Evidence-based approach to providing informed consent for hip fracture surgery during the COVID-19 era
2021-06-18RoryCuthbertDavidFergusonBabarKayaniSaeefHaqueAounAliAsifParkarPeterBatesKrishnaVemulapalli
Rory Cuthbert, David Ferguson, Babar Kayani, Saeef Haque, Aoun Ali, Asif Parkar, Peter Bates, Krishna Vemulapalli
Rory Cuthbert, David Ferguson, Saeef Haque, Aoun Ali, Asif Parkar, Krishna Vemulapalli, Department of Trauma & Orthopaedic Surgery, Queen's Hospital-Romford, London RM7 0AG, United Kingdom
Babar Kayani, Peter Bates, Department of Trauma & Orthopaedic Surgery, Royal London Hospital, London E1 1FR, United Kingdom
Abstract BACKGROUND Hip fractures are the most common reason for inpatient orthopaedic trauma admission.Urgent surgical intervention for hip fractures has remained a clinical priority throughout the coronavirus disease 2019 (COVID-19) pandemic.Despite this, there is a paucity of clinical guidance addressing the informed consent process for hip fracture surgery in COVID-19 positive patients.This is of paramount medicolegal importance in a high-risk patient population.AIM To quantify the additional perioperative risks for COVID-19 positive patients undergoing hip fracture surgery and provide clinicians with an evidence-based framework to establish an informed consent process.METHODS Two hundred and fifty nine consecutive patients undergoing surgical intervention for hip fractures in four hospitals in the United Kingdom were recruited.51 patients were confirmed positive for COVID-19.Predefined outcomes were analyzed over a 30-d postoperative period.COVID-19 positive and COVID-19 negative patients were compared after adjustment for confounding factors.RESULTS COVID-19 positive patients had more intensive care admissions (27% vs 5%, P < 0.001), longer inpatient stays (median 23 d vs 9 d, P < 0.001) and a higher 30-d mortality (29% vs 10%, P = 0.001) than COVID-19 negative patients.Postoperative complications were evident in 74.5% of COVID-19 positive patients.35.3% of COVID-19 positive patients suffered postoperative lower respiratory tract infections with 13.7% developing acute respiratory distress syndrome (ARDS) and 9.8% experiencing symptomatic thromboembolic events.CONCLUSION The COVID-19 pandemic has created uncertainty in the medical community worldwide and poses unique challenges in providing informed consent for surgery.COVID-19 positive patients undergoing hip fracture surgery should be consented for the additional risk of postoperative complications (including lower respiratory tract infection, ARDS, deep vein thrombosis and pulmonary embolism), increased requirement for intensive care admission, longer inpatient stay and higher risk of mortality.Further, clinicians must be transparent about the potential for unknown risks as research into the long-term surgical outcomes of COVID-19 positive patients continues to evolve.
Key Words: COVID-19; Hip fractures; Mortality; Morbidity; Outcome assessment; Informed consent
INTRODUCTION
Hip fractures are the most common reason for inpatient orthopaedic trauma admission, with an estimated 1.6 million cases globallyperyear[1].Incidence has remained stable during the coronavirus disease 2019 (COVID-19) pandemic[2], and the British Orthopaedic Association continues to advocate urgent surgical intervention[3].Patients are usually elderly with multiple comorbidities and poor physiological reserves[4].Therefore, it is medicolegally imperative that the material risks inherent in hip fracture surgery for COVID-19 positive patients are addressed and quantified to facilitate an informed consent process.
A multi-center study from our institution reviewed outcomes in 422 hip fracture patients in the Greater London area and found postoperative 30-d mortality in COVID-19 positive patients was 30.5% compared to 10.3% in COVID-19 negative patients (P< 0.001).COVID-19 positive patients were also associated with increased perioperative morbidity, more admissions to the intensive care unit, and increased length of hospital stay compared to COVID-19 negative patients.However, there remains a paucity of focussed clinical guidance for providing informed consent for hip fracture surgery in COVID-19 positive patients.Davies reports that only one in 46 patients undergoing orthopaedic surgery was consented for the risk of complications secondary to COVID-19 infection[5].This underscores the importance of establishing COVID-19 related perioperative risks in hip fracture surgery and providing clinicians with a clear structure to facilitate informed consent.
