Dermatomyositis and polymyositis in total hip arthroplasty
2021-06-18SamuelRosasMichaelSchallmoAnirudhKrishnaGowdMatthewReynoldsAkelmanDavidLuoCynthiaLynnEmoryJohannesFrankPlate
Samuel Rosas, Michael Schallmo, Anirudh Krishna Gowd, Matthew Reynolds Akelman, T David Luo, Cynthia Lynn Emory, Johannes Frank Plate
Samuel Rosas, Anirudh Krishna Gowd, Matthew Reynolds Akelman, T David Luo, Cynthia Lynn Emory, Johannes Frank Plate, Department of Orthopedic Surgery, Wake Forest School of Medicine, Winston Salem, NC 27101, United States
Michael Schallmo, Department of Orthopedic Surgery, Atrium Healthcare, Charlotte, NC 28203, United States
Abstract BACKGROUND Idiopathic inflammatory myopathies (IIM) are systemic autoimmune disorders such as dermatomyositis (DM), polymyositis (PM), inclusion body myopathy, and autoimmune necrotizing myopathy that, similar to osteoarthritis, affect quality of life and activities of daily living.Moreover, these patients are often burdened with chronic pain and disability; however, the outcomes and risk of total hip arthroplasty (THA) in this patient population remain unclear.AIM To evaluate 90-d complications and costs in patients with these conditions.METHODS A retrospective case control study was designed by accessing data from the Medicare dataset available on the PearlDiver server.Patients with IIM, here, those with DM and PM were matched based on possible confounding variables to a cohort without these diseases and with the same 10-year risk of mortality as defined by the Charlson Comorbidity Index Score (CCI).Univariate and multivariate analysis were performed to evaluate complications and t-tests to evaluate 90-d Medicare reimbursements as markers of costs after THA.RESULTS The total sample was 1090 patients with each cohort comprised of 545.Females were 74.9% of the population.The mean CCI was 5.89 (SD 2.11).Those with IIM had increased rates of pneumonia [odds ratio (OR) 1.45, P < 0.001] and pulmonary embolism (OR 1.46, P = 0.035) and decreased hematoma risks (OR 0.58, P = 0.00).90-d costs were on average $1411 greater for those with IIM yet not significantly different (P = 0.034).CONCLUSION Patients with IIM have an increased 90-d rate of pneumonia and pulmonary embolism concomitant with a decreased hematoma rate consistent with their procoagulatory state.Further attention to increased resource utilization in these patients is also warranted.
Key Words: Dermatomyositis; Arthroplasty; Polymyositis; Outcomes; Charges; Reimbursement
INTRODUCTION
Preoperative patient expectations are an important factor in a patient’s decision to undergo arthroplasty[1-3].Such expectations are intimately related to, among other factors, the likely risks and benefits for an individual patient[1-3].As a result, there is burgeoning interest in all surgical specialties towards quantifying the expected risks and benefits associated with a given procedure[4].
One particular population that has not been widely studied with respect to arthroplasty are patients with idiopathic inflammatory myopathies (IIM), a group of four rare, systemic autoimmune disorders [dermatomyositis (DM), polymyositis (PM), inclusion body myopathy, and autoimmune necrotizing myopathy] that share a number of clinical characteristics[5-7].IIM patients have baseline increased risk of deep vein thromboses and death[5-9].
Degenerative joint disease is observed in up to 53% of patients with IIM[10].It is unclear whether IIM directly contributes to joint degeneration[6,7].High-dose corticosteroids are also often necessary to control major manifestations of IIM, which may result in osteonecrosis and eventual collapse and destruction of joints[9].
Despite the proven success of total hip arthroplasty (THA) in the general population, patients with IIM are amongst the most complex patients who undergo this procedure and there is a paucity in the evidence-based literature with regards to whether these patients experience a higher rate of complications, higher costs, or poorer outcomes following surgery[9,11,12].
The purpose of this study was to evaluate ninety-day complications and costs in patients with IIM, specifically DM or PM, undergoing primary THA for end-stage hip arthritis.The study hypothesized that patients with IIM would experience a higher rate of complications and higher costs following THA compared with the general population.
