Arthroereisis in juvenile flexible flatfoot: Which device should we implant? A systematic review of literature published in the last 5 years
2021-06-18AndreaVescioGianlucaTestaMirkoAmicoClaudioLizzioMarcoSapienzaPieroPavoneVitoPavone
Andrea Vescio, Gianluca Testa, Mirko Amico, Claudio Lizzio, Marco Sapienza, Piero Pavone, Vito Pavone
Andrea Vescio, Gianluca Testa, Mirko Amico, Claudio Lizzio, Marco Sapienza, Vito Pavone, Department of General Surgery and Medical Surgical Specialties, Section of Orthopedics and Traumatology, University Hospital Policlinico-San Marco, University of Catania, Catania 95123, Italy
Piero Pavone, Department of Clinical and Experimental Medicine, Section of Pediatrics and Child Neuropsychiatry, University of Catania, Catania 95123, Italy
Abstract BACKGROUND Flexible flatfoot (FFF) is a very common condition in children, characterized by the loss of the medial arch and by an increase in the support base with valgus of the hindfoot.Arthroereisis (AR) procedures are widely performed corrective surgeries and are classified as subtalar AR and calcaneo-stop (CS).AIM We investigated the literature published in the last 5 years with the aim of providing an update on the evidence related to AR treatment in FFF patients.We report the principal findings of subtalar AR and CS procedures concerning clinical and radiological outcomes and complication rates in the general population, young athletes, and obese people according to material device.METHODS Following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, a systematic review of studies published in the past 5 years and included the PubMed and Science Direct databases was performed on May 6, 2020.The research string used was (pediatric OR children OR Juvenile NOT adult) AND (flexible NOT rigid) AND (flat foot OR pes planus) AND (calcaneo-Stop OR arthroereisis OR subtalar extra-articular screw OR SESA OR subtalar arthroereisis OR endosinotarsal).The risk of bias assessment was performed using the Dutch checklist form for prognosis.RESULTS A total of 47 articles were found.Ultimately, after reading the full text and checking reference lists, we selected 17 articles that met the inclusion and exclusion criteria.A total of 1864 FFFs were identified.Eight studies concerned the subtalar AR (47.1%) and nine concerning CS (52.9%).The average age of patients at start of treatment was 11.8 years, the average follow-up of the studies was 71.9 mo (range 29.1-130).Globally, complications occurred in 153 of the 1864 FFF treated, with a rate of 8.2%.CONCLUSION Both AR procedures are valid surgical techniques for treating FFF.Surgeon experience, implant cost, and cosmetic correction are the most common considerations included in the orthopedic device decision-making process.In obese patients, the subtalar AR is not recommended.In adolescents who need to improve sports performance, the CS screw had better results compared with other implants.
Key Words: Pes planus; Arthroereisis; Treatment; Calcaneo-stop; Subtalar arthroereisis; Complication
INTRODUCTION
Flexible flatfoot (FFF) is a very common condition in children[1] characterized by loss of the medial arch and increases of both heel valgus and plantar pressure[1].FFF is typically an asymptomatic condition, but pain may occur in the lower leg or medial level of the foot at the insertion point of the posterior tibial on the scaphoid, especially after intense exercise or long walks[2].In some cases, early and easy fatigue can occur and are consider important symptoms[3].Surgical treatment is indicated in symptomatic children over 8 years of age or not responsive to conservative treatment.Arthroereisis (AR) procedures are common corrective surgeries that are widely performed.AR was first introduced in 1946 by Chambers[4], who described the “abduction block,” as a wedge-shaped bone block aimed to impact the anterior border of the posterior facet of the calcaneus and to limit excessive anterior displacement of the talus on the calcaneus and correct the deformity.
The first author to introduce the term “arthroereisis” was Lelièvre[5] in the early 70s to illustrate a temporary staple across the subtalar joint.In 1979, the Buruturan[6] impact blocking screw, which was inserted into the calcaneus using the sinus tarsi as the entry point, is the first description of a calcaneo-stop (CS) procedure.In 1992, Viladot[7] reported the success rate achieved by the first non-osseous sinus tarsi implant.The aim of implants is to correct the FFF deformity with preservation of foot function and limitation of excessive anterior displacement of the talus upon the calcaneus[8].Moreover, some authors[9,10] have hypothesized that CS could play a role in the activation of mechanoreceptors in the sinus tarsi, although it has not yet been supported by experimental evidence.Subtalar implants are classified by type as impact blocking devices, which include subtalar AR; and self-locking implants, which include CS screws[11].Impact blocking devices have a stem that is fixed in the sinus tarsi vertically just anteriorly to the posterior subtalar surface and a head, that interferes with the talar lateral process, limiting its internal rotation.Self-locking implants are inserted in the sinus tarsi along its main axis, supporting the talar neck, avoiding contact between talar lateral process and sinus tarsi floor, and reducing talar adduction and plantar flexion.
