How does anterior cruciate ligament reconstruction affect the functioning of the brain and spinal cord?A systematic review with meta-analysis
2021-03-19KzndrRodriguezRinnPlmieriSmithChndrmouliKrishnn
Kzndr M.Rodriguez,Rinn M.Plmieri-Smith,b,Chndrmouli Krishnn,c,d,e,*
a School of Kinesiology,University of Michigan,Ann Arbor,MI 48109,USA
b Department of Orthopaedic Surgery,Michigan Medicine,Ann Arbor,MI 48109,USA
c Department of Physical Medicine and Rehabilitation,Michigan Medicine,Ann Arbor,MI 48108,USA
d Biomedical Engineering,University of Michigan,Ann Arbor,MI 48109,USA
e Michigan Robotics Institute,University of Michigan,Ann Arbor,MI 48109,USA
Abstract
Keywords: ACLR;Cortical excitability;H-reflex;Transcranial magnetic stimulation;TMS
1. Introduction
More than 250,000 people suffer from an anterior cruciate ligament (ACL) injury each year, resulting in more than 150,000 ACL reconstruction procedures annually.1Despite the goal to restore quadriceps strength and function during rehabilitation, many individuals continue to present with lingering quadriceps deficits for months to years after surgery.2,3This persistent quadriceps weakness has been associated with abnormal knee biomechanics, poor patient-reported function,decreased functional performance, and increased risk of reinjury in individuals with ACL reconstruction.4-12Furthermore, quadriceps weakness has been linked to an increased risk for ACL re-injury11and early-onset post-traumatic osteoarthritis.13Thus, understanding the factors that contribute to chronic quadriceps weakness is critical to prevent re-injury and support long-term joint health after ACL reconstruction.
Incomplete voluntary activation (i.e., the inability to activate the quadriceps muscle completely during a contraction)is a commonly attributed source of quadriceps weakness after ACL reconstruction.13Incomplete voluntary activation can occur due to submaximal recruitment of the motor units within the quadriceps muscle and/or due to suboptimal firing of the recruited motor units.14Indeed, diminished voluntary activation is well documented in the literature for both the reconstructed and the non-reconstructed legs relative to healthy control legs (i.e., legs of the uninjured control group participants), and this bilateral inhibition has been attributed to the observed bilateral weakness after unilateral ACL injury and reconstruction.15Proposed sources of voluntary activation deficits include peripheral factors,such as pain,16joint effusion,17and abnormal afferent feedback from the mechanoreceptors.18,19Recent evidence also points to the contributions of neural alterations that occur following ACL reconstruction.For example, alterations in spinal-reflex and corticospinal excitability have been reported following ACL injury and reconstruction,20-26and these alterations have been associated with quadriceps weakness after ACL reconstruction.
Spinal-reflex excitability is typically measured using the quadriceps Hoffmann reflex(H-reflex),which provides an estimate of the proportion of the motor-neuron pool that can be reflexively activated.27The H-reflex can be influenced by both pre- and post-synaptic pathways,27and decreased H-reflex excitability is considered to contribute to poor quadriceps voluntary activation after ACL injury or surgery.28However, the magnitude and direction for spinal-reflex changes remain unclear, as studies have reported conflicting results,23-26which may limit the ability to design appropriate interventions to target quadriceps inhibition after ACL reconstruction.Thus,a better understanding of the alterations in spinal-reflex pathways is crucial to combat quadriceps weakness after ACL reconstruction.
The excitability of the corticospinal pathways is typically evaluated using the size of the motor evoked potentials(MEPs) elicited via transcranial magnetic stimulation (TMS)and the minimum TMS intensity required to produce a pre-defined MEP(i.e.,motor threshold). Following injury and surgery,changes in neurophysiology associated with lost ACL mechanoreceptors29and other peripheral (e.g., pain and effusion) and spinal factors could influence the excitability of the corticospinal pathways. Consequently, the disrupted corticospinal pathways may suppress the neural drive to the quadriceps muscle and induce quadriceps weakness and activation failure.24Although decreased MEPs and increased motor threshold are reported in individuals with ACL injury and reconstruction,21,22these studies also present conflicting findings.20,23-25,30-33Thus, similar to spinal-reflex excitability, it remains unclear whether the excitability of the corticospinal pathways is altered after ACL reconstruction.
