Clinical outcomes of moderate to severe COVID-19 patients receiving invasive vs.non-invasive ventilation
2021-04-29ZubiaJamilSamreenKhalidShahidMumtazAbbasiYasirWaheedJamalAhmed
Zubia Jamil, Samreen Khalid, Shahid Mumtaz Abbasi, Yasir Waheed, Jamal Ahmed
1Department of Medicine, Foundation University Medical College, Foundation University, DHA Phase 1 Islamabad 44000, Pakistan
2Fauji Foundation Hospital, Rawalpindi 46000, Pakistan
3Department of Multidisciplinary Lab, Foundation University Medical College, Foundation University, DHA Phase 1 Islamabad 44000, Pakistan
4Department of Pulmonology, Fauji Foundation Hospital, Rawalpindi 46000, Pakistan
ABSTRACT
KEYWORDS: COVID-19; SARS-CoV-2; Non-invasive ventilation; Respiratory insufficiency; Hypoxia; Mechanical ventilation
1. Introduction
Novel coronavirus (SARS-CoV-2) pandemic has infected millions of people around the world, mainly causing COVID-19 pneumonia and respiratory failure leading to death. There are around 73 million confirmed cases of COVID-19 globally with 1.5 million deaths and 41 million cases recovered[1]. Currently, Pakistan has 445 000 confirmed cases with 9 000 deaths[2].
Most patients with COVID-19 develop mild respiratory symptoms while approximately 14% develop severe SARS-CoV-2 pneumonia that requires hospitalization and oxygen support, and 5% require admission to an intensive care unit[3]. Severe cases can be complicated by acute respiratory insufficiency leading to respiratory failure, hypercoagulability, septic shock and multiorgan involvement resulting in death[4].
Emerging evidence suggests the distinctive COVID-19 pneumonia presents with two phenotypic patterns, type L (characterized by low elastance, low ventilation to perfusion ratio) and type H (high elastance, low compliance and increased lung edema) corresponding to early and late stage lung damage[5]. In early disease, despite severe hypoxemia, patients have normal lung compliance in contrast to acute respiratory distress syndromes (ARDS)[6], which later develop inflammation and cytokine storm leading to severe lung damage, poor lung compliance, and respiratory failure[7].
In more severe disease, an important deficit in the ventilation/perfusion ratio occurs: some lung areas ventilate poorly due to the presence of lung infiltrates and interstitial edema, other areas ventilate well but are not regularly perfused due to the thrombotic occlusion of the vessels[8]. Therefore, oxygen support therapy plays a pivotal role in managing severe COVID-19 pneumonias causing respiratory failure[9].
Non-invasive strategies in the form of high flow nasal cannula,face masks, rebreather masks and bilevel positive airway pressure are commonly suggested methods to improve oxygenation in such patients[10]. However, those requiring intubation and mechanical ventilation have a poor outcome due to additional ventilator associated lung injury[11].
We conducted a retrospective study on COVID-19 patients with acute hypoxemic respiratory failure admitted in High Dependency Unit (HDU) to determine whether non-invasive ventilation has better survival outcomes than invasive mechanical ventilation.
2. Subjects and methods
The primary purpose of this study was to evaluate the in-hospital outcome of moderate to severe COVID-19 patients admitted in HDU in relation to invasive vs. non-invasive mode of ventilation.
2.1. Study design and settings
This was a retrospective observational study carried out from April 2020 to August 2020 at HDU of Fauji Foundation Hospital,Rawalpindi, Pakistan that was specifically designated to treat hypoxemic patients with COVID-19 pneumonia.
2.2. Study participants
All the patients who required admission in HDU during the said period were included in this study. Patients were shifted to HDU through emergency, general wards medical ICU and COVID-19 stable wards.
The following participants were included: (1) Patients of both gender and Age ≥13 years; (2) Patients with moderate COVID-19 disease; (3) Patients with severe COVID-19 disease; (4) Patients with evidence of acute respiratory distress syndrome.
