BRCA mutation rate and characteristics of prostate tumor in breast and ovarian cancer families: analysis of 6,591 Italian pedigrees
2021-06-19LauraCortesiFedericaDomatiAnnalisaGuidaIsabellaMarchiAngelaTossElenaBarbieriLuigiMarcheselliMartaVenturelliSimonettaPianaClaudiaCirilliMassimoFederico
Laura Cortesi, Federica Domati, Annalisa Guida, Isabella Marchi, Angela Toss, Elena Barbieri,Luigi Marcheselli, Marta Venturelli, Simonetta Piana, Claudia Cirilli, Massimo Federico
1Department of Oncology and Hematology, University Hospital of Modena, Modena 41124, Italy; 2Department of Medical and Surgical Sciences for Children & Adults, Division of Medical Oncology, University Hospital of Modena, Modena 41124,Italy; 3Pathology Unit, Azienda USL Reggio Emilia, IRCCS, Reggio Emilia 42123, Italy; 4Modena Cancer Registry, Public Health Department, AUSL Modena 41126, Italy
ABSTRACT Objective: As prostate cancer (PrC) shows a BRCA mutation rate as high as 30%, it becomes crucial to find the optimal selection criteria for genetic testing. The primary objective of this study was to evaluate the BRCA mutation rate in families with PrC associated with breast and/or ovarian cancers; secondary aims were to compare the characteristics of families and BRCA-related PrC outcome among BRCA1 and BRCA2 carriers.
KEYWORDS BRCA genes; prostate cancer; hereditary cancer; Modena criteria; breast cancer; ovarian cancer
Introduction
Prostate cancer (PrC) is the most common malignancy among males representing 7.1% of all cancers and a mortality rate of 3.8% in men1. In Italy the 5-year survival rate for men with PrC is 92% and the 10-year survival rate is 90%2. The etiology of PrC has been the subject of numerous studies and remains largely unknown compared to other common cancers. The well-established PrC risk factors are advanced age, ethnicity, genetic factors, and family history3.Other factors associated with PrC include diet (increased consumption of saturated animal fat and red meat, lower intake of fruit, vegetables, vitamins, and coffee), obesity and physical inactivity, inflammation, hyperglycemia, infections,and environmental exposure to chemicals or ionizing radiation. However, an increasing number of elderly men are being diagnosed with PrC due to increased life expectancy and increased prostate specific antigen (PSA) screening. It has also been observed that the risk of PrC mainly increases in Caucasian males over 50 years of age who have no PrC family history, and in Black males over 40 years of age or men with a familial history of PrC4. The disease appears to be linked to hereditary factors in a minority of cases (≤30%)5.BRCA1andBRCA2genes in prostate tumorigenesis have been associated with more aggressive disease and poor clinical outcomes. The estimated lifetime risk is 9.5%forBRCA1and 20% forBRCA2mutation carriers6. Overall,BRCA1/2mutation carriers present an increased risk for breast cancer (BC) (52%-72% in BRCA1, 45%-84% inBRCA2), ovarian cancer (OC) (39%-63% in BRCA1, 11%-27% in BRCA2), PrC (3.4-fold increased risk in BRCA1,8.6-fold increased risk in BRCA2), and pancreatic cancer(PC) (1%-3% in BRCA1, 2%-7% in BRCA2)7-11. The identification of a mutation inBRCAgenes plays a crucial role in the management of hereditary cancer prevention, diagnosis, and treatment. According to the guidelines of the Italian Association of Medical Oncology (AIOM), which reflect the Modena criteria12-14listed in Table 1, the Italian National Health Service provides free BRCA diagnostic tests exclusively for breast, ovarian and pancreatic cancer patients, and to healthy individuals with an estimated risk of carrying aBRCAmutation ≥ 40%. This large, single-institution cohort study sought to firstly evaluate the rate of BRCA-positive families among those presenting a family history of PrC associated with BC and/or OC selected by Modena criteria and secondly, to explore family history and outcomes of BRCA-related PrCs.

Table 1 The Modena Criteria (AIOM Guidelines 2019)
Materials and methods
Study population and design
The human investigations were reviewed and approved by the Modena Human Investigations Committee (Approval No. 209/16/3387). The patients provided their written informed consent to participate in this study.
Patients with a family history of BC and/or OC who received genetic counseling for risk category classification and theBRCAtest at the Modena Family Cancer Clinic (MFCC)from 1991, were eligible for the purpose of this analysis.Probands affected with BC or OC who met the Modena criteria for genetic testing could undergo the BRCA analysis and in the case of a positive result, could ease cascade analysis thus favoring access to risk-reducing surgeries, chemo-preventive studies, or more intensive surveillance programs. Family history that included PrC with Gleason score ≥ 7 in a first- or second-degree relative (in the case of female interposition) of BC or OC, were evaluated for this analysis.