The aim of the study was to review the literature of the last 5 years regarding the surgical treatment of juvenile FFF with a focus on the AR procedures and to report the principal subtalar AR and CS procedure findings concerning clinical and radiological outcomes and complication rate in general population, young athletes and obese population according to the device.
MATERIALS AND METHODS
Study design
A systematic review of studies published in the last 5 years.Clinical outcomes and radiological measurements, Athletes and Obese cohorts’ outcomes, Complications, Materials of subtalar AR and CS were recorded.
Search strategy
A systematic review of studies published in the last 5 years and indexed in PubMed and Science Direct was performed by an author (Vescio A) on May 6, 2020.The research string used was “(pediatric OR children OR Juvenile NOT adult) AND (flexible NOT rigid) AND (flat foot OR pes planus) AND (calcaneo-stop OR arthroereisis OR SESA OR subtalar arthroereisis OR s OR subtalar extra-articular screw)”.
Study selection and inclusion criteria
Eligible studies for this systematic review included FFF treatment and AR.The titles and abstracts were screened, using the following inclusion criteria: treatment consisted of AR with or without additional soft tissue procedures, operative treatment, or cast application, and a minimum average follow-up of 6 mo in patients between 7 and 17 years of age.Studies of patients with secondary, including syndromic and neurological FFF, nonoperative treatment or lateral column lengthening (LCL), or medializing calcaneal osteotomy duplicate publications, articles dealing with other topics, those with poor scientific methodology or without an accessible abstract were excluded.Reference lists were also hand-searched for further relevant studies.Systematic reviews, Meta-analyses, abstracts, case reports, conference presentations, editorials, and expert opinions were excluded.
Data extraction and quality assessment
Two subtalar implant types were considered, impact blocking devices and self-locking implants[13].The risk of bias assessment was performed independently by two authors (Vescio A and Amico M) using the Dutch checklist form for prognosis recommended by the Cochrane Collaboration[13].Conflicts about data were resolved by consultation with a senior surgeon (Pavone V).Table 1 presents a risk of bias summary including checklist items with low risk (+), high risk (-), or unclear risk (?).The forms were compared and discussed for final consensus (Table 2).
Evidence synthesis
For each included article, a standard data entry form was used to extract the number of patients, number of feet treated, affected side, sex, patient age when treated, type of procedure with or without additional surgeries, number of successes and failures, period of the study, and implant materials.We considered improvement of the medial arch, hindfoot valgus, radiological evaluation, pedobarographic measurements, and functional outcome as indicators of treatment success.The assessment included: (1) The American Orthopedic Foot and Ankle Society (AOFAS) Ankle–Hindfoot score; (2) The Oxford Ankle Foot Questionnaire for Children; (3) The Foot and Ankle Disability Index (FADI); (4) FADI Sport scores; (5) The Foot Function Index Questionnaire; (6) The self-reported Foot and Ankle Score; and (7) Visual Analogue Score.Major and minor complications included screw device loosening, transient pain and discomfort at the level of the surgical incision, contracture of the lateral peroneal muscles, and superficial infection.