The following participants were excluded: (1) Duration of HDU less than 48 hours; (2) Patients not requiring supplemental oxygen;(3) Patients who were already on long term oxygen therapy (LTOT)prior to admission in HDU due to any chronic lung disease (COPD,ILD, Bronchiectasis); (4) Patient with severe anemia (hemoglobin <6 g/dL); (5) Patients having nephrogenic or cardiogenic pulmonary edema leading to hypoxemia.
2.3. Methodology
Fauji Foundation Hospital, Rawalpindi is a large tertiary care hospital catering the treatment of families of ex-service men. In response to pandemic COVID-19 infection, this hospital established an isolated ward for COVID-19 stable patients with 30-bedded and COVID-19 High Dependency Unit with 24-bedded fully equipped with trained staff, different modes of oxygen delivery, equipment for all investigational therapies, ports for oxygen supply, equipment for positive airway pressure (CPAP and BiPAP), invasive mechanical ventilators. This HDU has 24 hours cover of post graduate trainees who are working under the supervision of pulmonologists,anesthetics and medical specialists with involvement of doctors of all other specialists as needed. All entitled patients or their attendants signed fully informed consent form before admission in which data of patients can be used for research purposes relating to COVID- 19 keeping in view that personal information of every patient is fully concealed before sharing data. Medix software (Electronic health record medical system) is used in this hospital to maintain data of patients and can be traced by specific medical record number allocated to each entitled patient. COVID-19 infection was confirmed by reverse transcription polymerase chain reaction (RTPCR) by taking sample through nasopharyngeal swab. First ethical approval was taken from Fauji Foundation Ethical Committee before collecting data. Before acquiring data, the identity of each patient was made anonymous by the hospital. Records of patients admitted from April 2020 to August 2020 were assessed and analyzed.Patients with all other conditions that can cause or precipitate hypoxemia (anemia, pulmonary edema, chronic lung diseases) were excluded from the study to avoid potential bias.
2.4. Important terminology
Mode of oxygen delivery: Two main methods of ventilation were used. Non-invasive (oxygen ≤10 L/min or >10 L/min through mask or nasal prongs, rebreather masks and bilevel positive airway pressure) and invasive. The indications for use of different oxygen modes were as follows: (1) Oxygen ≤10 L/min or >10 L/min through a mask or nasal prongs, rebreather masks: SpO<94%without signs of respiratory muscle overload and respiratory acidosis on arterial blood gases. (2) Positive airway pressure: R/R >30/min or PO<60 mmHg or pH <7.35 or PCO>45 mmHg on arterial blood gases or signs of respiratory muscle overload or failure of the above strategies to maintain oxygen saturation >94%. (3) Invasive ventilation: hemodynamic instability or altered sensorium or signs of persistent or worsening respiratory failure or R/R >40/min or lack of improvement in signs of respiratory muscle overload or severe respiratory acidosis on ABGs (arterial blood gases) or poor response to the above strategies to maintain adequate oxygen saturations.
Moderate disease: (SpO>90%, but <94%) with chest X ray showing infiltrates <50% of total lung fields or HRCT chest showing peripheral ground glass opacities.
Severe disease: (SpO<90% with or without stable vital signs,respiratory rate >30/min, chest X ray showing infiltrates >50% of total lung fields or HRCT chest showing extensive peripheral ground glass opacities.
ARDS (acute respiratory distress syndrome): Radiological evidence of diffuse chest infiltrates, arterial blood gases (severe; PaO/FiO≤100 mmHg, moderate; PaO/FiO>100 but ≤200 mmHg, mild;PaO/FiO>200 but ≤300 mmHg).
Primary outcome: At 30-day in-hospital, it was death or survival[discharged, recovered (COVID-19 PCR negative), shifted to stable ward] of the patient.
2.5. Statistical analysis
SPSS version 26 and MedCalC were used for statistical analysis.Quantitative variables were expressed as mean ± standard deviation and ranges or median (IQR) wherever appropriate, while qualitative variables were expressed as percentages. Patients were studied by classifying them into two groups: invasive vs. non-invasive groups.Quantitative variables of two groups were compared by student t-test and qualitative variables were compared by chi-square tests. For analysis of 30-day hospital mortality in relation to the use of different modes of oxygen, Kaplan Meier and Log rank analyses were used.In the end, all variables were checked by linear regression analysis to find the independent predictors of outcome in these patients. Only those variables that were found statistically significant on linear regression analysis were further analyzed by Cox regression analysis to find predictors of survival of patients with moderate to severe COVID-19 patients.