A retrospective medical record review of the pedigrees with a Gleason score ≥ 7 PrCs, previously collected during genetic counseling visits, was completed for the present study.
BRCA testing procedures
Before 2014, genetic testing ofBRCA1andBRCA2genes at our institution was carried out by direct Sanger sequencing, whilst after 2014, genetic testing was performed using next generation sequencing (NGS). The NGS workflow benefits from the use of the Ion AmpliSeq TM (Thermo Fisher Scientific, Waltham, MA, USA) technology that was handled initially with a semi-automated and subsequently, with a fully automated procedure for multiplex polymerase chain reaction (PCR)-based library preparation sequencing on the Ion Torrent platforms (Thermo Fisher Scientific, Waltham, MA,USA). More recently a Multigene Panel Testing provided by MySeq Dx System (Illumina, San Diego, CA, USA), comprising 27 hereditary syndrome genes, was used. Sanger sequencing was routinely performed to validate candidate mutations, as long as multiplex ligation probe amplification (MLPA, MRCHolland, Amsterdam, The Netherlands) was carried out on a blood sample to detect copy number variations in all genes,exceptBARD1,BRIP1, andNBN. Sequence alignment, base calling, variant filtering, and annotation process took advantage of the Torrent Software Suite (Thermo Scientific) and of a custom designed bio-informatic pipeline, as described in previously published works15,16. Pathogenicity was defined as categories 4 (likely pathogenic) and 5 (pathogenic) of the ENIGMA classification17. Classes C3 (unclassified variants),C2 (probably benign), or C1 (benign) were not reported.
Statistical analysis and outcome measures
A database was set up at our health center, which consisted in collecting family and individual information, surveillance and follow-up data, additional investigation, and the outcome of all examinations. The reports of these families included test results (if performed), age at cancer onset, histology, relation to the proband, vital status, and type of other cancers. We calculated the median follow-up of the proband in the period from 1991 to 2019. The PrC follow-up was calculated from the date of cancer onset to the endpoint of interest: the date of death or the end of the study period. The chi-square (χ2)test was used to determine differences in clinicopathological features between groups. All statistical tests were two-sided.Survival curves were estimated using the Kaplan-Meier method including the log-rank test group comparison.
Results
BRCA mutation rate
From March 1991 to August 2019, 6,591 families with history of BC and/or OC, were counseled and used as the reference population by the MFCC. Seven hundred and seventy-five(11.7%) families reported a family history of associated PrC. Among those PrCs, 580 (74.8%) had a Gleason score≥ 7. According to the 2019 Modena criteria, 332 (57.2%) of these families were eligible for BRCA testing. In total, 215 probands affected with BC or OC were tested (64.8%), mostly with BC (203) and 12 with OC. The remaining patients were not tested because they refused to or were unable to undergo genetic analysis due to poor health conditions or because patients were not in close proximity to the medical center. Forty-one families were found to beBRCAmutation carriers and one family showed aCHEK2mutation defined c.1100delC, typically associated with PrC (19.5%). Among theBRCAmutated patients, 18 wereBRCA1positive (43.9%)and 23 wereBRCA2mutated families (56.1%). We inferred thatBRCAmutations were also found in PrCs, without testing any prostate cancer case. The diagram of patient selection is represented in Figure 1.
Family characteristics and patient outcomes
The mean age of PrC onset in all population was 68.3 years(range 21-90 years of age), with the lowest age in theBRCA2carriers (63.2 years) compared withBRCA1carriers (67.9 years) (P= 0.84). In the BRCA1 and BRCA2 groups, four(22.2%) and nine (39.1%) families showed two or more PrC cases, respectively, compared with 99 (18.4%) multiple PrCs found in other families (P= 0.195). In Table 2 the characteristics of mutated BRCA and not families are described. The stomach and melanoma tumor rates were increased inBRCA2mutation carriersvs BRCA1carriers (P= 0.136 andP= 0.347,respectively). However, no statistically significant differences were seen among all three populations with regard to other associated tumors. The onlyCHEK2mutation shown was described in a family with PrC, BC and bladder cancer.
After 240 months of follow-up, the median overall survival of PrC, evaluated from diagnosis to date of death or last follow-up, was equal to 65 months in a non-tested group of patients, 62 months in patients with BRCA1-related PrC and 40 months in PrC-related BRCA2 patients (P= 0.265) (Figure 2).