Therefore,the primary purpose of this study was to systematically review the current research related to alterations of spinal-reflex and corticospinal excitability following ACL reconstruction and perform a meta-analysis to gain a better understanding of the magnitude and direction of changes in spinal-reflex and corticospinal excitability of the quadriceps muscle. A secondary purpose was to evaluate the extent of quadriceps weakness and activation failure in this population.We hypothesized that individuals with ACL reconstruction will demonstrate a decrease in spinal-reflex (H-reflex to muscle response(H:M)ratio)and corticospinal excitability(motor threshold, MEP), which will be paralleled by a decrease in quadriceps strength and voluntary activation.
2. Methods
2.1. Identification and selection of studies
Based on guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement,34a comprehensive search of the published literature was performed on the following electronic databases: (1) MEDLINE via PubMed, (2) EMBASE, (3) Web of Science Core Collection, and (4) the Cochrane Library. Permutations of the text keyword combinations for the search included the following: “anterior cruciate ligament”, “anterior cruciate ligament injury”, “anterior cruciate ligament reconstruction”, “anterior cruciate ligament surgery”, and their respective abbreviations,along with the terms “quadriceps”, “knee”, and “muscle”.These terms were then combined with terms associated with neural alterations, such as “cortical excitability”, “neural excitability”, “corticospinal excitability”, “H-reflex”,“Hoffmann reflex”, “spinal reflex”, “spinal excitability”,“transcranial magnetic stimulation”, “TMS”, “motor threshold”, “motor evoked potential”, “MEP”, and “H:M ratio”.Paper references yielded from the computerized search were manually inspected to identify other potential studies that fit our inclusion criteria.All databases were searched for relevant articles up until January 13,2020.
2.2. Inclusion and exclusion criteria
Studies were examined by 2 independent reviewers to determine eligibility and to appraise methodological quality.This meta-analysis included relevant articles that were (1)original investigations related to individuals with unilateral ACL reconstruction; (2) cross-sectional and prospective casecontrol studies measuring at least one of the following variables in the quadriceps muscle: H:M ratio, MEP, or motor threshold; and (3) written in English. Case studies or case series, conference abstracts or presentations, studies that focused on other lower leg injuries and variables, or studies that failed to meet inclusion criteria (e.g., literature reviews,articles not available in English) were excluded. Intervention studies were included only if pre-intervention data were available. An initial screening was used to determine inclusion based on title and abstract.If the abstract provided insufficient information,researchers read full-length articles to finalize eligibility. The reference lists of all included articles were also manually surveyed for relevant articles.
2.3. Assessment of methodological quality and risk of bias across eligible studies
The National Institutes of Health(NIH)Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies was used to examine the methodological quality of all included studies. The assessment tool included 14 questions shown in Supplementary Table 1.Responses(yes/no/not reported(NR)/not applicable(NA))to these questions were determined based on whether or not the study met the recommended quality criteria.A score of 1 was given for“yes”and 0 for“no”.In addition, not reported items were marked by NR and not applicable items were marked by NA. The quality assessment was performed by 1 reviewer and confirmed by a 2nd reviewer. The NIH assessment tool was scored based on the total number of questions relevant to the study; thus, totals may vary.In addition,funnel plots and Egger’s test were used to examine the publication bias for the outcome variables.35
2.4. Data extraction and analysis
A data extraction sheet was developed to summarize the following variables: (1) sample size, (2) age, (3) height, (4)weight, (5) time since surgery, (6) self-reported activity level(Tegner Activity Score),36(7) self-reported knee function(International Knee Documentation Committee Questionnaire),37and (8) neuromuscular parameters (H:M ratio, motor threshold, MEP, knee strength, and voluntary activation).When insufficient information was provided on subject demographics and measure-related parameters, the corresponding author for the study was contacted.
