Effect of mild moxibustion on cancer-related fatigue,serum ghrelin and adiponectin in patients undergoing chemotherapy after colorectal cancer surgery
2021-06-22LuoQian罗茜ChenJiaquan陈佳权
Luo Qian (罗茜), Chen Jia-quan (陈佳权)
Central Hospital of Enshi Tujia and Miao Autonomous Prefecture, Hubei 445000, China
Abstract Objective: To observe the effect of mild moxibustion on cancer-related fatigue, serum ghrelin and adiponectin in patients undergoing chemotherapy after colorectal cancer surgery.
Keywords: Moxibustion Therapy; Moxa Stick Moxibustion; Drug Therapy; Drug-related Side Effects and Adverse Reactions;Colorectal Neoplasms; Fatigue; Ghrelin; Adiponectin
Colorectal cancer, including colon cancer and rectal cancer, are common clinical malignant tumors of the digestive tract, with high morbidity and mortality[1].Surgery combined with chemotherapy is the only way to radically cure colorectal cancer, as it improves the clinical symptoms and increases the survival rate of patients to some extent[2]. However, cancer-caused body-environment changes and chemotherapeutic drugs-caused damage to normal cells can result in cancer-related fatigue (CRF). CRF specifically refers to a painful, persistent, subjective, physical, emotional, and cognitive fatigue or exhaustion that is related to cancer and cancer treatment and not consistent with the recent activity[3]. CRF runs through the entire process of tumor occurrence, treatment, progression, and rehabilitation, seriously affecting the treatment and quality of life in the patients. At present, no therapeutic drug can evidently improve CRF, and drug intervention is mainly aimed at tumor complications or symptomatic treatment to improve CRF[4]. The clinical intervention methods of CRF are mainly non-drug therapies such as health education consultation,nutritional support, and exercise intervention. In recent years, acupuncture therapy has been widely used in malignant tumor treatment to reduce the adverse reactions of radiotherapy and chemotherapy, alleviate cancer pain and improve quality of life in the patients,showing a good application prospect[5-6]. In this study,the effects of mild moxibustion treatment on CRF,serum ghrelin and adiponectin in patients undergoing chemotherapy after colorectal cancer surgery were investigated. The results are as follows.
1 Clinical Materials
1.1 Case selection
1.1.1 Western medicine diagnostic criteria
① Met the diagnostic criteria of colorectal cancer in the Chinese Guidelines for Diagnosis and Treatment of Colorectal Cancer (2015 Edition)[7], with pathological diagnosis; ② CRF diagnostic criteria referred theInternational Classification of Diseases (ICD-10)Application Guide[8]: recurrent fatigue symptoms last for more than 2 weeks, accompanied by 5 or more symptoms, including general weakness or heavy limbs;unable to concentrate; depression, loss of interest and lack of passion; insomnia or drowsiness; failure to recover energy after sleep; difficulty in activities;emotional reactions such as sadness, frustration, and irritability; unable to complete competent daily activities as usual; short-term memory loss; fatigue symptoms persisting for several hours without improvement.
1.1.2 Syndrome differentiation standard in traditional Chinese medicine (TCM)
The syndrome differentiation criteria of spleen and kidney yang deficiency in theGuiding Principles for Clinical Study of New Chinese Medicineswere referred[9]. The main symptoms included fatigue,depression, soreness and weakness of waist and knees,chills with cold limbs, chronic diarrhea or diarrhea with undigested food. The secondary symptoms included cold and pain in the abdomen, edema and oliguria,pale-puffy tongue with white and slippery coating, and sunken-slow-weak pulse.
1.2 Inclusion criteria
Met the Western medicine diagnostic criteria for colorectal cancer and CRF; met the syndrome differentiation criteria for spleen and kidney yang deficiency in TCM; well recovered patients 1 month after surgery and receiving chemotherapy; 10-70 years old; expected survival time more than 6 months;voluntarily participated in this trial and signed an informed consent.
1.3 Exclusion criteria
Patients receiving hormones or other psychostimulants; patients with fatigue caused by muscle relaxants or sedatives; patients with serious primary diseases such as cardiovascular,cerebrovascular, liver or kidney disorders;breastfeeding or pregnant women; patients with definitively mental illnesses or psychological diseases.