MATERIALS AND METHODS
Given the low prevalence of IIM, a retrospective review was performed using a national database of surgeries and outcomes.A subset of the United States Medicare patient population was evaluated by way of the Medicare Standard Analytical Files.This dataset is available on the PearlDiver server (PearlDiver Inc., Colorado Springs, CO, United States), a health insurance portability and accountability act-compliant and commercially-available software that allows for scrutiny of large number of records through International Classification of Disease, Ninth Revision (ICD-9) and Current Procedural Terminology (CPT) codes.This server contains over 50 million patient records and has been used extensively by various groups around the country to study a variety of conditions and diseases.No Institutional Review Board approval was required for this study, given the de-identified dataset.
Adult patients with a diagnosis of IIM were identified through ICD-9 710.3 (DM) and 710.4 (PM).These two specific conditions were used as a surrogate for IIM as a whole, given that the available IIM literature–particularly with respect to morbidity and mortality–tends to focus primarily on these two conditions.Cases of THA were identified through ICD-9 81.51 and CPT 27130.Hemiarthroplasty and revision procedures were excluded from the study.Included patients with IIM who underwent primary THA were then matched with controls at a one-to-one ratio through a wellestablished, comprehensive set of variables.These included age distribution, sex and Charlson Comorbidity Index (CCI).The CCI is a validated predictor of 10-year mortality and has been widely used across multiple medical specialties.Following the matching process, patient groups were compared with respect to age distribution, sex, geographic region where the procedure was performed, and specific comorbidities.
The outcomes assessed in this study included postoperative complications and costs.Diagnosis codes used to identify and compare complications in the postoperative period were similar to those used in previous studies and are reported in Supplementary material[13].Reimbursement data for day-of-surgery and the ninety-day postoperative period were collected as a surrogate for costs[14].The ninety-day timeframe was chosen as it is the most common time frame involved in bundled payment programs.
Statistical analysis
All statistical analyses were performed using R (R Foundation for Statistical Computing, Vienna, Austria).Chi-square tests with Fischer corrections were used for dichotomous variables and pairedt-tests were used for cost data after it was determined that the data was parametric through the Kolmogorov-Smirnov test.Multivariate regressions including age, gender, CCI and the presencevsabsence of IIM were performed for each of the outcomes of interest, yielding an adjusted odds ratio (OR) with corresponding 95% confidence interval (CI).For all statistical analyses, the threshold for significance was established atP≤ 0.05.Unless noted otherwise, numerical values given were mean ± SD.
RESULTS
Initial query of the database identified 78005 patients with a diagnosis of IIM and 1145631 cases of THA.After inclusion, exclusion, and matching criteria were applied, 1090 patients were captured for a final total of 545 patients in each of the two groups from 2005 to 2014.
The majority of patients were aged 69 and younger, with no significant difference in age distribution between groups (Table 1).
Females comprised the majority of patients in both groups, with 408 (74.9%) in each (P= 1.000).There were no significant differences between groups with respect to the geographic distribution of patients by region (P= 0.185).
The mean CCI was identical for both groups (5.89 ± 2.11;P= 1.000).Compared with patients with IIM, a significantly higher proportion of patients in the control group had diabetes mellitus (59%vs44%;P< 0.0001), pulmonary disease (56%vs46%;P= 0.001), and peripheral vascular disease (31%vs30%;P= 0.008).Table 2 presents the pre-operative comorbidity profiles of both cohorts.Groups were otherwise similar with respect to comorbidities.
Multivariate regression analysis demonstrated that, compared with controls, patients with IIM had a higher risk of developing pneumonia (OR = 1.456, 95%CI: 1.170-1.812;P= 0.001) and pulmonary embolism (OR = 1.460, 95%CI: 1.026-2.077;P= 0.035) following THA (Table 3).Further, regression analysis demonstrated that patients with IIM had a lower risk of hematoma formation that became clinically significant compared with controls (OR = 0.582, 95%CI: 0.406-0.833;P= 0.003).Groups were otherwise similar with respect to risk of complications following THA.
When evaluating mean day-of-surgery reimbursements, there were no significant differences identified between IIM patients ($12952 ± $4002perpatient) and controls ($12445 ± $3857perpatient;P= 0.299).Similarly, mean ninety-day reimbursements were comparable for patients with IIM ($15530 ± $4901perpatient) and controls ($14480 ± $4525perpatient;P= 0.140).
