Bilateral ureteral reconstruction using appendicular interposition combined with Wallace anastomosis following stenosis after radical cystectomy and ileal neobladder construction
2021-05-27TakashiMuranaka
Dear Editor,
Ureteral stenosis at anastomotic site is a common complication of radical cystectomy with construction of an ileal conduit or an ileal neobladder.Reconstruction is sometimes challenging because of difficulty to achieve adequate length of the ureter after resection of the fibrotic ureteral tissue.Here we report a case whose bilateral ureteral stenoses at anastomotic sites were successfully reconstructed using appendicular interposition combined with Wallace anastomosis.
A 60-year-old man with muscle invasive bladder cancer underwent laparoscopic radical cystectomy with construction of an ileal neobladder by Studer’s method.Since bilateral ureteral stenoses developed at anastomotic sites just after the operation,bilateral percutaneous nephrostomy tubes were placed.At 10 months,we reconstructed the bilateral ureters via open surgery.After adequate resection of the fibrotic ureteral tissue,we judged that the right ureter could be directly anastomosed to the afferent limb of the neobladder,whereas the left ureter could not because there was a 5 cm distance between the left ureteral end and the afferent limb.Thus,the appendix,which was 7 cm in length,was harvested for interposition between the left ureteral end and the afferent limb.After incision of the mesoappendix while preserving the appendicular artery,the base of the appendix was dissected and then the apical end of the appendix was opened.The basal side of the appendix was anastomosed to the left ureter.After 1.5 cm spatulations were made on the right ureteral end and the apical end of the appendix,the right ureter,left appendicular ureter and the afferent limb of the neobladder were anastomosed in a tension-free manner(Fig.1).Although urine passage through the anastomotic site was insufficient just after the reconstruction,it improved as time passed without any intervention.At 3 and 6 months after the reconstruction,the right and left nephrostomy tubes could be removed,respectively.Four years after the reconstruction,no recurrence of stenosis was observed.
It is difficult to simplify and standardize the method for revision because the conditions and situations of anastomotic stricture vary among individuals depending on the laterality,length of the stricture,degree of bowel adhesion and fibrosis surrounding the stricture,body mass index and so on.Thus,we should have several options for revision according to the situation encountered during the surgery.
There have been several reports on the clinical usefulness of the appendix as a substitute ureter[1-3].There are several merits of the appendicular ureter such as its lesser invasiveness and avoidance of complications like ileus and short bowel syndrome induced by harvesting an additional bowel segment.On the other hand,the major demerit is that appendicular interposition is not always possible because of the limited length and mobility of the harvested appendix.In this case,although urine passage through the anastomotic site was insufficient just after the reconstruction,no intervention was performed because of anxiety about iatrogenic complications of balloon dilation such as ureteral injury and ischemia.Since we were confident about the procedure of the reconstruction,we decided to wait as long as possible because the insufficient drainage might have been due to edema and/or immature compatibility between the urothelium and intestinal epithelium.Finally,we could achieve a favorable outcome by 6 months after the reconstruction.To create a single unit by anastomosis between a native ureter and a reconstructed appendicular ureter may contribute to long-term patency of anastomotic site.Thus,using the appendix as a substitute ureter is less invasive because a small bowel segment is unnecessary.If it is practically available,this method is one of useful options for reconstruction of the defective ureter.
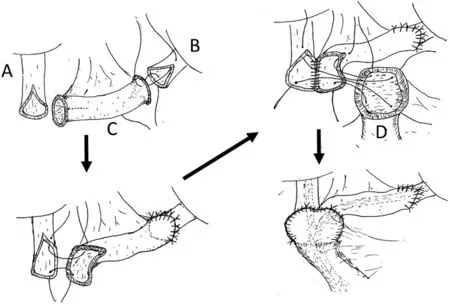
Figure 1 Surgical procedure.(A)Right ureter;(B)Left ureter;(C)Appendix(interposition);(D)Afferent rim of ileal neobladder.
Author contributions
Study concept and design
:Naoya Masumori.Drafting of manuscript
:Takashi Muranaka.Critical revision of the manuscript
:Naoya Masumori.Conflicts of interest
The authors declare no conflict of interest.
Takashi Muranaka
Naoya Masumori
Department of Urology,Sapporo Medical University School of Medicine,Sapporo,Japan
*Corresponding author.
E-mail address:
masumori@sapmed.ac.jp(N.Masumori)8 April 2019
杂志排行

Asian Journal of Urology的其它文章
- Super-mini percutaneous nephrolithotomy
- Are we progressing in prostate cancer management?
- Testicular germ cell tumors
- Multimodal therapy in oligometastatic prostate cancer:A glimpse into the future?
- Cystic nephroma:A bosniak III benign tumor in the kidney
- Expanding luminal epitheliums as cells of origin for prostate cancer