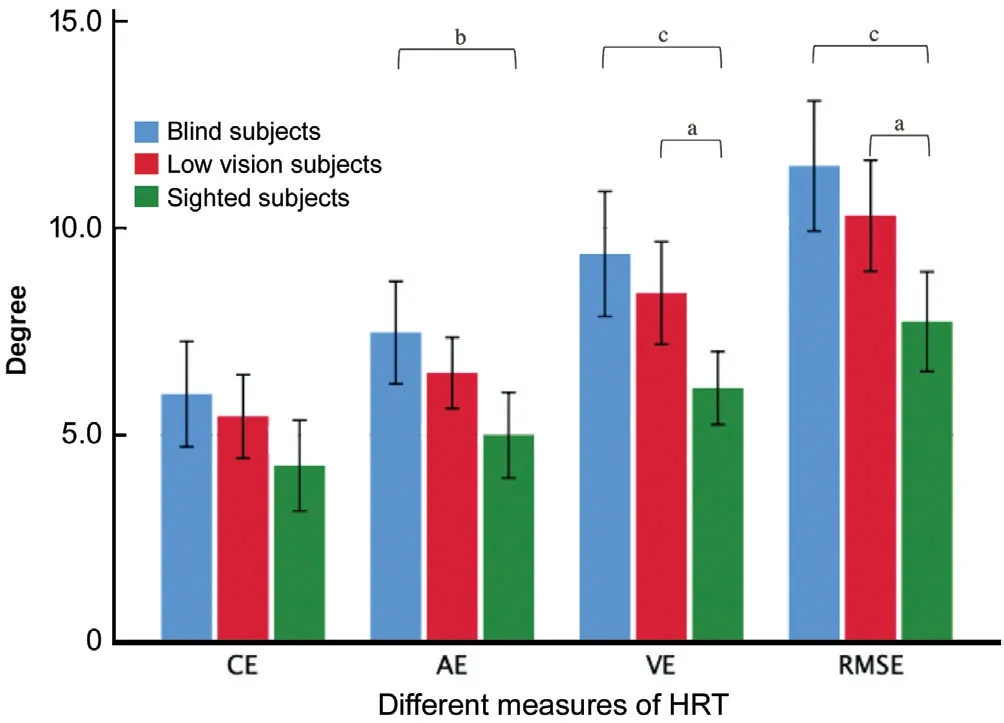
Figure 3 Comparison of HRT in blind, low vision, and sighted subjects aP<0.05, bP<0.01, cP<0.001. CE: Constant error, AE:Absolute error, VE: Variable error, RMSE: Root mean square error,SD: Standard deviation.
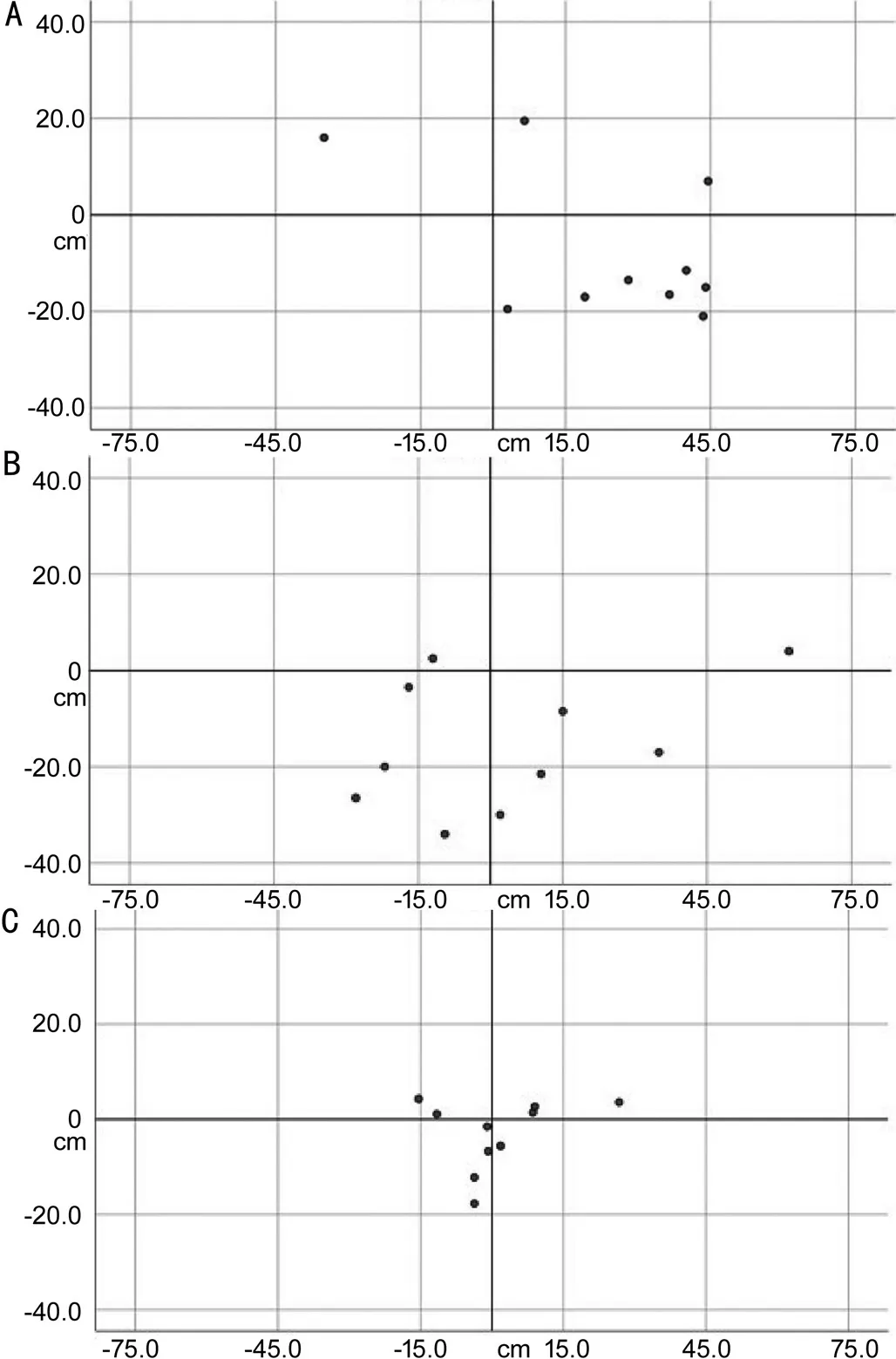
Figure 4 The positioning results for HRT in blind, low vision,and sighted subjects, respectively The horizontal axis represents the X axis, the vertical axis represents the Y axis, the origin is in the center. The results showed higher accuracy and precision for head repositioning in sighted subjects. A: The scatter plot for blind subjects; Β: The scatter plot for low vision; C: The scatter plot for sighted subjects.
Head Repositioning Test Analysis of Left and Right Hand Dominance SubjectsNo significant differences were observed between left and right hand dominance blind, low vision and sighted subjects (P>0.05; Table 2).
Head Repositioning Test Analysis of Subjects with and Without Balanced VisionAmong the blind and low vision subjects, no statistical differences between subjects with balanced binocular vision, strong vision in the left eye and strong vision in the right eye were observed (P>0.05; Table 3).
DISCUSSION
HRT is a simple and valid test to determine the sensitivity of head and neck movement. Ⅰn 1906, Slinger and Horsley[20]proposed the use of a simple target matching task to test the accuracy of upper limb movements. Ⅰn 1991, using the same principle, Revelet al[13]were the first to use HRT to determine the proprioceptive function and motor control of the head and neck. Subsequently, numerous studies have utilized HRT to study motor control ability of the head and neck. These include investigating neck pain[21], low back pain[15]and spine‐related diseases[16], as well as studies related to exercise training[17].The use and reliability of HRT have been validated[14,22].
Ⅰn this study, coordinate values were used to calculate the global repositioning error. CE reflects the direction and magnitude of the repositioning error[19], AE[23]and RMSE[19]reflects the accuracy of the general head repositioning and VE reflects the variation of the head repositioning[19,23],i.e.the stability of repositioning. Comprehensive analysis of our results demonstrated that compared to sighted subjects, the accuracy of head repositioning was worse in blind and low vision subjects and had greater variation in repositioning. However,no difference in the accuracy of head repositioning between blind and low vision subjects was observed. The accuracy of repositioning was worse in congenitally blind subjects while there were no differences in HRT performance between left and right hand dominance subjects and between visually balanced and unbalanced subjects. Ⅰnterestingly, the combined comparison of blind and low vision subjects with sighted subjects, HRT performance seemed worse in blind subjects.
Hence, our study does not prove that long‐term vision loss or impairment leads to better HRT performance due to compensatory enhancement of other sensations. The reasons may be as follows.