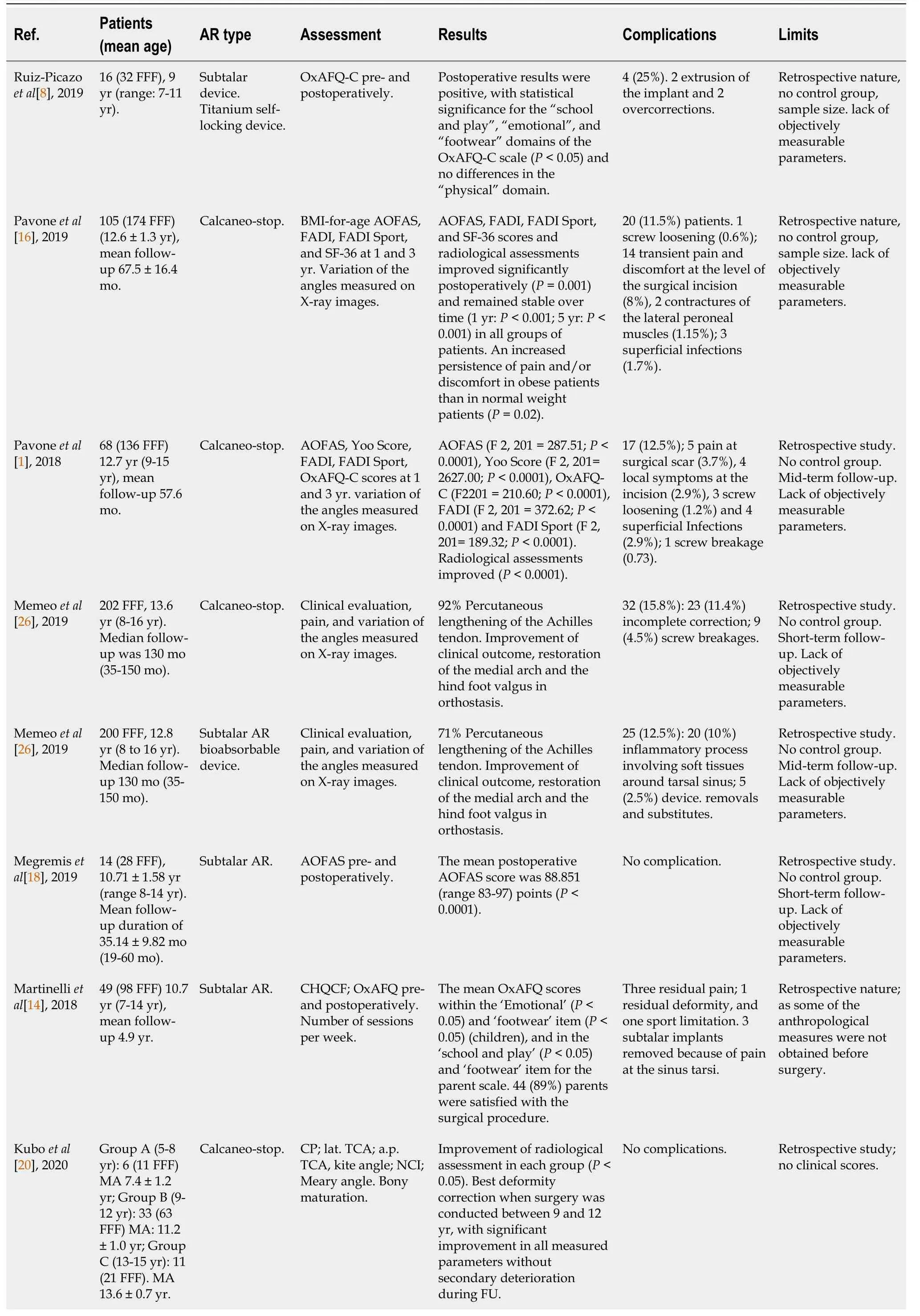
Table 1 Study results
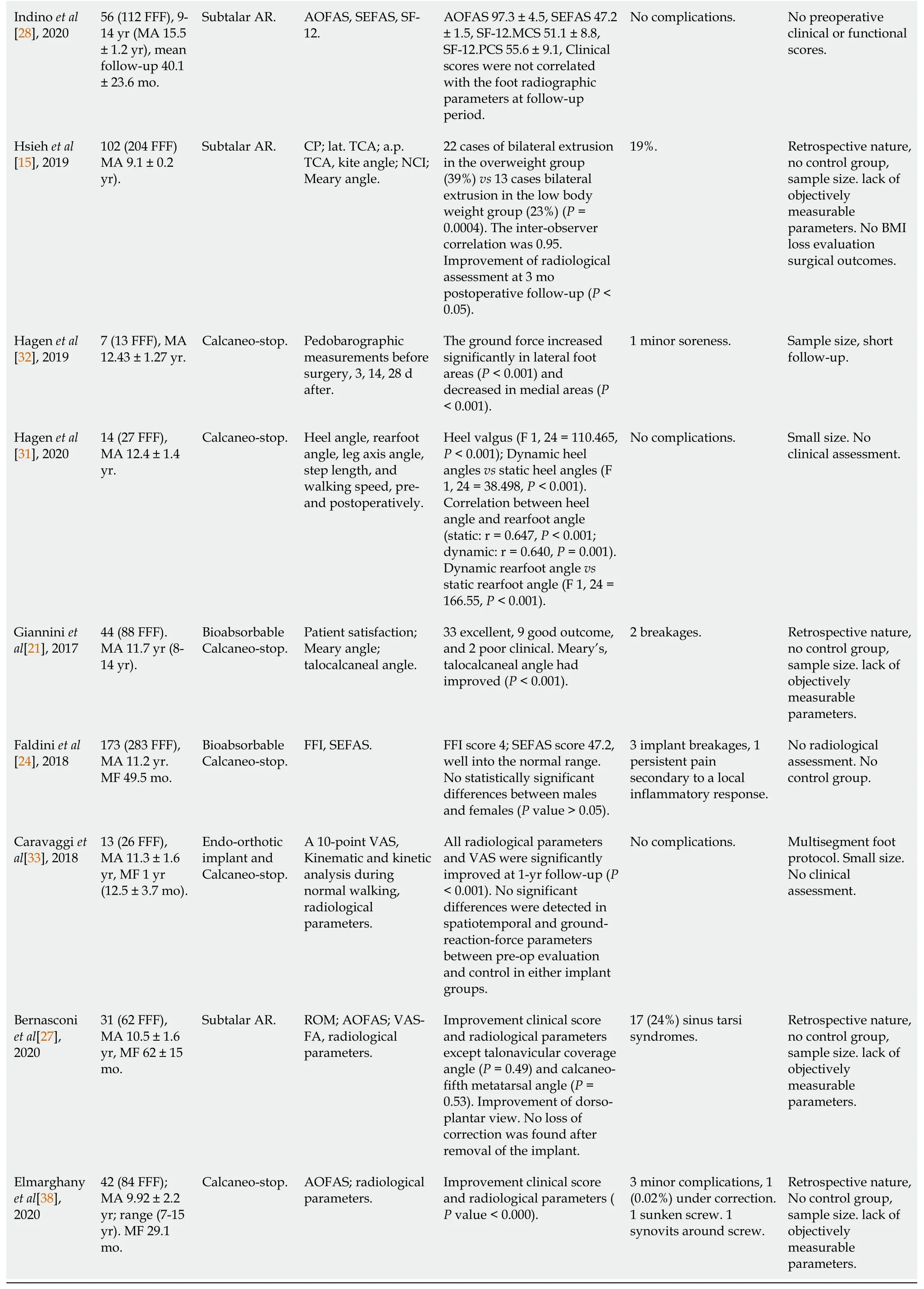
AOFAS: American Orthopedic Foot and Ankle Society; AR: Arthroereisis; FADI: Foot and Ankle Disability Index; FFF: Flexible flatfoot; FFI: Foot Function Index Questionnaire; MA: Mean age; MF: Mean follow-up; OxAFQ-C: Oxford Ankle Foot Questionnaire for Children; ROM: Range of motion; SEFAS: Self-reported Foot and Ankle Score; VAS: Visual Analogue score.
RESULTS
Study selection
A total of 47 articles were retrieved, 34 duplicate publications were excluded, and after the first screening following the previously described selection criteria, 22 were eligible for full-text evaluation.After full-text evaluation, and reference list checking, we selected 17 articles for inclusion (Table 1).The Preferred Reporting Items for Systematic Reviews and Meta-Anal (PRISMA)[12] flowchart of selection and screening is shown in Figure 1.A total of 1864 FFFs were treated In the 17 studies.Eight (762 FFFs) evaluated subtalar AR (47.1%) and nine (1102 FFFs) evaluated CS devices (52.9%).At start of treatment, the average age of patients was 11.8 years, the average follow-up was 71.9 mo (range 29.1-130), and complications occurred in 153 of the 1864 FFF treated, a rate of 8.2% (Table 1).