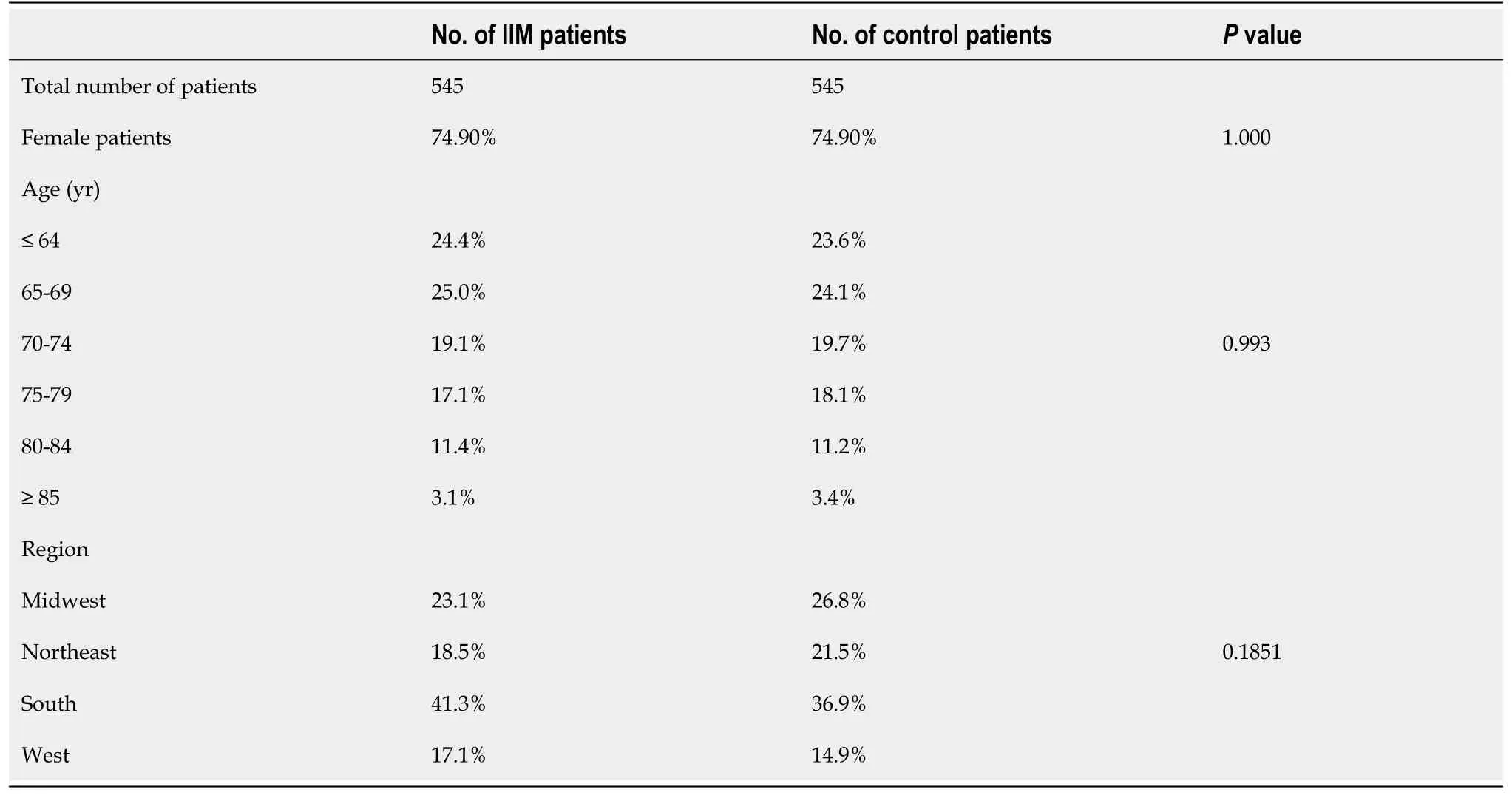
Table 1 Demographic factors for patients included in this study
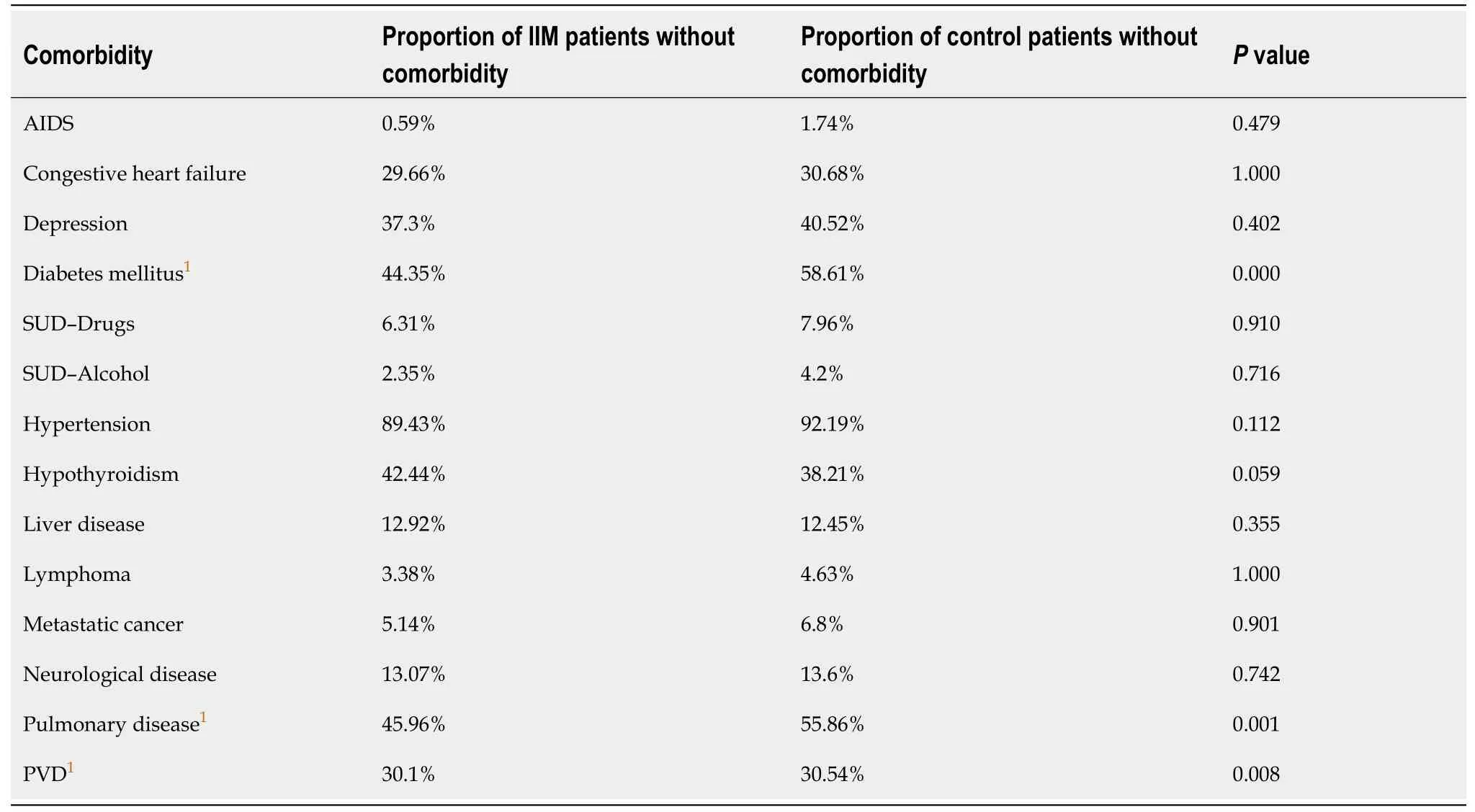
Table 2 Additional comorbidities for patients included in this study
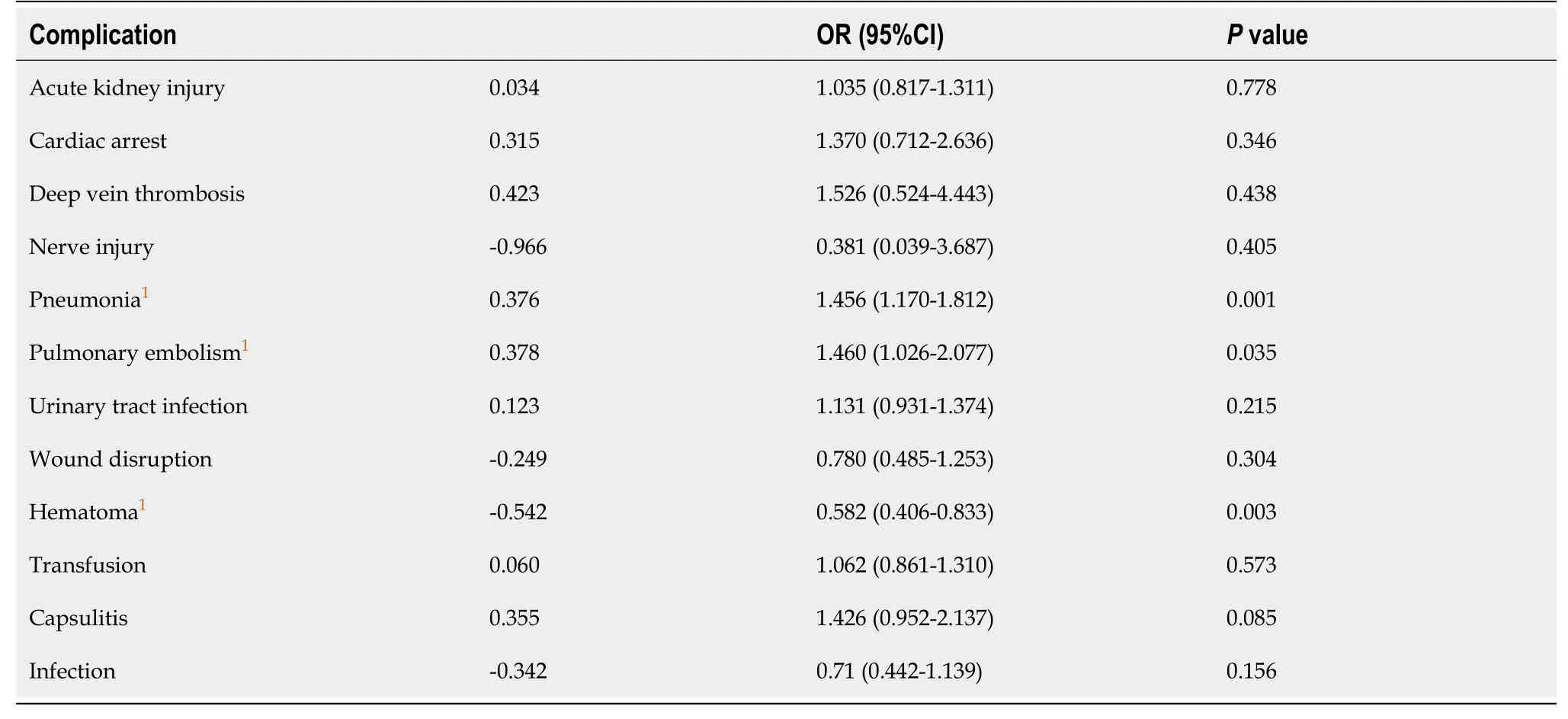
Table 3 Results of multivariate regression analysis to evaluate the relative risk of complications in patients with idiopathic inflammatory myopathies compared with controls following total hip arthroplasty
DISCUSSION
The results of this study support the hypothesis that patients with IIM experience a higher rate of ninety-day complications, namely pneumonia and pulmonary embolism, following THA.However, the study results also contradict part of our hypothesis in that costs (as represented by ninety-day reimbursements) were similar between patients with IIM and controls.Interestingly, there was one complication (clinically diagnosed hematoma formation) we identified that occurred less frequently in patients with IIM, likely given the pro-thrombotic state of these inflammatory conditions as discussed below.To our knowledge, this is the first study to comprehensively analyze the specific complications and reimbursements associated with THA in patients with IIM compared with patients in the general population with a matched comorbidity profile.