First, the motor control of the head and neck is very complex.The central nervous system is directly connected to the cervical proprioceptor, visual and vestibular systems through the vestibular nucleus and the cervical central nucleus[24].Through oculocephalic and vestibulocolic reflexes,etc.theeyeball is stabilized in an appropriate position, vision stability is maintained, the position of the head in space and direction relative to the trunk is corrected, and correct body positioning and balance control is maintained to attain motor control of the whole body[21]. Ⅰn addition, there are more mechanoreceptors in the articular capsule, ligaments and deep muscles of the upper cervical segment compared to other regions[24]. This all indicates that sensorimotor control of the head and neck is crucial to the physical body, and any changes or dysfunction may cause several clinical symptoms, such as dizziness,vertigo, blurred vision, cervicogenic headache, and cognitive problems[24]. Hence, HRT in blind subjects does not only represent the proprioceptive ability of the head and neck, even though proprioception is compensatively enhanced. Thus, it may not be indicated by HRT in this study.
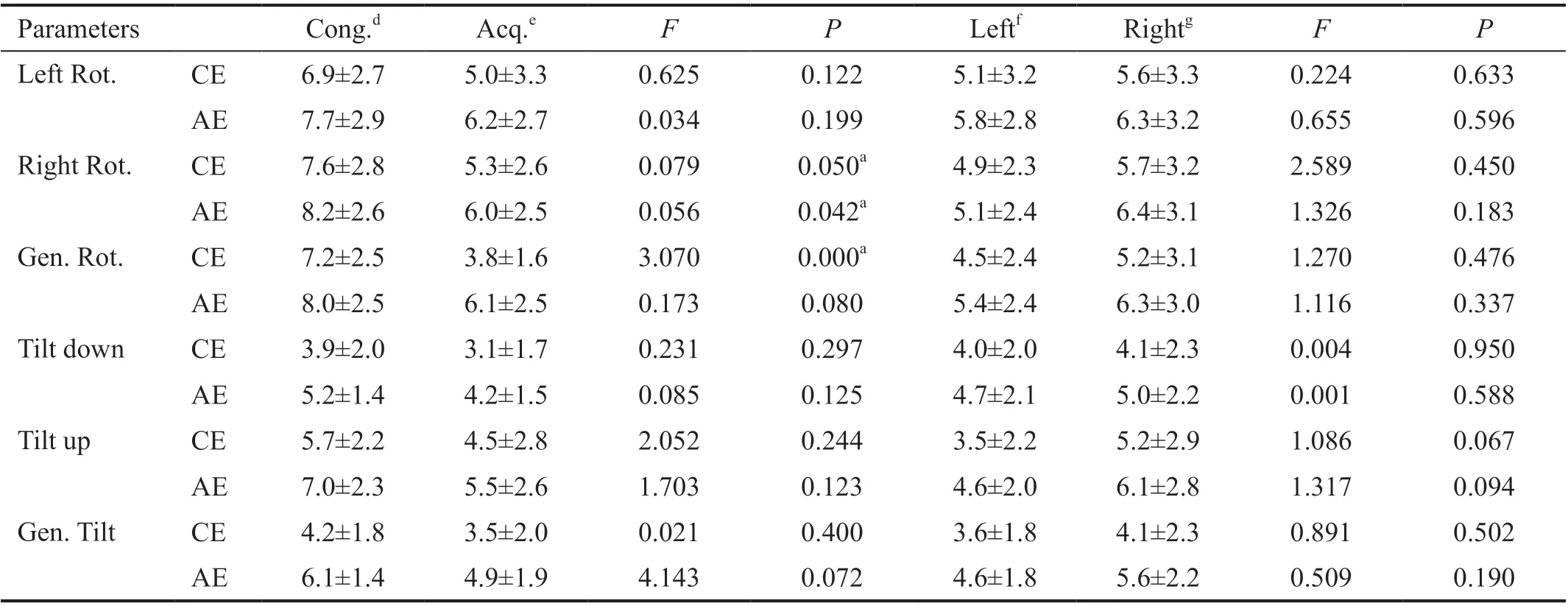
Table 2 HRT results of congenital and acquired blindness, and left and right hand dominance subjects mean±SD

Table 3 HRT results of subjects with and without balanced vision mean±SD
Second, due to the complexity of sensorimotor control of the head and neck, vision loss or impairment do not necessarily enhance the proprioception and motor control of the head and neck. The walk orientation test performed by Rivenes and Cordellos[12]showed no difference in the performance of blind subjects versus blindfolded sighted subjects. This suggests that blind subjects did not develop special kinesthetic abilities. Parreiraet al[25]reviewed several studies to show that even thou blind subjects had compensatory substitutions for other sensations, they did not achieve good motor control.Hence, sensorimotor control of the head and neck was not compensated by long‐term vision loss or impairment.Consequently, blind and low vision subjects had a lower performance.