Clinical outcomes and radiological measurements
Eight studies evaluated subtalar AR in a total of 762 FFFs.The average age of patients at the start of treatment was 11.6 years (range 7 to 16 years) and the average follow-up of the studies was 68.9 mo.Every study reported statistically significant differences between pre- and postoperative assessments of pain, clinical scores, or parent and patient satisfaction (Pvalues of 0.001 to 0.05).Radiological measurements showed improvement in every trial (Pvalues of 0.001 to 0.05).
Nine articles evaluated CS in a total of 1102 FFFs.The average age of patients at the start of treatment was 12.0 years (range 7 to 17 years) and the average follow-up of the studies was 70.9 mo.As with subtalar AR Every study reported statistically significant differences between pre- and postoperative assessments of pain, clinical scores, or parent and patient satisfaction (Pvalues of 0.001 to 0.05).Radiological measurements showed improvement in every trial (Pvalues of 0.001 to 0.05).The clinical and radiological characteristics are summarized in Table 1.
Athlete and obese patient outcomes
Two articles investigated sport activities in FFF patients.In Martinelliet al[14]’s, 49 patients (98 FFFs) underwent to clinical and radiological evaluation after subtalar AR implant.Despite improvements in the emotional, school and play, and footwear (P< 0.05) items of the OxAFQ, the authors did not find any increase sport ability (P> 0.05).On the other hand, Pavoneet al[1].evaluated 68 CS-treated FFFs and reported improvement of sport activity levels, with patients recovering sports activity within 3 mo of surgery and without limitation in the execution of preferred activities (FADI Sport pre-vspostoperative scoresP< 0.005).
Two studies included obese patients.Hsiehet al[15] evaluated 102 (204 FFFs) subtalar AR-treated patients.The study outcome was radiological assessment at 3 mo postoperative follow-up.Significatively differences in implant bilateral extrusion (39%vs23%) were seen in overweight and normal weight patients, respectively,P= 0.0004).Obese patients treated with CS procedure reported a persistence of foot pain (AOFAS pain domainP< 0.05) at 1 year after the surgery compared with normal weight and overweight subjects[16].
Complications
Complications occurred in 74 of the 762 FFFs treated with subtalar AR 9.7% and 79 of 1102 FFFs treated with CS (7.2%).The complications in subtalar AR patients included tarsi pain in 40 patients, and under- or overcorrection in four patients.The complications in CS patients included incomplete correction of the deformity in 24 and transient pain or discomfort at the incision site in 20 patients.
Materials
Fourteen studies evaluated nonabsorbable implants, seven were CS studies, and seven were subtalar AR studies.Four investigated bioabsorbable implants, three CS screws and one subtalar AR).