1.4 Elimination and dropout criteria
Patients whose condition was deteriorated during the trial; those voluntarily asked to withdraw from the trial, terminated chemotherapy, or had incomplete data.
1.5 Statistical methods
The SPSS version 20.0 software was applied to analyze the data. The measurement data in normal distribution were represented as mean ± standard deviation (±s). Self-comparison was performed by pairedt-test, and groupt-test was used for comparison between groups. Chi-square test was used for the rate comparison of the numeration data.P<0.05 indicated statistically significant difference.
1.6 General information
A total of 70 colorectal cancer patients undergoing chemotherapy in our hospital between May 2016 and December 2018 were selected. A random number table was generated by computer. Random numbers were assigned to patients according to the enrollment sequence and divided into a control group and an observation group, with 35 cases in each group. During the trial, 2 cases in the control group and 1 case in the observation group dropped out due to worsened condition. Therefore, 33 valid samples in the control group and 34 valid samples in the observation group were remained. There were no statistically significant differences between the two groups in patients’general information, including gender, age, and cancer type (allP>0.05), (Table 1).

Table 1. Comparison of general information between the two groups
2 Treatment Methods
Patients in both groups were treated with conventional FOLFOX4 chemotherapy regimen:intravenous administration of oxaliplatin (85 mg/m2) for 2 h on the first day; intravenous administration of calcium folinate (200 mg/m2) for 2 h, and 5-fluorouracil(400 mg/m2) for 30 min on the first and second days.Fourteen days was a chemotherapy cycle.
2.1 Control group
Patients in the control group received conventional chemotherapy combined with symptomatic treatment of complications, health education, nutritional support,and exercise intervention for 3 consecutive chemotherapy cycles.
2.2 Observation group
Patients in the observation group received mild moxibustion on the basis of interventions used in the control group.
Acupoints: Shenque (CV 8), Guanyuan (CV 4), and bilateral Zusanli (ST 36), Pishu (BL 20) and Shenshu(BL 23).
Methods:Pure moxa sticks with a diameter of 1.8 cm and a length of 20 cm (Nanyang Hanyi Moxa Co., Ltd.,China) were used. Patients first exposed skin of acupoint area in a supine position. The operator lighted the moxa stick and performed moxibustion at a distance of 2-3 cm from the acupoint skin. It is better for the patients to feel local warmth without burning pain. Each acupoint received moxibustion for about 10 min with local skin flushing[10]. After moxibustion at acupoints in a supine position, the above steps were repeated in a prone position to complete the moxibustion at all selected acupoints. Moxibustion was performed once every other day for 3 consecutive chemotherapy cycles.
3 Observation Items and Results
3.1 Observation items
3.1.1 Piper fatigue scale-revision (PFS-R)
Before and after treatment, PFS-R assessments were performed by physicians who did not know the group and treatment status. There are 22 items in PFS-R,covering 4 dimensions of behavior, emotion, feeling and cognition. A 0-10 points scoring method was used for each dimension. 0 point indicated no fatigue, and 10 points indicated the most serious fatigue[11]. The total of the four-dimension scores was used as PFS-R score.
3.1.2 Karnofsky performance status (KPS) score
KPS score was evaluated by physicians who were blind to the grouping and treatment status to determine the functional conditions of patients before and after treatment. The higher score, the better quality of life and the more one can tolerate treatment-related adverse effects[12].
3.1.3 Score of spleen and kidney yang deficiency syndrome
It was evaluated by a physician who did not know the grouping and treatment status based on the syndrome differentiation criteria of spleen and kidney yang deficiency developed according to theGuiding Principles for Clinical Study of New Chinese Medicines[9]. Patients were divided into 4 grades (0-3 points) according to the severity of the main symptoms of spleen and kidney yang deficiency, including fatigue, depression, chills with cold limbs, soreness and weakness of waist and knees, and abnormal stools. The higher the total score, the more severe the findings of the spleen and kidney yang deficiency.
3.1.4 Serological indicators
Early morning fasting venous blood was collected from patients of the two groups before and after treatment,and the serum ghrelin and adiponectin levels were determined by enzyme-linked immunosorbent assay.