This study includes an additional 110 patients who were not included in the original multi-center review, and addresses the following objectives: Firstly we seek to quantify the additional perioperative risks for COVID-19 positive patients undergoing hip fracture surgery and secondly we develop an evidence-based framework for providing informed consent for hip fracture surgery during the COVID-19 pandemic.
MATERIALS AND METHODS
Study design
This retrospective cohort study included all patients undergoing surgical treatment for hip fractures at four National Health Service (NHS) hospitals between February 1–May 21, 2020.All adult patients undergoing operative treatment for a closed intracapsular, intertrochanteric or subtrochanteric hip fracture were included.Paediatric patients, open hip fractures, femoral shaft fractures (defined as 5 cm distal to the lesser trochanter) and periprosthetic femoral fractures were excluded.Research approval was obtained from respective departmental leads, and the NHS Research Ethics Committee decision tool excluded need for ethical review.
Patients
Of 259 patients were recruited.51 patients were COVID-19 positive and 146 patients were COVID-19 negative.62 patients were excluded as they were not tested for COVID-19.Patients were classified COVID-19 positive in the presence of clinical symptoms and a positive throat and nose swab assay using reverse transcriptasepolymerase chain reaction (RT-PCR) for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).Patients were classified COVID-19 negative in the absence of clinical symptoms and a negative throat and nose swab assay using RTPCR for SARS-CoV-2.Repeat swabs were performed if patients exhibited new or persistent symptoms.
Data collection
The following predefined study outcomes were recorded by orthopaedic registrars using a standardized collection proforma: Patient demographics and baseline characteristics [age, gender, ethnicity, American Society of Anaesthesiologists (ASA) grade, comorbidities, dementia status, mobility]; preoperative factors (admission haemoglobin, admission leukocytes, RT-PCR SARS-CoV-2 swab results, associated injuries, systemic symptoms on admission, medical treatment on admission); operative factors (time from injury to surgery, type of anaesthesia, surgical procedure, grade of operating surgeon, operative time, intra-operative complications); postoperative outcomes (location of postoperative treatment, outcome at 30-d post-surgery and time from surgery to hospital discharge or mortality); and postoperative complications (COVID-19 positive patients).Outcomes were sourced from electronic medical records.
Statistical analysis
Analyses of the demographics and baseline characteristics of COVID-19 positive and COVID-19 negative patients were performed using the unpairedt-test for continuous variables following normal distributions, and the Mann-Whitney U test for continuous variables not following normal distributions.Categorical variables were compared using the Chi-squared test except for variables with small sample sizes where Fisher’s exact test was preferred.
Outcomes in COVID-19 positive and COVID-19 negative patients were compared statistically before and after adjustment for confounding factors exhibiting a difference between cohorts in the initial analyses (P< 0.2).Logistic regression was performed to analyze binary outcomes.Survival analysis was performed using Cox regression to compare length of inpatient stay.Patients who were still in the hospital and not ready for discharge when the data was finalized were censored.Patients who died were censored at the time of death.
Odds ratios were used to quantify the size of the association between each variable and outcome.ThePvalue for statistical significance was set at < 0.05.The statistical analysis was performed using Stata version 15.1 (Stata Corp LLC, College Station, Texas).
RESULTS
Baseline characteristics and operative factors
There was no significant difference between COVID-19 positive and COVID-19 negative patients for age, gender, ASA grade, comorbidities, dementia, mobility or admission leukocyte levels.Admission haemoglobin levels were significantly reduced in COVID-19 positive patients (108 g/Lvs116 g/L,P= 0.02) (Table 1).
There was no significant difference between COVID-19 positive and COVID-19 negative patients for choice of anaesthesia, surgical procedure or grade of operating surgeon.COVID-19 positive patients had an increased waiting time from admission to surgery (3 dvs2 d,P= 0.03) and reduced operative time (71 minvs80 min,P= 0.008) comparative to COVID-19 negative patients (Table 1).
The effects of COVID-19 on study outcomes
COVID-19 positive patients had more intensive care admissions (27%vs5%,P< 0.001), longer inpatient stays (median 23 dvs9 d,P< 0.001) and a higher 30-d mortality (29%vs10%,P= 0.001) than COVID-19 negative patients (Table 2).