3. Results
During the study period from April 2020 to August 2020, 5 567 patients visited this tertiary care unit for COVID-19 screening. The number of patients requiring oxygen inhalation and admission to HDU in the given period was 219 out of 5 567 who had moderate to severe COVID-19 disease. The mean age of the study group was [54.26 ± 17.04] (14-88 years) and the gender distribution was females 75.8% (n=166) vs. males 24.2% (n=53). Oxygen is the mainstay treatment among the hypoxemic patients given by noninvasive or invasive ventilation.
At time of outcome, about 15.1% (n=33) patients with severe COVID-19 infection required invasive mechanical ventilation to correct hypoxemia while 84.9% (n=186) patients needed noninvasive techniques of ventilation. Among non-invasive modes,55.7% (n=122) patients required oxygen <10 L/min through mask or nasal prongs, 5.9% (n=13) required oxygen >10 L/min, rebreather masks for correction of hypoxemia was used in 10.5% (n=23) and bilevel positive airway pressure (BiPAP) was needed by 12.8%(n=28) patients in HDU. The main target was to maintain oxygen saturations above 94% in HDU through different modes of oxygen delivery.
The main aim of this study was to evaluate the clinical outcomes of patients with moderate to severe COVID-19 infection in relation to invasive and non-invasive mode of ventilation. When we compared the biochemical features of two groups, we found that those patients who required invasive ventilation during their management had evidence of thromboembolism (elevated D-dimers), high inflammatory markers (CRP, Ferritin, CPK, IL-6)and hypoxemia (low PaOand oxygen saturations) at the time of admission as compared to group requiring non-invasive ventilation.The comparison of biochemical features of the two groups is shown in Table 1.
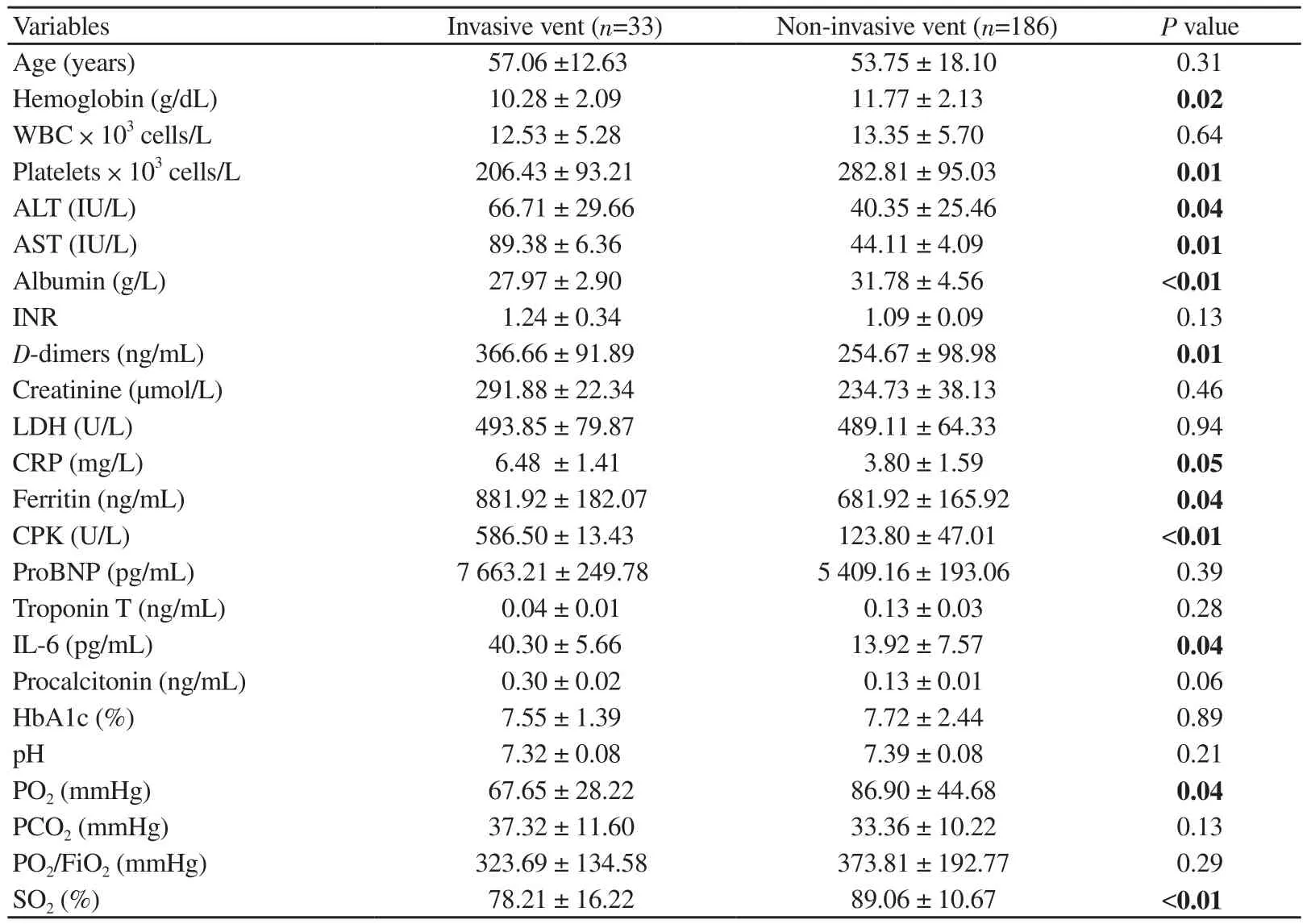
Table 1. Biochemical features of COVID-19 patients stratified by mode of ventilation.