3.2 Results
3.2.1 PFS-R score comparison
Before treatment, there were no statistical differences between the two groups in the behavior, emotion,feeling, cognition scores and the PFS-R total score (allP>0.05). The after-treatment feeling score of the control group was lower than that before treatment (P<0.05),while the behavior, emotion, cognition scores and PFS-R total score did not change significantly (allP>0.05); the behavior, emotion, feeling, cognition scores and PFS-R total score in the observation group were significantly reduced (allP<0.05) and lower than those in the control group (allP<0.05), (Table 2).
3.2.2 Comparison of the KPS score
Before treatment, there was no statistical difference in the KPS score between the two groups (P>0.05). After treatment, the KPS scores of the two groups were increased (bothP<0.05), and it was significantly higher in the observation group than in the control group (P<0.05),(Table 3).
Table 2. Comparisons of the PFS-R scores between the two groups (±s, point)

Table 2. Comparisons of the PFS-R scores between the two groups (±s, point)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time point Behavior Emotion Feeling Cognition Total score Observation 34 Before treatment 6.00±0.85 5.08±1.36 6.08±0.87 5.58±1.41 22.76±2.54 After treatment 4.32±1.011)2) 3.35±1.901)2) 4.41±0.981)2) 4.76±1.441)2) 16.85±2.761)2)Control 33 Before treatment 6.06±0.83 5.18±1.21 6.00±0.79 5.81±1.42 23.06±2.12 After treatment 6.33±0.92 5.27±1.15 5.33±1.141) 6.18±1.62 23.12±2.07
Table 3. Comparison of the KPS score between the two groups(±s, point)
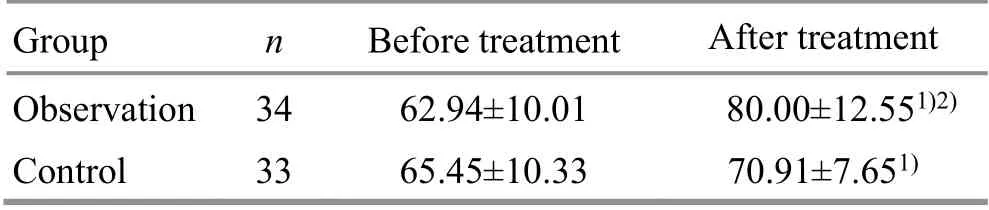
Table 3. Comparison of the KPS score between the two groups(±s, point)
Note: Compared with the same group before treatment, 1) P<0.05;compared with the control group after treatment, 2) P<0.05
Group n Before treatment After treatment Observation 34 62.94±10.01 80.00±12.551)2)Control 33 65.45±10.33 70.91±7.651)
3.2.3 Comparisons of the scores of spleen and kidney yang deficiency syndrome
Before treatment, there were no statistical differences between the two groups in fatigue, depression, chills with cold limbs, soreness and weakness of waist and knees, abnormal stool scores, and total score of spleen and kidney yang deficiency syndrome (allP>0.05). After treatment, the score of soreness and weakness of waist and knees was decreased (P<0.05), while the other scores and the total score of spleen and kidney yang deficiency syndrome in the control group did not change significantly (allP>0.05); while the fatigue, depression,chills with cold limbs scores, and the total score of spleen and kidney yang deficiency syndrome in the observation group were significantly reduced (allP<0.05); meanwhile,the fatigue, depression, chills with cold limbs scores, and the total score of spleen and kidney yang deficiency syndrome in the observation group were lower than those of the control group (allP<0.05), (Table 4).
3.2.4 Comparisons of the serum ghrelin and adiponectin levels
Before treatment, there were no significant differences in the serum ghrelin and adiponectin levels between the two groups (bothP>0.05). After treatment,there were no significant changes in the serum ghrelin and adiponectin levels in the control group (bothP>0.05);while those in the observation group were significantly increased (bothP<0.05), and were both higher than those in the control group (bothP<0.05), (Table 5).