BRCA pathogenic variants and prostate cancer risk
BRCAmutations detected in families with history of PrC are reported in Figure 3A and Figure 3B. Eleven of 18 (61%)BRCA1mutations were located on exon 10. On the other hand, 10 of 23 (44%) mutations in theBRCA2gene fell in the prostate cancer cluster region (PCCR) at the 3′ terminal of the 7914 codon. Finally, the most commonBRCA1mutation types were frame-shift mutations (11 of 18, 61%), followed by missense mutations (7 of 18, 39%). In theBRCA2gene, the most frequent mutations were similarly frame-shift mutations (12 of 23, 52%).
Discussion

Figure 1 The flow-chart of families evaluated and tested at the MFCC.
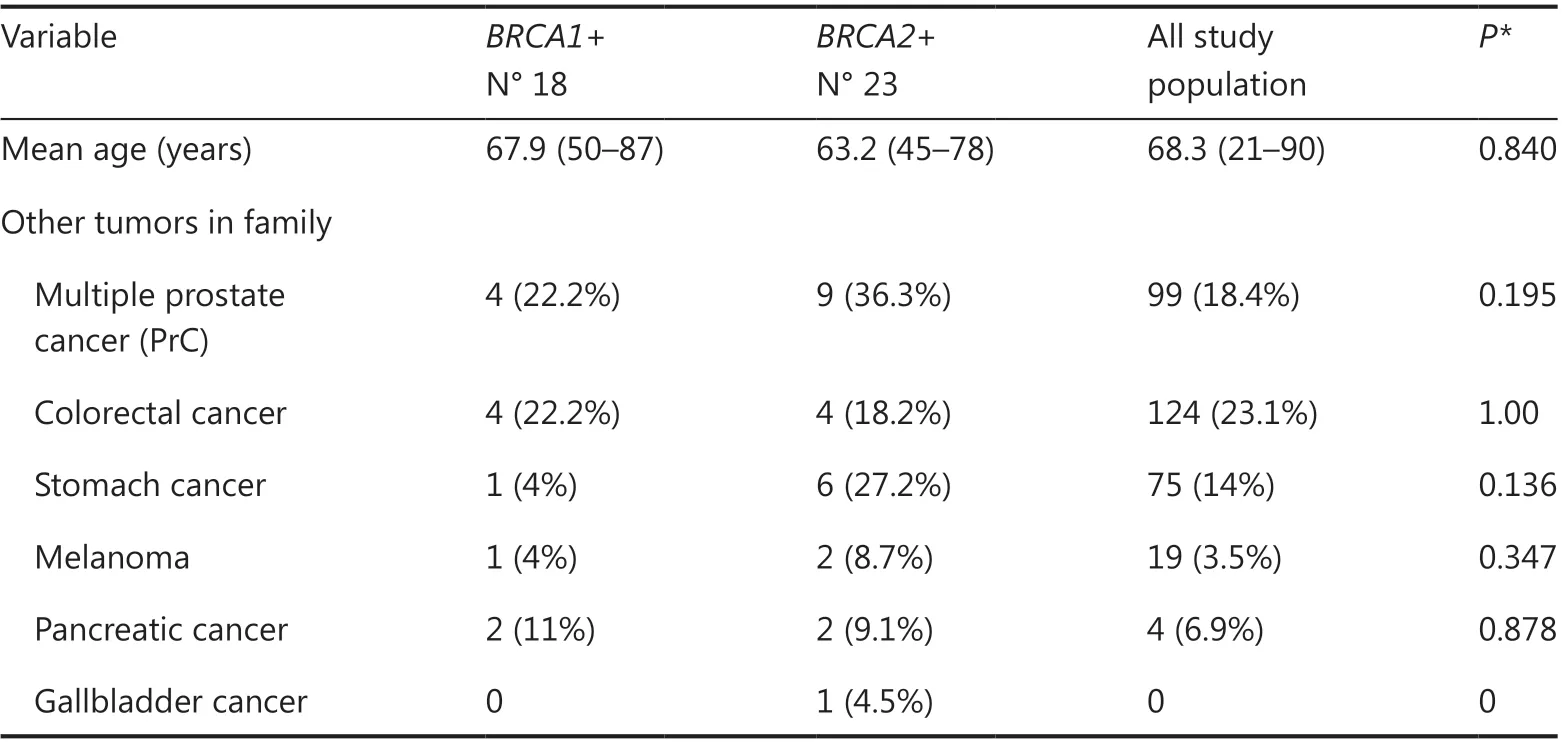
Table 2 Characteristics of family history
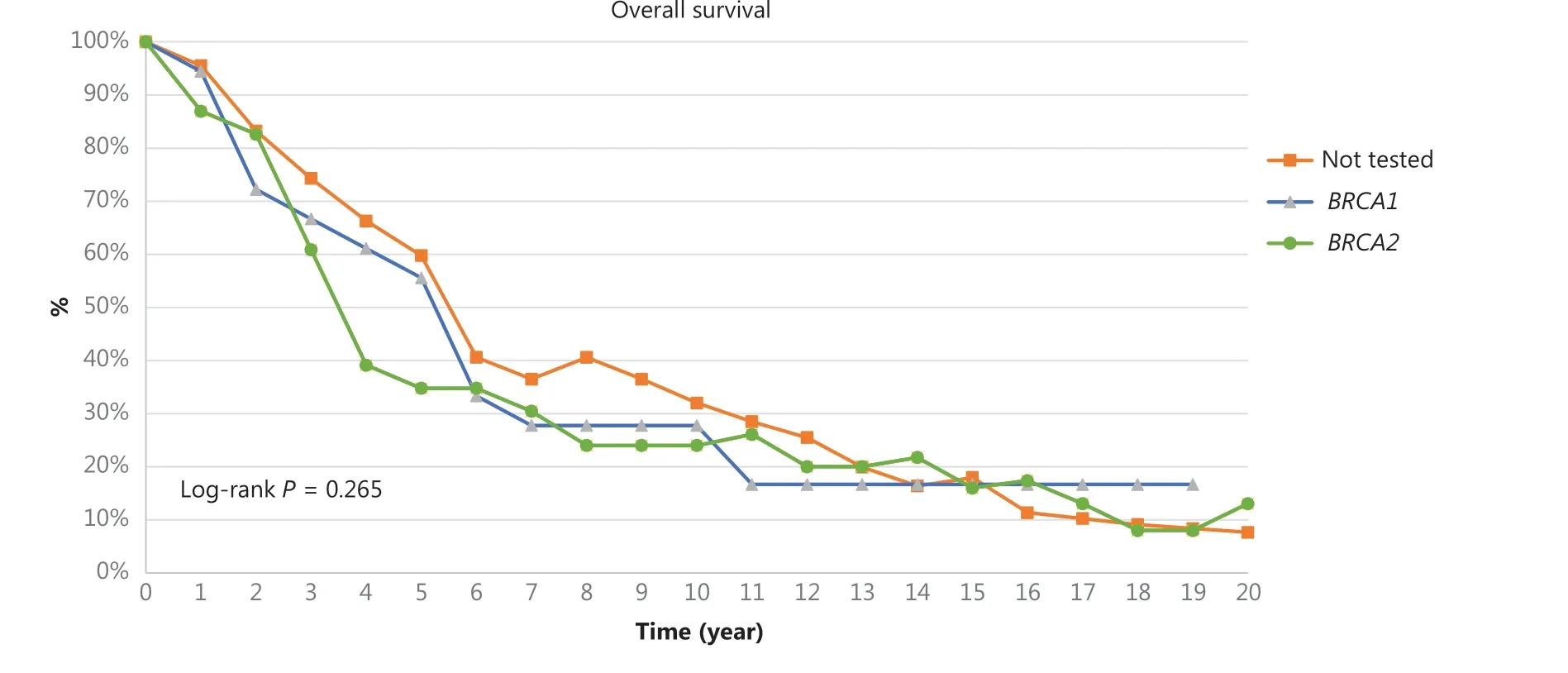
Figure 2 Overall Survival of PrC at 240 months of median follow-up. The log-rank test between non-tested (orange line) and BRCA1 mutation carriers (blue line) is equal to P = 0.911; the log-rank test between non-tested (orange line) vs BRCA2 mutation carriers (green line) is equal to P = 0.265; the log-rank test between BRCA1 mutation carriers (blue line) and BRCA2 mutation carriers (green line) is equal to P =0.575.

Figure 3 Distribution of mutations along BRCA1 (A) and BRCA2 (B) genes. Mutations detected more than once are represented in bold characters.
Approximately 7%-8% of all patients with PrC has an underlying gene defect on theBRCA1,BRCA2, andCHEK2genes5.Furthermore, a recent population study performed on Scandinavian twins, shows a very high rate of hereditary PrC conditions, reaching a high of 57%18. Particularly, theHOXB13gene has been associated with early onset of PrC in 6% of cases19.Moreover, data on positive family history for PrC show a high rate of first-degree relationship for this type of cancer (32.3%)20.It therefore becomes crucial to find the optimal selection criteria for genetic testing, with a positive ratio between cost and effectiveness, in order to ease cascade analysis of at-risk relatives and offer effective surveillance programs, based on annual PSA and prostatic ultrasound, that have recently demonstrated to increase the detection of early stage prostate tumors, particularly in case ofBRCA2mutation carriers21.