After adjusting for potentially confounding variables, odds of intensive care admission were 4.64 times higher (95%CI: 1.59-13.50,P= 0.005), and odds of 30-d mortality were 3 times higher (95%CI: 1.22-7.40,P= 0.02) in the COVID-19 positive cohort (Table 2).
Postoperative complications were evident in 74.5% of COVID-19 positive patients.35.3% of COVID-19 positive patients suffered postoperative lower respiratory tract infections (LRTI) with 13.7% developing acute respiratory distress syndrome (ARDS).9.8% of COVID-19 positive patients experienced symptomatic thromboembolic events with a 3.9% incidence of deep vein thrombosis (DVT) and a 3.9% incidence of pulmonary emboli (PE) (Table 3).
DISCUSSION
Informed consent is grounded in the assumption that we as clinicians know the risks of a surgical procedure with a reasonable degree of accuracy, and are able to convey these risks to patients in order to facilitate a balanced decision on whether to proceed with surgical intervention.The COVID-19 pandemic has created uncertainty in the medical community worldwide and poses unique challenges in providing informed consent for surgery.
A hip fracture in the elderly population is a life-threatening injury.Despite advancement in prosthesis design, antibiotic prophylaxis and focussed rehabilitation, mortality following hip fracture surgery remains 7.9%-9.6% at 30 d and 22.8%-27.0% at one year[6,7].Operative intervention is recommended to enable early mobilisation, provide effective pain relief and reduce mortality from complications secondary to prolonged bedrest[8].
COVID-19 positive patients had a higher 30-d mortality (29%vs10%,P= 0.001) than COVID-19 negative patients.These findings echo other studies in Europe and America: Results from the Spanish Hip-COVID Observational Study illustrated a 14-d mortality of 30.4% in COVID-19 positive patients[9], while the 30-d mortality for COVID-19 positive patients following hip fracture surgery in New York was 52.9%[10].It is therefore clear that a full and frank discussion about the increased risk of post-operative mortality must form an integral aspect of the informed consent process for COVID-19 positive patients undergoing hip fracture surgery.
Informed consent mandates exploration of alternative treatment options.Nonoperative management of hip fractures typically requires a prolonged period of bedrest or traction.This may condemn patients to weeks of pain; the National Institute for Health and Care Excellence guidelines advocate even if a hip fracture complicates or precipitates a terminal illness, surgery should still be considered as part of a palliative care approach[8].Prolonged bedrest increases the risk of complications such as pneumonia, urinary tract infection and pressure sores[11].In studies prior to the pandemic, hip fracture mortality following non-operative management with bedrest was 63.6%-73.0% at 30 d and 84.4% at one year[12,13].In patients managed nonoperatively in the Spanish Hip-Covid Observational Study, the 14-d mortality was 67%[9].These mortality rates are significantly higher than 30-d mortality rates reported in COVID-19 positive patients following hip fracture surgery.Therefore, COVID-19 positive patients who are medically fit for hip fracture surgery should be advised that existing literature does not support deviation from surgical intervention as the optimum standard of care.