Table 4. Comparisons of the scores of spleen and kidney yang deficiency syndrome between the two groups (±s, point)

Table 4. Comparisons of the scores of spleen and kidney yang deficiency syndrome between the two groups (±s, point)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time Fatigue Depression Chills with cold limbs Soreness and weakness of the low back and knees Abnormal stool Total score Observation 34 Before treatment 2.17±0.83 1.58±0.49 2.08±0.83 1.94±0.74 1.53±0.51 9.32±1.32 After treatment 0.73±0.861)2) 0.82±0.831)2) 0.85±0.891)2) 1.44±0.501) 1.14±0.821) 5.00±1.841)2)Control 33 Before treatment 1.87±0.92 1.51±0.51 2.03±0.85 2.03±0.92 1.54±0.50 9.00±1.50 After treatment 1.55±0.51 1.39±0.49 1.94±0.79 1.51±0.511) 1.57±0.50 7.96±1.15
Table 5. Comparisons of the serum ghrelin and adiponectin levels between the two groups (±s)

Table 5. Comparisons of the serum ghrelin and adiponectin levels between the two groups (±s)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Ghrelin (ng/L) Adiponectin (μg/mL)Before treatment After treatment Before treatment After treatment Observation 34 205.36±16.40 229.09±18.261)2) 10.23±1.32 11.21±1.371)2)Control 33 208.25±13.93 210.89±11.04 10.17±1.43 9.71±1.29
4 Discussion
CRF is common in clinical practice and rarely occurs alone, often accompanied by symptoms such as pain,depression, sleep disturbance, and anemia. The etiology of CRF is complicated, mainly including cancer itself,cancer treatment, cancer and cancer treatment related complications, environment and psychological factors[13].However, the pathogenesis is not clear, though generally believed to be caused by hypothalamic-pituitary-adrenal axis dysfunction, 5-hydrooxytryptamine neurotransmitter disorder, abnormal adenosine triphosphate or muscle metabolism, influence of inflammatory cytokines, and circadian rhythm disorders[14].
CRF belongs to the ‘consumptive disease’ in TCM, and is related to deficiency due to illness, congenital deficiency, spleen and stomach disorders, emotional internal injuries. Spleen is the foundation of acquired nature, the engendering transformation source of qi and blood. If the spleen qi and the healthy qi are insufficient,the pathogenic qi will take advantage of the deficiency to enter into the body, and the accumulative diseases in the viscera such as colorectal cancer are easy to form; if the engendering transformation source of qi and blood is weak, the whole body and the five Zang and six Fu organs cannot be nurtured, showing fatigue, drowsiness, and weakness of limbs, which cannot be relieved after rest[15].Kidney is the foundation of the innate, which stores essence, receives qi and controls yin and yang in the whole body. Insufficient kidney essence, primordial yin and yang will cause deficiency of Zang-fu organs,manifested as fatigue, forgetfulness, poor sleep, etc.Moreover, kidney governs water, and thus the water will not flow well due to kidney deficiency. This will result in gathering dampness into phlegm, and blocking the qi movement in ascending and descending, thus to cause fatigue[16]. It can be seen that the deficiency of spleen and kidney is the basic pathogenesis of CRF, and the deficiency of spleen and kidney yang is more common.Long-term accumulation of cancer toxins and deeply involved pathogenic qi damage the healthy qi and attack the primordial yang. This will cause spleen and kidney yang deficiency, failure to warm, water-dampness accumulation, and depletion of yang qi, which further aggravate spleen and kidney yang deficiency, resulting in losing warmness in five Zang and six Fu organs, and the whole body.