2.5. Statistical analysis
Descriptive statistics for all demographic and neuromuscular variables were computed and tabulated for both the ACL and control groups (Table 1). The following equations were used to calculate between-group pooled standard deviation Eq.(1)and effect size Eq.(2):38-40

The standard error of the effect size for between-group analysis Eq. (3) was calculated using the following equation:38-40

The following equations were used to calculate between-leg(ACL-reconstructed (ACL-R) vs. ACL-non-reconstructed(ACL-NR) leg) pooled standard deviation Eq. (4) and effect size Eq.(5),assuming a modest correlation of 0.5:38-40
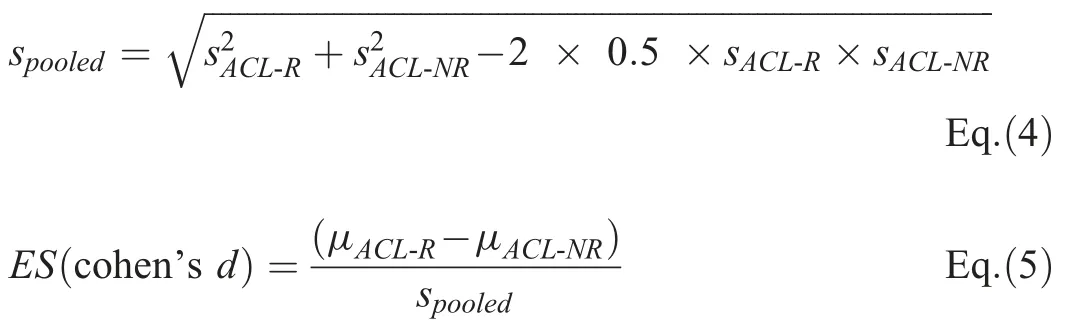
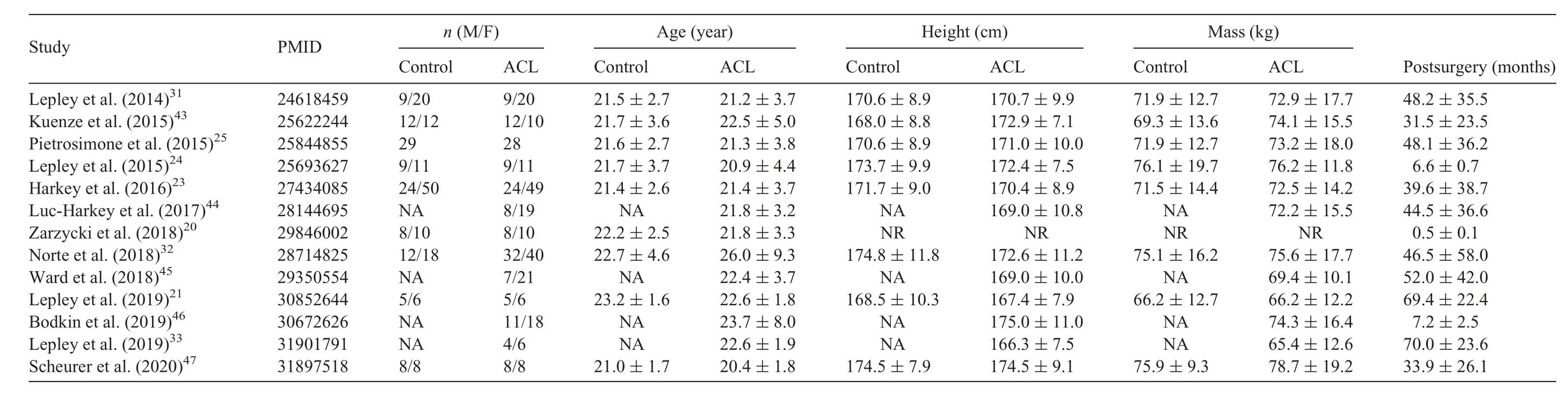
Table 1 Study characteristics and participant demographics for all included studies.