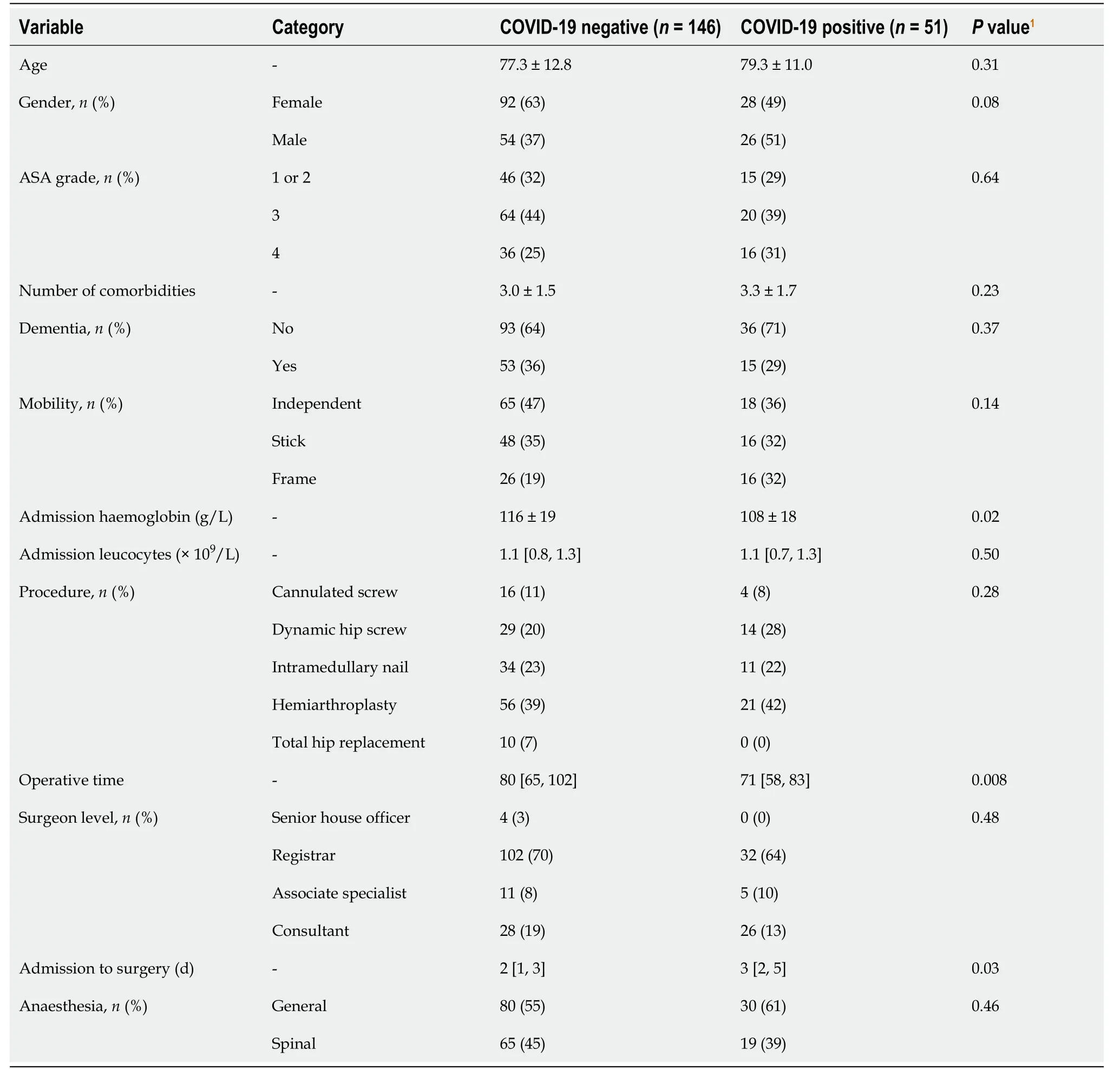
Table 1 Patient demographics and baseline characteristics
COVID-19 positive patients had more intensive care admissions (27%vs5%,P< 0.001) and longer inpatient stays (median 23 dvs9 d,P< 0.001) than COVID-19 negative patients.Although often overlooked and not technically a prerequisite of the informed consent process, preoperative discussion regarding location of postoperative care and anticipated length of inpatient stay are invaluable in ensuring patients develop realistic expectations for their recovery.Further, providing a pragmatic estimation for duration of inpatient stay enables patients to prepare in advance for the logistical complexities of mandatory self-isolation post hospital discharge for COVID-19 positive patients.This is especially important when care arrangements need to be made for other vulnerable persons living at the same address as the patient.
Postoperative complications were evident in 74.5% of COVID-19 positive patients.35.3% of COVID-19 positive patients suffered postoperative LRTI with 13.7% developing ARDS (Table 3).This reflects results from the CovidSurg collaborative which analyzed 835 COVID-19 positive patients undergoing emergency surgery and identified post-operative LRTI in 40% of patients with 14.3% developing ARDS[14].Prior to the pandemic, the rate of LRTI post hip fracture surgery was estimated to be 4.9%-7.0% with the combined incidence of atelectasis, respiratory failure, pulmonary embolism and ARDS at 4%[15,16].It is theorised that fracture and surgical intervention may trigger an oxidative stress response promoting excessive inflammation and decreasing patients’ immunity–increasing the likelihood of respiratory complications secondary to COVID-19 infection[17].Therefore, COVID-19 positive patients undergoing hip fracture surgery must be consented for the increased risk of postoperative LRTI and development of ARDS.