Mild moxibustion has the effects of warming meridians and dredging collaterals, warming yang and replenishing qi, activating blood circulation and promoting qi flow, which can strengthen vital qi to eliminate pathogenic factors, regulate qi, blood and yin and yang, and can be used to treat CRF[17]. Among the acupoints used for moxibustion, Shenque (CV 8) has the functions of warming yang and reinforcing qi,invigorating spleen and kidney, opening orifices and refreshing mental activity; meanwhile, Shenque (CV 8) is adjacent to the stomach and intestines with the major indication of spleen and stomach disorders. Guanyuan(CV 4) is the Front-Mu point of small intestine, and has the effect of invigorating the kidney and strengthening the roots with the main indication of kidney-yang, and Zang-fu organs deficiency. Zusanli (ST 36) is the He-Sea point of the Stomach Meridian and the Lower He-Sea point of stomach, which can invigorate the spleen and stomach, replenish qi and blood, and regulate qi movement, and is a key acupoint for invigorating deficiency and health care. Pishu (BL 20) and Shenshu(BL 23) are the Back-Shu points of the spleen and kidney respectively, and the main acupoints for the treatment of spleen and kidney diseases; meanwhile, both of them are the meridian acupoints in the Bladder Meridian.Therefore, moxibustion at Pishu (BL 20) and Shenshu(BL 23) is particularly effective in warming the spleen and kidney. The above acupoints are combined to strengthen spleen and reinforce kidney, reinforce qi and warm yang,improve the deficiency and strengthen the foundation.In this study, after treatment, total score of PFS-R in the control group did not change significantly (P>0.05), but it was significantly reduced in the observation group(P<0.05) and lower than that in the control group(P<0.05); KPS scores of both groups were increased (bothP<0.05), and significantly higher in the observation group than in the control group (P<0.05); the total score of spleen and kidney yang deficiency syndrome in the control group did not change significantly (P>0.05), but it was significantly reduced in the observation group(P<0.05) and lower than that in the control group(P<0.05). This indicates that mild moxibustion can relieve the fatigue of patients undergoing chemotherapy after colorectal tumor surgery, improve quality of life, and improve the symptoms of spleen-kidney yang deficiency.
This study also observed the changes in serum Ghrelin and adiponectin levels of patients in the two groups.Ghrelin can stimulate appetite and increase eating,promote gastrointestinal motility, increase gastric acid secretion, protect mucosa of the digestive tract, promote the digestion and absorption of nutrients, regulate the body's energy metabolism, and increase weight; it can also inhibit the activity of calpain, promote the phosphorylation of protein kinase B in skeletal muscle,reduce the expression of muscle atrophy F-box(MAFbx/atrogin-1), reduce muscle protein degradation,and inhibit skeletal muscle atrophy[18]; it can also reduce the levels of serum tumor necrosis factor, interleukin and other cytokines, inhibit myotube cell atrophy, protect skeletal muscle, and regulate the function of the hypothalamus-pituitary-adrenal axis to improve fatigue symptoms[19]. Adiponectin is a biologically active polypeptide secreted by adipocytes, which can increase fatty acid oxidation and sugar absorption in skeletal muscle cells, and increase insulin gluconeogenesis;similar to ghrelin, adiponectin can also inhibit the expression of tumor necrosis factor and exert antiinflammatory and anti-tumor effects[20]. Therefore,regulating the ghrelin and adiponectin levels may be potential targets for the treatment of CRF. In this study,after treatment, the serum ghrelin and adiponectin levels in the control group did not change significantly(bothP>0.05), but they were significantly increased in the observation group (bothP<0.05) and higher than those in the control group (bothP<0.05). This indicates that mild moxibustion can significantly increase the serum ghrelin and adiponectin levels in the patients,which may be one of the possible mechanisms in mild moxibustion treatment of CRF.
In summary, mild moxibustion can relieve the fatigue in patients undergoing chemotherapy after colorectal tumor surgery, improve the quality of life, and improve the symptoms of spleen and kidney yang deficiency,which may be related to the regulation of serum Ghrelin and adiponectin levels. The limitations of this study included a small case number, single-center patient source, and failure to conduct long-term follow-up of CRF symptoms and quality of life. These need to be improved in the future studies to provide a more reliable basis for the clinical application of mild moxibustion.
Conflict of Interest
There is no potential conflict of interest in this article.
Acknowledgments
There was no project-fund supporting for this study.
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 30 March 2020/Accepted: 9 July 2020
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Assessment of the safety and efficacy of acupuncture in erectile dysfunction treatment
- Clinical observation of heat-sensitive moxibustion for acute ischemic stroke
- Efficacy observation of Zhi Shen Tiao Sui acupuncture method for depression after ischemic stroke
- Clinical observation on acupoint pressure plus longsnake moxibustion for upper-limb spastic hemiplegia after cerebral infarction
- Clinical efficacy observation of acupoint threadembedding in treating obese patients with food addiction
- Effects of acupuncture plus spinal manipulations on physical functioning and biochemical indicators in patients with ankylosing spondylitis