Patients with presence of co-morbid conditions required invasive ventilation more than those who didn’t have any co-morbidconditions (P<0.05). Among 219 patients in HDU, 78.1% (n=171)patients survived while 21.9% (n=48) COVID-19 patients died.According to disease severity, 77 patients (35.2%) had moderate disease while 142 patients (64.8%) had a severe COVID-19 infection. Patients with severe COVID-19 infection required invasive ventilation more than patients with moderate disease (P<0.05).When we compared the survival percentages among non-invasive vs. invasive group, we found that 87.1% (162 out of 186) patients who had non-invasive ventilation survived compared to 27.3% (9 out of 33) requiring invasive ventilation (P<0.05). The comparison of clinical outcomes of two groups is shown in Table 2.

Table 2. Comparison of clinical outcomes of two groups of COVID-19 patients in relation to mode of ventilation.
The 30-day mortality was 72.7% (24 out of 33 patients) for invasive ventilation group and 12.9% (24 out of 186 patients) for noninvasive ventilation group (P<0.05). The median time from hospital admission to outcome (death or survival) was 7 days for group requiring invasive ventilation (IQR=8, HR=3.99, 95% CI=1.96-8.09) and for group requiring non-invasive ventilation this duration was 18 days (IQR=4, HR=0.25, 95% CI=0.12-0.50). This duration was statistically significant among two groups (Log rank x=26.91,P<0.001). The Kaplan Meier analysis, curve showing the overall survival probability of admission to outcome among two groups is shown in Figure 1.

Figure 1. Kaplan Meier analysis curve showing survival probability (%)in patients with invasive vs. non-invasive ventilation during stay in High Dependency Unit. The median time from hospital admission to outcome(death or survival) was 7 days for group requiring invasive ventilation and for group requiring non-invasive ventilation this duration was 18 days(Log rank x2=26.91, P<0.001).