The standard error of the effect size for between-leg analysis Eq.(6)was calculated using the following equation:38

Standardized mean difference (SMD) meta-analyses were performed for H:M ratio, motor threshold (% maximum stimulator output (%MSO)), MEP, knee extensor strength, and voluntary activation (central activation ratio(CAR)) using the JASP software program (Version 0.11.1.0; JASP-Stats, Amsterdam, the Netherlands). SMD meta-analyses were performed to quantify (1) reconstructed and non-reconstructed leg differences, (2) reconstructed and healthy control leg differences, and (3) non-reconstructed and healthy control leg differences.38,39A randomeffects model was selected to improve generalizability, as eligible studies varied in participant demographics and variables collected.40A Wald’s test was utilized to determine between-group (ACL reconstructed vs. healthy controls)and within-group (reconstructed vs. non-reconstructed leg)differences for all variables. Forest plots were created for all variables to determine SMDs and 95% confidence intervals (95%CIs) of the between-group and within-group differences. I2statistics was used to assess heterogeneity between the studies. The I2values of <40% is considered to be not important and 50%-90% represent substantial heterogeneity.41
3. Results
3.1. Literature search,study selection,and study characteristics
Our comprehensive search identified 337 articles.A total of 213 studies were assessed after removal of duplicate studies.After screening the titles and abstracts,17 articles were further evaluated for inclusion criteria. A total of 13 studies met our eligibility criteria.A total of 10 studies reported H:M ratio,12 studies reported motor threshold, 6 studies reported MEPs(Table 2),9 studies reported quadriceps strength,and 9 studies reported voluntary activation (Supplementary Table 2). Subject characteristics and descriptive data for each study are outlined in Table 1.A PRISMA flowchart for the literature search and selection is shown in Fig.1.
3.2. Study quality and risk of bias
The methodological quality of the studies ranged from a score of from 5 to 8 (maximum possible 11) (Supplementary Table 1).Visual inspection of the funnel plots indicated minimal publication bias for the variables included in the analysis(Supplementary Figs. 1-5). The Egger’s test indicated a significant publication bias for MEP when comparing the reconstructed and non-reconstructed legs(p <0.001)and for motor threshold when comparing the reconstructed and healthy control legs (p=0.024). All remaining analyses indicated no significant publication bias(all p >0.05).

Table 2 Primary outcome variables(H:M ratio,motor threshold,and motor evoked potential)of included studies(mean±SD).

Fig. 1. A schematic of PRISMA flow diagram of the identification and selection of the studies included in this meta-analysis. ACL=anterior cruciate ligament;ACLR=ACL reconstruction; H:M ratio=Hoffmann reflex to muscle response ratio; MEP=motor evoked potential; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses;TMS=transcranial magnetic stimulation.
3.3. Primary variables
3.3.1. Spinal-reflex excitability(H:M ratio)
A total of 10 studies with a cumulative sample size of 330 were included in the between-leg analysis (I2=0.017%,p=0.407). A total of 8 studies with a cumulative sample size of 508 were included in the between-group analysis of the ACL reconstructed leg and healthy control leg (I2=18.063%,p=0.153). A total of 8 studies with a cumulative sample size of 508 were included in the between-group analysis of the ACL non-reconstructed leg and healthy control leg(I2=0.007%,p=0.306)(Table 2).All studies evaluated the H:M ratio of the vastus medialis muscle using standardized procedures. Our meta-analysis indicated a significant increase in H:M ratio for both the reconstructed leg(SMD=0.28,95%CI:0.08-0.49, p=0.006) and the non-reconstructed leg(SMD=0.22, 95%CI: 0.04-0.40, p=0.016) when compared with the healthy control leg.However,we found no significant differences when comparing the reconstructed leg relative to the non-reconstructed leg (SMD=0.10, 95%CI: -0.01 to 0.21,p=0.078)(Fig.2).