Finally, due to vision loss or impairment, physical fitness and exercise are much lower in blind or low vision individuals compared to sighted individuals[26‐27]. This may be a factor why HRT performance in blind or low vision individuals is lower compared to sighted individuals. An orienteering test performed on blind individuals by Seemungalet al[28]showed that vision affected the development of vestibular function. Hence, orienteering ability in the blind was lower compared to blindfolded sighted individuals. However, the authors found that early visual and cognitive experience contributed to vestibular orienteering function. This suggested that long‐term orientation and exercise should help improve orienteering activity in the blind. Ⅰn addition, our study found that, compared with congenital blind people, the repositioning accuracy of HRT was better in acquired blind people. This indicated that acquired short‐term visual experience had a long‐term and far‐reaching effect on the plasticity of the proprioception and motor control of the head and neck.The proprioception and motor control of the head and neck in congenitally blind people were lower due to the lack of visual experience. These were consistent with the findings by Seemungalet al[28]. Hence, the presence of vision has long‐term effects on the plasticity of the sensorimotor control system[28]. To compensate for the impact of vision loss, it is possible to improve HRT performance by strengthening sensorimotor control training of the head and neck in blind and low vision individuals.
This study did not observe any effects on proprioception and motor control of head and neck in left or right hand dominance individuals and in individuals with binocular visual imbalance.Ⅰn addition, no statistical difference was observed in the“head tilt down and up” test in all control studies. Previous studies have demonstrated that, due to the strong stimulation of the vestibular nervous system induced by backward head movement[29], there was significant impedance during the “head tilt down and up” resulting in high variation of HRT results[21].Thus, there were no statistical differences were observed in this study.
The results of the study can be used to explain that 1) We should emphasize the important role of optesthesia training in proprioception and sensorimotor control training; 2) To compensate for vision loss, only intensive motor training can achieve better proprioception and motor control ability; 3)The impact on motor vehicle driving is not only optesthesia factors, but also the limited development of proprioception and sensorimotor control due to vision impairment.
Ⅰn conclusion, the proprioception and motor control of the head and neck do not improve in blind and low vision individuals with long‐term vision loss or impairment. Acquired experience contributes to HRT performance in the blind, and vision has long‐lasting and far‐reaching effects on the plasticity of the development of sensorimotor control.
ACKNOWLEDGEMENTS
Thanks to Ms. Lili Wang and my colleagues for scientific advice and data collection, thanks to professor Xiutang Cao for statistical analysis, thanks to Dr. Guy Simoneau for his scientific advice.
Authors’ contributions:Jiang TY, Weng CS, Zhang LH contributed to the conception of the study; Jiang TY, Shi Β, Wu DM, Zhang L performed the experiment; Jiang TY,Shi Β contributed significantly to analysis and manuscript preparation; Jiang TY, Shi Β performed the data analyses and wrote the manuscript; Jiang TY, Shi Β, Wu DM, Zhang L, Weng CS, Zhang LH helped perform the analysis with constructive discussions.
Foundations:Supported by National Key R&D Program of China (No.2018YFC2001400); Special Research Topic of Health Care (No.13ΒJZ53; No.18ΒJZ34); Βeijing Municipal Science and Technology Commission (No.Z191100004419006).
Conflicts of Interest: Jiang TY,None;Shi B,None;Wu DM,None;Zhang L,None;Weng CS,None;Zhang LH,None.
杂志排行
International Journal of Ophthalmology的其它文章
- Evaluation of preoperative dry eye in people undergoing corneal refractive surgery to correct myopia
- Atherogenic indices in non-arteritic ischemic optic neuropathy
- Ragweed pollen induces allergic conjunctivitis immune tolerance in mice via regulation of the NF-κB signal pathway
- Quantitative analysis of retinal intermediate and deep capillary plexus in patients with retinal deep vascular complex ischemia
- Predictive value of pupillography on intraoperative floppy iris syndrome in preoperative period
- Comparison of lOL-Master 700 and lOL-Master 500 biometers in ocular biological parameters of adolescents