When we compared the 30-day in hospital mortality among moderate to severe COVID-19 patients in relation to different modes of oxygen we found that 30-day in hospital mortality was 1.8% (4 out of 219 patients) for patients with oxygen requirement <10 L/ min.For groups with oxygen requirement >10 L/min, rebreather mask and BiPAP 30-day in hospital mortality was 0.9% (2 out of 219 patients), 3.6% (8 out of 219 patients) and 4.5% (10 out of 219 patients) respectively. The median time from hospital admission to outcome (death or survival) was 19 days for group with oxygen requirement <10 L/min (IQR=4, 95% CI=17.67-21.27), 17 days for group with oxygen requirement >10 L/min (IQR=8, 95% CI=12.42-22.01), 8 days for groups with rebreather mask (IQR=4, 95%CI=6.23-10.29) and 14 days for groups requiring BiPAP (IQR=5,95% CI=10.40-18.72). This duration was statistically significant between these groups (Log rank x=44.76, P<0.001). The Kaplan Meier analysis curve showing the overall survival probability of admission to outcome in relation to the use of different modes of oxygen is shown in Figure 2.
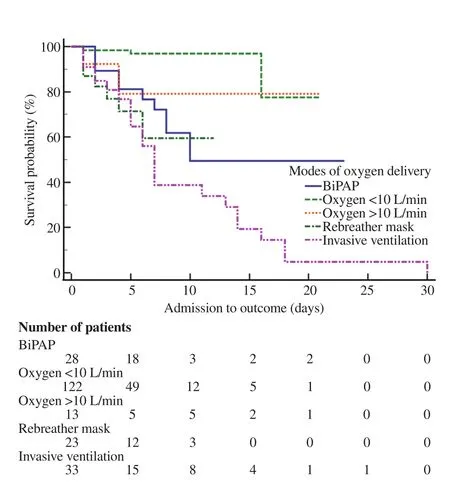
Figure 2. Kaplan Meier analysis curve showing survival probability (%)in patients with different modes of oxygen delivery during stay in High Dependency Unit. The 30-day in hospital mortality was 1.8% for patients with oxygen requirement <10 L/min. For groups with oxygen requirement>10 L/min, rebreather mask and BiPAP 30-days in hospital mortality was 0.9%, 3.6% and 4.5%, respectively. The meadian time from hospital admission to outcome (death or survival) was 19 days for group with oxygen requirement <10 L/min, 17 days for group with oxygen requirement>10 L/ min, 8 days for group with rebreather mask and 14 days for group requiring BiPAP (Log rank x2=44.76, P<0.001).
In the end, regression analysis was used to determine the predictors of outcome in moderate to severe COVID-19 patients during HDU stay. First linear regression analysis was carried out on all variables to find statistically significant predictors. Age,D-dimers level, presence of co-morbid conditions, number of days requiring oxygen, number of days on ventilator support and different modes of oxygen delivery were found to be influencing the outcome in these patients. Then these predictors were analyzed by Cox-proportional hazard regression analysis. Coxproportional hazard regression analysis for various predictors of outcome (determined by linear regression) is shown in Table 3.

Table 3. Variables in predicting the survival of patients with COVID-19 infection according to Cox-proportional hazard regression analysis.
4. Discussion
Supplemental oxygen therapy is the mainstay treatment in patients with acute hypoxemic respiratory insufficiency due to COVID-19 pneumonias. Our study cohort consisted of 219 moderate to severe COVID-19 patients admitted in HDU requiring respiratory support in the form of non-invasive or invasive ventilation. All patients required supplemental oxygen to correct hypoxemia and maintain oxygen saturation >94%. Supplemental oxygen was mainly administered through non-invasive techniques which included O<10 L/min by nasal prongs or face masks, O>10 L /min by face masks,rebreather masks and bilevel positive airway pressure (BiPAP) or rapid transition to invasive mechanical ventilation when non-invasive strategies failed. The rate of intubation and invasive ventilation in our study was 15.1%, while 84.9% patients were subjected to noninvasive ventilation to correct hypoxemia. However, it was higher(from 31% to 84%) in a study conducted by Thille et al[12].
Overall mortality in our HDU was 21.9% (48/219) that was very high. In a review of 15 studies conducted in the countries worst hit by pandemic, the overall ICU mortality rate was around 25%,while it was close to 100% amongst patients requiring mechanical ventilation[13]. Similarly, high mortality rates in ICU were reported by other studies[14].