3.3.2. Corticospinal excitability(motor threshold)
A total of 11 studies with a cumulative sample size of 304 were included in the between-leg analysis (I2= 24.033%,p=0.085). A total of 8 studies with a cumulative sample size of 403 were included in the between-group analysis of the ACL reconstructed leg and healthy control leg(I2= 63.445%, p=0.005). A total of 7 studies with a cumulative sample size of 371 were included in the between-group analysis of the non-reconstructed leg and healthy control leg(I2= 77.393%, p <0.001) (Table 2). All studies evaluated the motor threshold of the vastus medialis muscle using the Magstim device. Our meta-analysis indicated a significant increase in motor threshold of the reconstructed leg when compared with the non-reconstructed leg (SMD=0.20,95%CI: 0.06-0.34, p=0.005). In addition, significant increases in motor threshold were observed for both the reconstructed and non-reconstructed legs when compared with the healthy control leg (SMD=0.76,95%CI: 0.40-1.12,p <0.001 and SMD=0.47, 95%CI: 0.00-0.95, p=0.049,respectively)(Fig.3).

Fig.2. Forest plot depicting the pooled standardized mean difference(95%confidence intervals(lower limit to upper limit))of the quadriceps H:M ratio between the (A) reconstructed leg and the non-reconstructed leg, (B) reconstructed leg and the healthy control leg, and (C) non-reconstructed leg and the healthy control leg.Note that there was a significant increase in the H:M ratio of the reconstructed and non-reconstructed legs when compared with the healthy control leg and a non-significant increase in the H:M ratio of the reconstructed leg when compared with the non-reconstructed leg.H:M ratio=Hoffmann reflex to muscle response ratio.
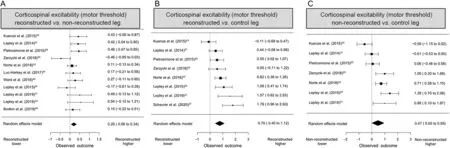
Fig. 3. Forest plot depicting the pooled standardized mean difference (95% confidence intervals (lower limit to upper limit)) of the quadriceps motor threshold between the(A)reconstructed leg and the non-reconstructed leg,(B)reconstructed leg and the healthy control leg,and(C)non-reconstructed leg and the healthy control leg.Note that there were significant increases in the motor threshold of both the reconstructed and non-reconstructed legs when compared with the healthy control leg and of the reconstructed leg when compared with the non-reconstructed leg.
3.3.3. Corticospinal excitability(MEP)
A total of 6 studies with a cumulative sample size of 115 were included in the between-leg analysis (I2=80.637%,p <0.001).A total of 3 studies with a cumulative sample size of 166 were included in the between-group analysis of the ACL reconstructed leg and healthy control leg (I2=81.009%,p <0.001).A total of 3 studies with a cumulative sample size of 108 were included in the between-group analysis of the non-reconstructed leg and healthy control leg (I2=0.000%,p=0.434) (Table 2). All studies measured the MEP of the vastus medialis at 120%of motor threshold using the Magstim device. Our meta-analysis indicated no significant betweenleg (SMD=-0.08, 95%CI: -0.54 to 0.38, p=0.741) or between-group differences (reconstructed vs. healthy control leg:SMD=0.14,95%CI:-0.82 to 1.11,p=0.772;non-reconstructed vs.healthy control leg:SMD=0.30,95%CI:-0.10 to 0.70,p=0.140)in MEPs of the quadriceps muscle (Fig.4).