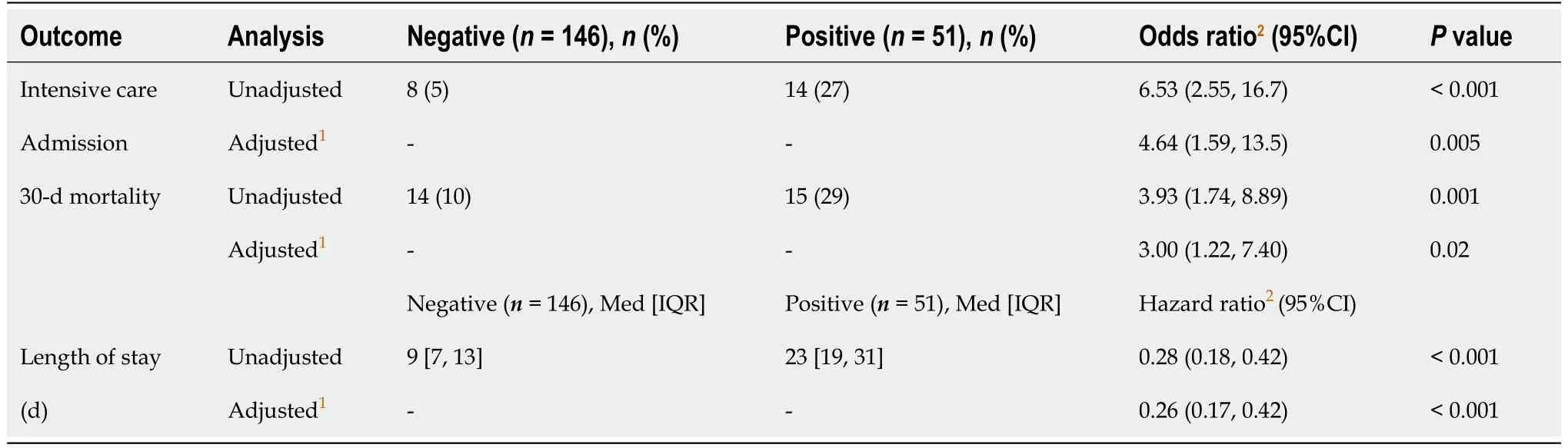
Table 2 Comparison of outcomes between coronavirus disease 2019 positive and coronavirus disease 2019 negative cohorts
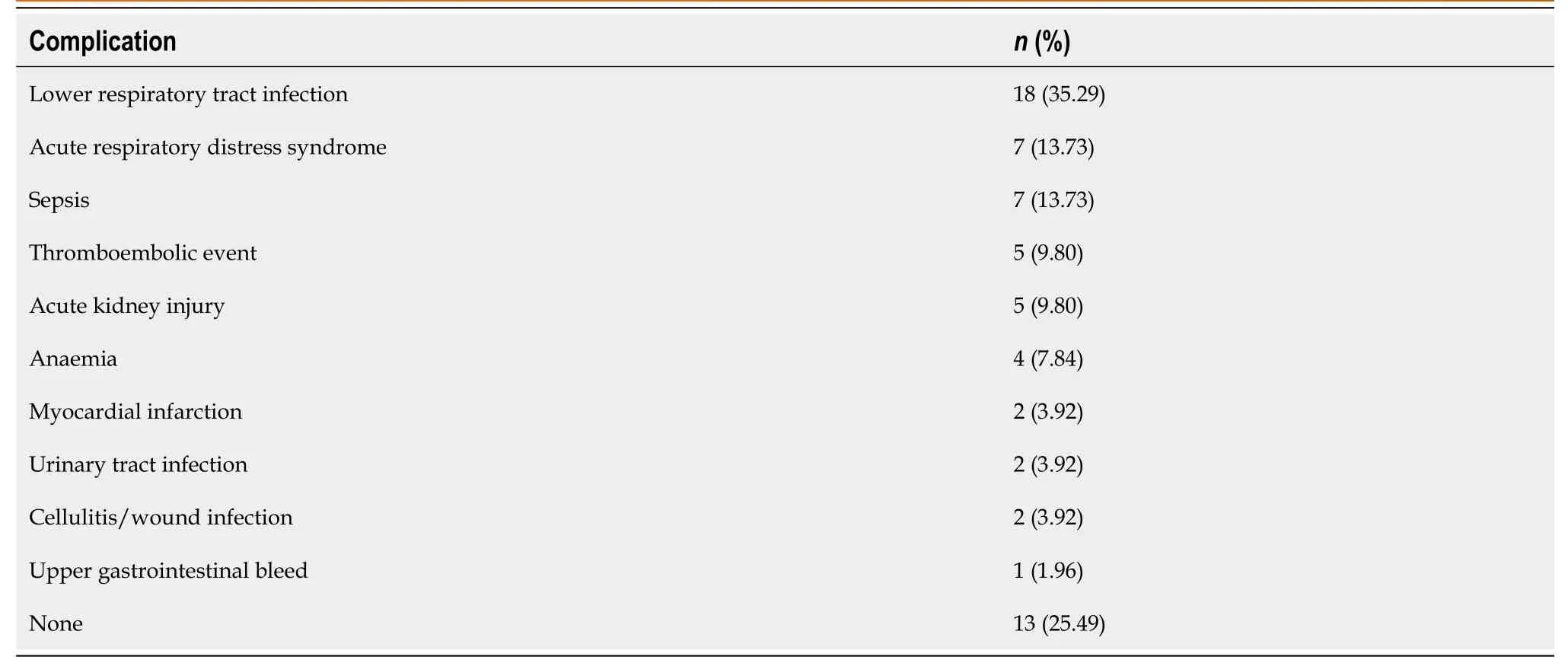
Table 3 Postoperative complications in coronavirus disease 2019 positive patients
The British Orthopaedic Association’s blue book for the care of patients with fragility fractures reports a 3% incidence of symptomatic DVT and a 1% incidence of pulmonary embolism following hip fracture surgery[18].In our study, 9.8% of COVID-19 positive patients experienced a symptomatic thromboembolic event with a 3.9% incidence of DVT, a 3.9% incidence of PE and a 1.96% incidence of cerebrovascular infarction.This corroborates findings from the CovidSurg collaborative where 2.2% of COVID-19 patients undergoing emergency surgery developed postoperative PEs[14].In critically unwell COVID-19 positive patients, rates of thromboembolic events are even higher–with 25% patients admitted to an intensive care unit in Holland developing a DVT after 21 d[19].
Patients with hip fractures and COVID-19 infection automatically fulfil two of the three criteria in Virchow’s triad for thrombus formation: Venous stasis due to immobility and hypercoagulability secondary to an inflammatory state[20].Evidence suggests COVID-19 may also cause the third criteria: endothelial injury.It is proposed that serum levels of angiotensin 2 are elevated in COVID-19 positive patients stimulating production of reactive oxygen species responsible for the breakdown of nitric oxide which leads to endothelial dysfunction[21].In the context of these studies, it is prudent to consent COVID-19 positive patients undergoing hip fracture surgery for the increased risk of postoperative thromboembolic events, and to reiterate the importance of compliance with venous thromboembolism protocols.
In summary, COVID-19 positive patients undergoing hip fracture surgery should be consented for the increased risk of postoperative complications (including LRTI, ARDS, DVT and PE), increased requirement for intensive care admission, longer inpatient stay and a higher risk of mortality.Further, COVID-19 has enforced an additional requirement for the informed consent process: Transparency about the potential for unknown long-term risks and an honest admission of how little we currently understand as research into the long-term surgical outcomes of COVID-19 positive patients continues to evolve.
The principle strengths of this study are that a robust and comprehensive range of predefined study outcomes were recorded using a standardized collection proforma; the study collected data over a four month period from four NHS hospitals at the epicentre of the United Kingdom’s COVID-19 outbreak providing a large sample size; only those patients with confirmed COVID-19 positive or COVID-19 negative swab assays were included rather than reliance on interpretation of vague and variable symptomatology; and the study included a control group of COVID-19 negative patients undergoing operative intervention in the same time period with outcome analysis including adjustment for confounding variables between cohorts.