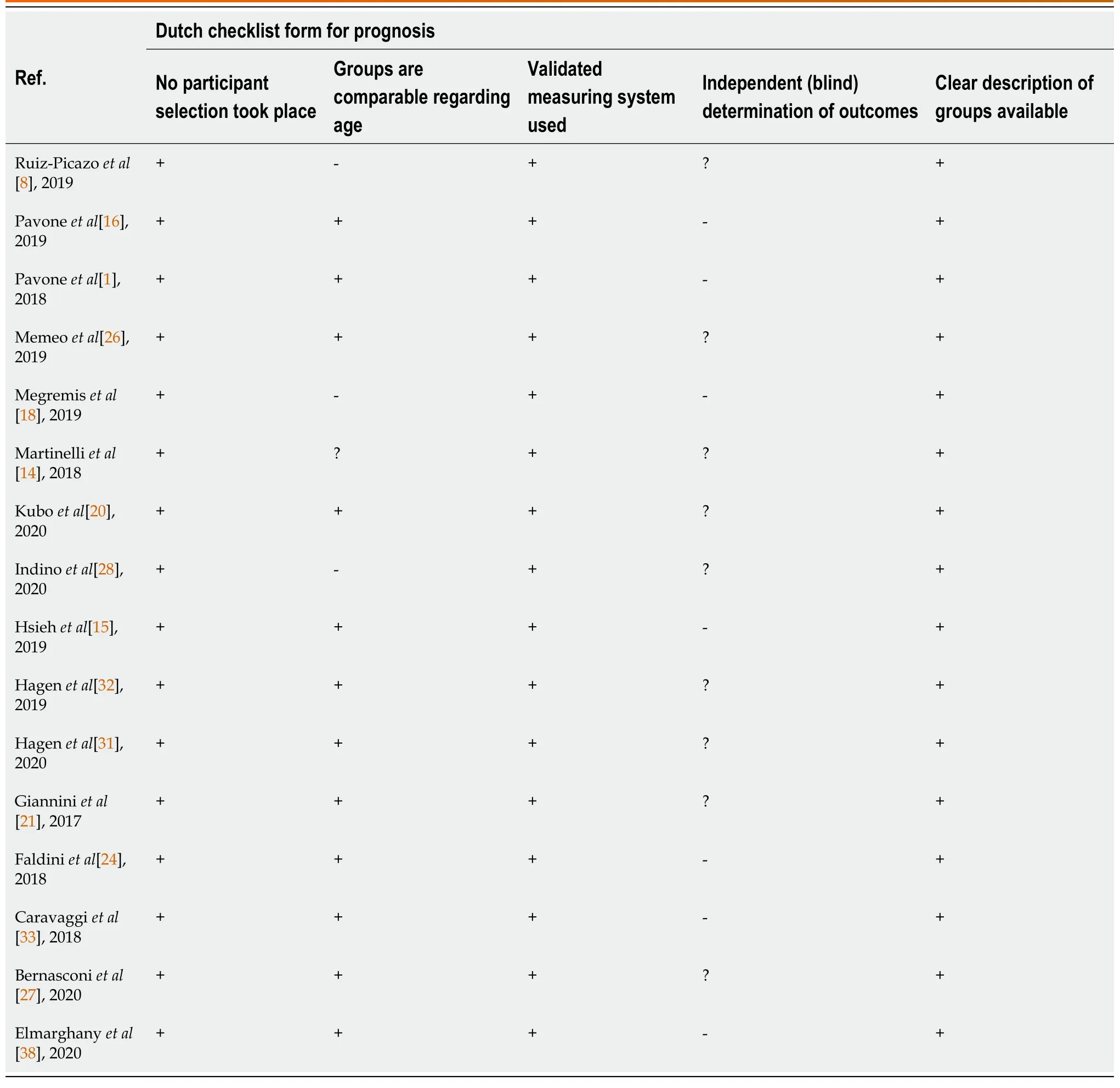
Table 2 Risk of bias of the included studies
DISCUSSION
AR procedures were found to simple, reliable, and minimally invasive interventions for the treatment of pediatric FFF, allowing the alignment of the talus and calcaneus and restoring a proper foot arch.Both implants improved clinical and radiological outcomes.Despite pain persistence for 1 year following CS treatment, subtalar selflocking is not recommended for obese patients.At the same time, an increase of sport activities was reported after CS implants but no differences were noted after subtalar implant procedures.Complications were reported in 153 of the 1864 FFFs that were treated.To the best of our knowledge, this is the first article investigating the outcomes of AR-treated patients reported in the past 5 years and analyzing CS procedures for impact blocking devices and subtalar AR self-locking implant results separately, including the technique-associated complications in specific populations.

Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of the systematic literature review.
The juvenile and adult surgical indications were not completely defined, and a common consensus was not present among orthopedic surgeons.The principal intervention parameters were age, symptoms including pain while walking or standing, postural fatigue, or cramping sensation in the foot or arch.Night cramps, lower back or knee pain, or sedentary preference may also be reasons for patients to seek medical intervention[16-28].In juvenile FFFs the most median age at treatment is 8 to 14 years of age, but only when the pain is persistent after conservative treatment[19].Kuboet al[20], considering bone maturation stage, found that the best deformity correction was achieved when surgically was performed between 9 and 12 years of age, without secondary deterioration during follow-up.
Every study included in this systematic review reported significative improvements of clinical and radiological assessments.Unfortunately, few articles[24,29,30], comparing the self-locking and impact blocking devices, were published in the last 5 years.The articles did not clearly report the exact indication for the implant choice or if the procedures were all performed by the same surgeon.Nevertheless, subtalar AR and CS techniques were found to be similar.Hagenet al[31,32] described an increased ground force in lateral foot areas, a decrease in medial areas, and a correlation between heel angle and rearfoot angle.On the other hand, in Caravaggiet al[33] did not find significant differences in spatiotemporal and ground-reaction-force between preoperative evaluation and postoperative control achieved in either implant group.