There are a myriad of disease manifestations, comorbidities, and medication sideeffects that patients with IIM are susceptible to, which may place them at a higher risk of complications following arthroplasty compared with the general popula-tion[5-9,12,15].One of the most feared and potentially devastating complications in arthroplasty is venous thromboembolism (VTE)[9].Depending on the diagnostic study used and the chosen endpoint (e.g., asymptomatic, symptomatic, fatal,etc.), the risk of VTE following lower-extremity arthroplasty has been reported to be less than 1%-2% when chemoprophylaxis is used[9,16,17].It is well-documented that IIM carries a heightened risk of thromboembolic events, with one study reporting that these patients have an eight-fold higher risk of developing VTE compared with the general population[8].Our study identified that patients with IIM demonstrated a nearly 1.5-fold higher risk of pulmonary embolism compared with controls.The discrepancy in the observed increased risk of thromboembolic events between the two studies is likely due, in part, to the fact that our study used a comorbidity-matched control group, who themselves likely have an elevated risk of thromboembolic events above the general population.Moreover, our findings describe a nationwide cohort representative of the average IIM patient undergoing THA, whereas the study by Antovicet al[8] did not evaluate the rates of VTE in a surgical cohort and instead compared VTE incidences between IIM patients and the general population.Conversely, bleeding and hematoma formation are also potential complications, with 0.41% of patients who undergo THA requiring surgical evacuation of a hematoma[18].Interestingly, this study found that patients with IIM had a 42% lower incidence of hematoma compared with controls, which is in concordance with the hypercoagulable state these patients are in at baseline.
Based on the results of this study and studies involving other high-risk groups undergoing arthroplasty, it may be prudent to use more aggressive postoperative chemoprophylaxis in IIM patients undergoing THA as part of a multimodal approach to overall VTE prophylaxis.Further research is necessary to better characterize the elevated VTE risk and commensurate prophylaxis regimen for IIM patients undergoing THA.
Patients with IIM have an elevated baseline risk of developing pulmonary disease, including pneumonia[5-7,19].The lungs are the most commonly involved extramuscular organs in IIM.Infectious pulmonary complications occur in 26% of IIM patients, withPseudomonasandStaphylococcusbeing the most common causative organisms for pneumonia in these patients[19].In the present study, we found that IIM patients demonstrated a nearly 1.5-fold higher risk of pneumonia compared with controls.It is unclear which, if any, IIM-associated risk factors (e.g., dysphagia, leukopenia, hypoproteinemia, myopathy of thoracic musculature, concurrent immunosuppressive treatment) contributed to the development of pneumonia in our study population or what subtype of pneumonia each patient developed (e.g., community-acquired, hospital-acquired,etc.)[19].Further studies are necessary to better characterize pneumonia in this population, including elucidating the most common mechanisms (e.g., aspiration, poor hand or equipment hygiene of staff,etc.) and whether more intensive therapy or precautions (e.g., pulmonary hygiene, topical decontamination, vaccination,etc.) may be warranted.
With total annual Medicare reimbursements of approximately $20 billion and growing for arthroplasty, considerable efforts have been undertaken to reduce costs and limit spending[20].In this study, we observed similar ninety-day reimbursements between IIM patients ($15530) and controls ($14480).On the one hand, the similarity in reimbursement is commensurate with the matched comorbidity profile of the two groups.On the other hand, given the higher number of complications observed in patients with IIM, it was surprising that we did not observe a corresponding higher reimbursement.With complications comes increased healthcare utilization, leading to increased costs and ultimately increased insurance reimbursements[20-22].The Center for Medicare and Medicaid Services’ Comprehensive Care for Joint Replacement (CJR) bundled payments program penalizes hospitals with higher-than-average reimbursements and rewards hospitals with lower-than-average reimbursements[21].As a result, there is debate as to whether such bundling programs may incentivize hospitals and providers to treat patients who are more profitable (e.g., fewer comorbidities, lower costs) while creating barriers to treatment for higher-risk populations[21].Currently, the CJR program risk-stratifies patients undergoing lower extremity arthroplasty based on diagnosis related group codes, geographic region, and presence of a fracture; there is currently minimal risk adjustment for comorbidities[21].The specific complications quantified in this study contribute to an overall more robust risk stratification for IIM patients undergoing THA.This may have the added benefit of aiding bundled payment negotiations, providing more equitable reimbursement, and ultimately improving access for certain higher-risk patients.