This study has limitations which must be considered when interpreting findings.Diagnosis of COVID-19 was reliant on a positive throat and nose swab assay with a systematic review of the accuracy of COVID-19 tests establishing false negative rates between 2% and 29%[22].Further, our study focussed exclusively on patients undergoing hip fracture surgery.This minimized demographic and surgical confounders, but makes the generalisability of our findings to other trauma or elective orthopaedic procedures unclear.
CONCLUSION
COVID-19 positive patients undergoing hip fracture surgery should be consented for the increased risk of postoperative complications (including lower respiratory tract infection, ARDS, DVT and pulmonary embolism), increased requirement for intensive care admission, longer inpatient stay and a higher risk of mortality.Both clinicians and patients must acknowledge these risks as part of a detailed informed consent process.
ARTICLE HIGHLIGHTS
Research background
The incidence of hip fractures has remained stable throughout the coronavirus disease 2019 (COVID-19) pandemic, and urgent surgical intervention continues to be prioritized.However, there remains a persistent lack of clinical guidance addressing the subject of informed consent for COVID-19 positive patients undergoing hip fracture surgery.This is of paramount medicolegal importance in a high-risk patient cohort.
Research motivation
The COVID-19 pandemic has created novel challenges and uncertainties in providing informed consent for surgery throughout the medical community.Hip fractures are the most common reason for inpatient orthopaedic trauma admission, with an estimated 1.6 million cases globally per year.Therefore, an evidence-based framework for facilitating an informed consent process for hip fracture surgery would provide clinicians with valuable support and clarity worldwide.
Research objectives
This study had two primary objectives.Firstly, we aimed to quantify the additional perioperative risks for COVID-19 positive patients undergoing hip fracture surgery.Secondly, we sought to provide clinicians with an evidence-based framework for facilitating informed consent in COVID-19 positive patients undergoing hip fracture surgery.
Research methods
Two hundred and fifty nine consecutive patients undergoing hip fracture surgical intervention in four hospitals in the United Kingdom were recruited.51 patients were confirmed positive for COVID-19.Predefined study outcomes were recorded over a 30-d period using a standardized collection proforma.COVID-19 positive and COVID-19 negative patients were compared statistically before and after adjustment for confounding factors.Logistic regression was performed to analyze binary outcomes.Survival analysis was performed using Cox regression to compare length of inpatient stay.
Research results
After adjusting for potentially confounding variables, in COVID-19 positive patients the odds of intensive care admission were 4.64 times higher (95%CI: 1.59-13.50,P= 0.005) and the odds of 30-d mortality were 3 times higher (95%CI: 1.22-7.40,P= 0.02).75% of COVID-19 positive patients suffered post-operative complications.35.3% experienced postoperative lower respiratory tract infections, 14.3% developed acute respiratory distress syndrome (ARDS) and symptomatic thromboembolic events were evident in 9.8%.
Research conclusions
We conclude that the informed c onsent process for COVID-19 positive patients undergoing hip fracture surgery should discuss the additional risk of postoperative complications (particularly lower respiratory tract infection, ARDS, deep vein thrombosis and pulmonary embolism), increased requirement for intensive care admission, longer inpatient stay and higher risk of mortality.
Research perspectives
This study contributes to the body of literature reporting short-term surgical outcomes in COVID-19 positive patients.Future research in this field should analyze long-term surgical outcomes in COVID-19 positive patients.In the interim, it is integral that clinicians are transparent with patients that long-term risks of surgery in COVID-19 positive patients remain unknown.
杂志排行
World Journal of Orthopedics的其它文章
- Developing an enhanced recovery after surgery program for oncology patients who undergo hip or knee reconstruction surgery
- Slacklining: A narrative review on the origins, neuromechanical models and therapeutic use
- Off-the-shelf 3D printed titanium cups in primary total hip arthroplasty
- Dermatomyositis and polymyositis in total hip arthroplasty
- Outcome and revision rate of uncemented humeral head resurfacing:Mid-term follow-up study
- Trends in leadership at orthopaedic surgery sports medicine fellowships