The findings related to the return to sport activities after AR implant differed.Patients who underwent CS had improved levels of sport activities without any notable limitation in physical activity[16].No enhancement of sport activities was found in a subtalar AR study[14].Pavoneet al[16] hypothesized better body awareness, removal of the impact of minor deformity on function, less FFF-related embarrassment, and the possibility of socializing through sport could have influenced the emotional involvement of CS-treated patients in social interactions.Emotional status was improved in patients with subtalar self-locking devices, but improvement of sport activities was not seen.
Obesity has long been considered a contraindication to AR implant because of excessive stress on the implant[20].Two studies aimed to investigate the functional and radiological outcomes in overweight and obese patients.Pavoneet al[16] reported improvement of clinical and radiological assessments following treatment with CS procedures, even in heavy subjects, despite the persistence of pain for 1 year, compared to nonobese children.The discomfort could be related to the overload of foot structures[16], increased foot pressure with higher peak pressure, and peak force under the midfoot and metatarsal regions[25] during walking and inactivity, which delay the resolution of symptoms in obese children.On the other hand, Hsiehet al[15] noted that subtalar self-blocking implants in overweight patients had an increased possibility of implant extrusion, especially while walking.
Furthermore, a high percentage of satisfaction (78.5%vs96.4%)[34] with AR procedures, lower risk and complication rates were reported when compared with other procedures.Suhet al[34] reported complication rates of 3.5% to 45% of minor complications in more than 50% of LCL studies.They also reported a 30% rate difference in complications between silicone, polyethylene, staple, titanium, bioresorbable, and stainless steel “old-type” AR implants (45%) and “recent-type” implants (15.4%).In this review, the overall complication rate was 8.2%; 7.2% with CS devices and 9.7% with subtalar AR.Differences in the potential for complications are related to the CS technique or subtalar self-locking devices[35].
As sinus tarsi pain is the most common complication (54.0%) associated with subtalar self-locking devices[35], with a total of 40 cases (5.2%).It has hypothesized that extrusion and over- or under correction occur because of the difficulty of finding the correct dimension of the implant.Under correction can result from a small device that cannot fully correct excessive subtalar joint eversion, and allow a few degrees of remaining eversion.On the other hand, if the chosen implant size is too large, the subtalar joint motion could be limited, thus resulting in pain or extrusion caused by weight bearing activities.The most frequent complication of CS procedures was the incomplete correction of the deformity (24 cases, 2.2%), transient pain, or discomfort at the incision site (20 patients, 1.8%).
Regarding surgery, no consensus is present about the indications for bioabsorbable, nonabsorbable, or a combination of implant materials[17].Fourteen studies evaluated nonabsorbable implants (seven CS and 7 subtalar AR studies) and four (three CS[20,24,25], and one subtalar AR[26]) evaluated bioabsorbable implants.Both AR categories were found to result in improvement of clinical and radiological outcome measurements.Major advantages of the use of bioabsorbable implants include decreased interference during magnetic resonance imaging and avoidance of a second surgical procedure for hardware removal.Disadvantages and possible complications include screw breakage, inflammatory and foreign body reactions, cyst formation, and local bone lysis[29].In the bioabsorbable implants studies, below-knee boot and crutch gait assistance were needed immediately after surgery for weight bearing or partial weight bearing to prevent implant breakage.Aggressive walking or athletic activities were not allowed.Fourteen of the 419 implanted bioabsorbable devices (3.3%) were broken compared with the only CS screw breakage in 683 nonabsorbable implanted devices.Polymer chemical structure, processing conditions and storage history, implant molecular weight, crystallinity, and size are common reasons of premature poly-(Llactide) degradation.Cellular responses may include mild and temporary inflammatory reactions[23].Despite implant rupture, the patients had good self-reported results, comparable to the other patients, even after having the implant removed[24,25].A few months were not considered sufficient to promote complete correction of the deformity[9].On the other hand, a second surgery was often necessary to remove nonabsorbable implants.In the AOFAS 2015 web-based survey[30], one-third of the participants who performed subtalar AR had decided to abandon the procedure because of the failure rate and the need for implant removal.Many participants who were dissatisfied by the AR practiced in the United States.Some authors believe that abandonment might be related to problems with health insurance payments[11].
Surgeon experience, implant costs, and cosmetic correction are the most common considerations in the orthopedic decision-making process.The CS procedure is less expensive surgery, compared with any of the other implants[16,17].Moreover, Ortizet al[19] noted that, in selected patients, tarsal canal implants produced better cosmetic corrections compared with the CS technique.