There are a number of limitations with this retrospective data review that must be considered.As with any large, national database, there is the potential for errors, omissions, inconsistencies, and/or variability in the data.When statistical analysis is performed on a large dataset, the establishment of statistically significant differences is likely.Unfortunately, clinically important differences in rates of complications are seldom defined, as they are often subjective.Thus, clinically important differences in rates of complications were not established in our methodology.The database includes no specific operative details (e.g., operative time, anesthesia, intraoperative findings, prosthesis used, antibiotics used, postoperative protocol,etc.).Patients were not stratified based on length-of-stay in the hospital after surgery.Due to the nature of the database query in this study, there is the potential for retrospective bias.Using reimbursement data as a surrogate for costs introduces limitations to our analysis, given the convoluted payment models currently in place in the healthcare industry.In addition, reimbursement values captured in this study were not adjusted for inflation.Notwithstanding, these values represent reimbursements from the biggest payer in the country (Medicare) and thus allow for comparisons between studies[4].This study included a majority of female patients and did not evaluate hemiarthroplasty, revision procedures, or the two remaining IIM groups (inclusion body myopathy and autoimmune necrotizing myopathy), which may limit the generalizability of our results.Lastly, numerous studies have reported consistent validity of the CCI as a prognostic factor for mortality and health costs, the CCI includes only a limited number of fields for diagnosis entry and does not account for the clinical severity of most of the included diagnoses[21,23].Consequently, CCI may potentially underestimate the number and/or extent of comorbidities, which may limit the external validity of our results.In addition, and despite an identical mean CCI for both groups, the control group had a higher frequency of comorbid diabetes, pulmonary disease, and peripheral vascular disease, which may have had a confounding effect on postoperative complications and/or reimbursements.Future studies are needed to prospectively follow these patients and their complications, yet the low prevalence of IIM makes this a difficult feat.
CONCLUSION
Compared with patients in the general population with a matched comorbidity profile, patients with IIM who undergo primary THA are at an increased risk of potentially serious ninety-day complications (pneumonia and pulmonary embolism) and incur similar total costs following surgery.The results of this study may help improve patient selection for surgery and aid physicians in providing a more accurate, individualized risk-benefit assessment for IIM patients prior to surgery.
ARTICLE HIGHLIGHTS
Research background
There is a paucity of data evaluating patients with dermatomyositis (DM) and polymyositis (PM) undergoing total hip arthroplasty (THA).
Research motivation
To compare and contrast the outcomes of patients undergoing THA with DM and PM vs a matched control without inflammatory arthropathies.
Research objectives
To elucidate whether patients with DM and PM have increased risk of complications and greater 90-d costs when undergoing THA compared to controls.
Research methods
A retrospective case control was performed based on the medicare data.
Research results
Patients with DM and PM had increased rates of pneumonia [odds ratio (OR) 1.45, P <0.001] and pulmonary embolism (OR 1.46, P = 0.035) and decreased hematoma risks(OR 0.58, P = 0.00).90-d costs were on average $1411 greater for those with idiopathic inflammatory myopathies (IIM) yet not significantly different (P = 0.034).
Research conclusions
Patients with IIM have an increased 90-d rate of pneumonia and pulmonary embolism concomitant with a decreased hematoma rate consistent with their pro-coagulatory state.
Research perspectives
It is important to evaluate deep vein thrombose prophylaxis and respiratory status in those undergoing THA with DM or PM.
杂志排行
World Journal of Orthopedics的其它文章
- Developing an enhanced recovery after surgery program for oncology patients who undergo hip or knee reconstruction surgery
- Slacklining: A narrative review on the origins, neuromechanical models and therapeutic use
- Off-the-shelf 3D printed titanium cups in primary total hip arthroplasty
- Evidence-based approach to providing informed consent for hip fracture surgery during the COVID-19 era
- Outcome and revision rate of uncemented humeral head resurfacing:Mid-term follow-up study
- Trends in leadership at orthopaedic surgery sports medicine fellowships