Patients selected according to the Modena criteria reached a 19.5% of mutations considering all the families eligible for the test, overcoming the probability rate of 10% to find a heterozygous mutation that justifies BRCA screening, as suggested in many countries in accordance with National Institute for Health and Care Excellence (NICE) guidelines22. Assuming that first-degree or second-degree (in case of female interposition) relatives with high grade PrC carry theBRCAmutation,it can be concluded that the Modena criteria should be introduced in clinical practice for PrC genetic testing. Furthermore,we think that the recent introduction of the multigene panel test could increase the rate of hereditary PrC by adding new genes to the BRCA analysis such as CHEK2, that is frequently associated with this kind of tumor, as was shown recently23.
Although no statistically significant differences were seen among BRCA-positive and non-tested families, a trend toward an increased number of PrC and stomach cancer cases was shown inBRCA2mutated families. These data are consistent with other previously published studies24,25.
Finally, our survival data seem to reflect a worse prognosis ofBRCA2carriers in comparison with BRCA1 and non-tested patients, although no statistically significant differences have been found. These results can be compared with data from Narod et al.26where the median survival for BRCA2 PrC was 4 years,vs8 years in BRCA1 patients.
Of particular concern, 44% ofBRCA2mutations were found in the PCCR region at the 3′ terminal of the 7914 codon,recently identified by Patel et al.27. It could therefore be useful to identify these mutations, as the risk of PrC in men carriers is high thus inducing us to intensify prostate surveillance programs starting at an earlier age and including other imaging diagnostic tools such as multiparametric magnetic resonance imaging (MRI).
Even though there are some limitations to our retrospective analysis it should be noted that in this study, the BRCA test was performed on patients affected by BC or OC and the positive result was transferred on patients affected by PrC along the genealogy in which the hereditary transmission was found. As most PrC patients were not alive at the time of genetic counseling, it was not possible to verify which PrC patients in BRCA positive families wereBRCAcarriers.
Therefore, a bias may have occurred, as there is a chance,that some cancer cases and their outcome, were notBRCAcarriers, being phenocopies inBRCAmutated families. The high percentage of BRCA1 as compared to BRCA2 is not typical from most PrC series and may reflect biases based on this study population. Furthermore, we are well aware that a bias may have occurred, as only 215 families were tested.
In order to improve our data, we are currently evaluating the possibility to perform a prospective study in which the BRCA test is carried out on PrC tissue thus enabling us to also include deceased patients in future analysis.
In conclusion, our analysis found that Italian criteria are very effective to detectBRCA1orBRCA2mutations in PrC and should be taken into consideration when deciding upon testing. Data on family history and PrC outcomes inBRCA2mutation carriers show an increased number of multiple PrC and stomach cancers and a worse prognosis, as compared with previously published results. Finally, as 44% ofBRCA2mutations were found in the PCCR region at the 3′ terminal of the 7914 codon, we believe such a variant in healthy men could be useful to intensify a prostate surveillance program at earlier age including the use of multiparametric MRI.
Acknowledgments
We would like to thank and express our gratitude to Tamara Sassi and Johanna Chester for their editorial assistance and we gratefully acknowledge the support received from Associazione Angela Serra per la Ricerca sul Cancro, Angela Serra Cancer Research Association, Modena, Italy towards Dr. Angela Toss’PhD.
Conflict of interest statement
Laura Cortesi holds an honoraria from AstraZeneca, MSD,Pfizer and a consulting or advisory role at Pfizer, Novartis,Tesaro and Clovis. Angela Toss holds a consulting or advisory role at Lilly and Novartis.
杂志排行

Cancer Biology & Medicine的其它文章
- Circular RNAs: new biomarkers of chemoresistance in cancer
- Biological roles and potential clinical values of circular RNAs in gastrointestinal malignancies
- Biomaterial-based platforms for cancer stem cell enrichment and study
- sLex expression in invasive micropapillary breast carcinoma is associated with poor prognosis and can be combined with MUC1/EMA as a supplementary diagnostic indicator
- Nanomaterial-based delivery vehicles for therapeutic cancer vaccine development
- Targeting FGFR in non-small cell lung cancer: implications from the landscape of clinically actionable aberrations of FGFR kinases