Few high-quality studies AR studies have been published.To the best of our knowledge, two systematic reviews and one meta-analysis were previously published.Baryehet al[36] reported partially conclusive data supporting the subtalar AR as an adjunct treatment, but the analysis was limited to adult acquired flatfoot.Suhet al[34] performed a comparison between AR and the LCL procedures and concluded that LCL achieved more radiographic corrections and more improvements in the AOFAS score than the AR.Complications were more common in the LCL group than in the AR group, and the reoperation rates in the two groups were similar.As reported in a recent European Pediatric Orthopedic Society flatfoot survey[3], the procedure indications are different.At the same time, the survey included dated findings regarding AR complications and first AR devices.A meta-analysis by Hsiehet al[37] in 2020 did not find a superiority between subtalar AR and CS procedures according to the clinical score, but endosinotarsal devices showed a better improvement in Meary’s angle than exosinotarsal screws.Despite the remarkable conclusion, some concerns were present, for example, the authors chose the AOFAS score for the clinical assessment and Meary’s angle for the radiological evaluation.Neither measurement is specific for juvenile FFF, moreover in the few studies included in the meta-analysis, the assessments were not the primary study outcomes and were supplemented with other measurements.In addition differences in study design made group comparability difficult in some cases.
The strength of this study is the reporting of the most important evidence published in the last 5 years.Major limitations include great heterogeneity of the outcome assessments and the lack of high-profile studies.We extensively searched and identified all relevant investigations of FFF treated with AR devices.Therefore, risk of bias assessment had moderate overall risk of influencing our analysis.Statistical analysis was not performed.Variations in clinical and radiological scores were reported in the selected studies.Often more than one measurement was performed in order to evaluate different disease features.Moreover, no FFF-specific scores or X-ray lines were developed, and randomized clinical trials are missing and few were casecontrol studies.In our opinion, the analysis of partial or not high-quality study data could be misleading.
CONCLUSION
In conclusion, despite both AR procedures being valid surgical techniques for the treatment of FFF, surgeon experience, implant cost, and cosmetic correction are the most common considerations in the orthopedic decision-making process and AR choice.In obese patients, subtalar ARs are not recommended.In adolescents who need to improve sports performance, CS screws had a slightly lower rate of complications than subtalar self-locking implants.
ARTICLE HIGHLIGHTS
Research background
Flexible flatfoot (FFF) is a common disorder during childhood.When symptoms of early and easy fatigue during walking or pain are present, treatment is mandatory.Arthoereisis (AR) is frequently used for surgical management.Two device types were described, subtalar AR and calcaneo-stop (CS).
Research motivation
No common consensus or AR among orthopedic surgeons is present.
Research objectives
The aim of the study was to report the clinical and radiological outcomes after subtalar AR and CS procedures, including the results in obese and athlete populations, and the technique-related complications.Moreover, the intent was to include the more recent findings of the material devices.
Research methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)guidelines were used to perform a systematic review of English-language articles published of the last 5 years.
Research results
Seventeen articles were included in the study after the initial screening and the risk of bias assessment.A total of 1864 FFFs were identified.Eight studies evaluated subtalar AR and nine evaluated CS (52.9%).At the start of treatment, the average age of patients was 11.8 years and the average study follow-up was 71.9 mo.
Research conclusions
Both AR procedures are valid surgical techniques for FFF treatment, surgeon experience, implant cost, and cosmetic correction were the most common considerations in the orthopedic decision-making process and AR choice.In obese patients, the subtalar AR is not recommended.In adolescents who need to improve sports performance, the CS screw had better results compared with other implants.In adolescents who need to improve sports performance, CS screws had a slightly lower rate of complications than subtalar self-locking implants.
Research perspectives
High-quality randomized clinical trials are needed.
杂志排行
World Journal of Orthopedics的其它文章
- Developing an enhanced recovery after surgery program for oncology patients who undergo hip or knee reconstruction surgery
- Slacklining: A narrative review on the origins, neuromechanical models and therapeutic use
- Off-the-shelf 3D printed titanium cups in primary total hip arthroplasty
- Evidence-based approach to providing informed consent for hip fracture surgery during the COVID-19 era
- Dermatomyositis and polymyositis in total hip arthroplasty
- Outcome and revision rate of uncemented humeral head resurfacing:Mid-term follow-up study