Mortality was significantly higher in patients with severe disease requiring mechanical ventilation 72.7% (24 out of 33) than those with moderate disease requiring non-invasive strategies of ventilation 12.9% (24 out of 186). This was similar to mortality rate observed by Richardson et al.[15] for patients who received mechanical ventilation which was 76.4% as compared to only 1.98% in patients who did not receive mechanical ventilation. Above 40% patients died on invasive ventilation in another study conducted by Comassi et al[16].
The median duration of HDU stay in patients on invasive mechanical ventilation was 7 days among non-survivors as compared to non-invasive group which was 18 days. The similar duration of 7 to 9 days was observed in other studies showing patients on invasive ventilation have a shorter survival duration than patients on noninvasive ventilation[17,18].
Most patients in our study with severe COVID-19 infection requiring admission in HDU had pre-existing diseases most commonly diabetes mellitus. In COVID-19 disease, the development of pulmonary manifestations to severe hyperinflammation depends on the severity of infection, host response, physiologic reserve,co-morbidities and ventilatory responsiveness of the patient to hypoxemia[8]. These risk factors for disease severity including older age, comorbidities along with abnormal biochemical markers (high D-dimers, IL-6 etc.) were associated with poor outcomes which has been observed in studies of critically ill COVID-19 patients by Zhou et al.[19] and Du et al.[20] as well.
In a meta-analysis of 25 clinical trials on patients with acute hypoxemic respiratory failure secondary to COVID-19 infection by Ferreyro et al.[10] and Frat et al[21], treatment with non-invasive oxygenation strategies were associated with lower risk of death.Vianello et al.[22] proposed non-invasive ventilation with high flow nasal cannula which was a safe treatment in hypoxemic patients with COVID-19 pneumonia. In a study by Duca et al[9], non-invasive ventilation turned out to be a valid strategy in severely hypoxemic patients, and associated with better outcomes[23]. It provides an additional benefit in reducing the risks to healthcare workers by obviating the need for intubation[24].
In our study, the patients of older age groups, with associated co-morbid conditions, persistently elevated inflammatory markers, marked hypoxemia and oxygen saturations below 80%demonstrating the severity of disease required invasive mechanical ventilation more as compared to those with moderate disease and no pre-existing co-morbidities. There was a significant difference in 30-day mortality among patients subjected to invasive mechanical ventilation than those to non-invasive ventilation. A study by Sohaib et al.[25] on 373 patients showed similar results to our study indicating similar predictors of mortality, which included elevated inflammatory markers (D-dimers) and invasive ventilation.
To conclude, our study showed that oxygen delivery is a positive predictor of survival for moderate and severe COVID-19 pneumonia patients with acute respiratory insufficiency. Mechanical ventilation is associated with adverse outcomes possibly due to ventilator associated lung injury. Thus, protective non-invasive ventilation remains the necessary and safe treatment for severely hypoxic COVID-19 patients.
Conflict of interest statement
The authors have no conflict of interest to disclose.
Acknowledgements
The authors like to acknowledge all the paramedical staff, house officers, post graduate trainees, registrars and consultants from all departments of Fauji Foundation Hospital, Rawalpindi who have performed their duties vigilantly, skillfully and with responsibility in HDU during COVID-19 pandemic.
Authors’ contributions
Z.J. developed the conceptualization and performed the statistical analysis. Both S.K. and Z.J. contributed equally in methodology and wrote original draft of this article. Z.J., S.K., S.M.A., Y.W. and J.A.contributed to the writing-review and editing of the manuscript. J.A.supervised the project.
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- Expert consensus on emergency medicine procedure optimization guided by routine prevention and control strategy for COVID-19
- How much will be the cost for universal coverage of COVID-19 vaccination and how shall it be financed?
- COVID-19 vaccination intention among healthcare workers in Vietnam
- Clinical outcomes of hospitalized patients with chikungunya fever: A retrospective analysis
- Severe dengue associated with aseptic meningitis, acute kidney injury, and sudden sensorineural hearing loss: A case report
- Isolation of Kytococcus schroeteri from the brown rat Rattus norvegicus