3.4. Secondary variables
3.4.1. Quadriceps strength
A total of 8 studies with a cumulative sample size of 227 were included in the between-leg analysis (I2=54.024%,p=0.019). A total of 7 studies with a cumulative sample size of 357 were included in the between-group analysis of the ACL reconstructed leg and healthy control leg (I2=38.225%,p=0.091). A total of 6 studies with a cumulative sample size of 300 were included in the between-group analysis of the non-reconstructed leg and healthy control leg (I2=37.955%,p=0.078)(Supplementary Table 2).All studies reported maximum voluntary contraction force normalized to the subject’s body mass(i.e.,N·m/kg).Our meta-analysis indicated a significant reduction in quadriceps strength of the reconstructed leg when compared with the non-reconstructed leg(SMD=-0.54,95%CI: -0.76 to -0.32, p <0.001). In addition, we found a significant reduction in quadriceps strength of both the reconstructed and non-reconstructed legs when compared with the healthy control leg (SMD=-0.78, 95%CI: -1.07 to -0.49,p < 0.001 and SMD=-0.32, 95%CI: -0.63 to -0.01,p=0.042,respectively)(Supplementary Fig.6).
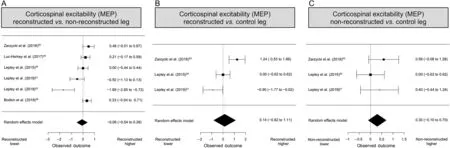
Fig.4. Forest plot depicting the pooled standardized mean difference(95%confidence intervals(lower limit to upper limit))of the quadriceps MEP between the(A)reconstructed leg and the non-reconstructed leg,(B)reconstructed leg and the healthy control leg,and(C)non-reconstructed leg and the healthy control leg.Note that there were no between-leg or between-group differences in MEP.MEP=motor evoked potential.
3.4.2. Quadriceps voluntary activation
A total of 9 studies with a cumulative sample size of 315 were included in the between-leg analysis (I2=0.000%,p=0.584). A total of 7 studies with a cumulative sample size of 482 were included in the between-group analysis of the ACL reconstructed and healthy control leg (I2=30.895%,p=0.041). A total of 7 studies with a cumulative sample size of 482 were included in the between-group analysis of the ACL non-reconstructed and healthy control leg(I2=50.634%,p=0.025)(Supplementary Table 2).All studies evaluated voluntary activation of the quadriceps muscle using the central activation ratio derived from the burst superimposition technique.42Our meta-analysis indicated a significant reduction in quadriceps voluntary activation of the reconstructed leg when compared with the non-reconstructed leg (SMD=-0.12,95%CI: -0.23 to 0.01, p=0.035). We also found significant reductions in quadriceps voluntary activation of both the reconstructed and the non-reconstructed legs when compared with the healthy control leg (SMD=-0.73, 95%CI: -0.97 to-0.50,p <0.001 and SMD=-0.55,95%CI:-0.82 to-0.27,p <0.001,respectively)(Supplementary Fig.7).
4. Discussion
The primary purpose of the current meta-analysis was to evaluate the changes in spinal-reflex and corticospinal excitability of the quadriceps muscle in individuals with ACL reconstruction. The findings of this meta-analysis partially support our initial hypotheses. As hypothesized, ACL-reconstructed individuals exhibited a significant increase in motor threshold of the reconstructed and non-reconstructed legs when compared with the healthy control leg. They also exhibited a significant increase in motor threshold of the reconstructed leg in comparison with the non-reconstructed leg. However, contrary to our hypothesis,no between-leg or between-group differences in MEPs were observed after ACL reconstruction.In addition,a significant increase in the H:M ratio was observed in both the reconstructed and the non-reconstructed leg when compared with the healthy control leg. The changes in spinal-reflex and corticospinal excitability were also paralleled by bilateral reductions in quadriceps strength and voluntary activation of the quadriceps muscle when compared with the healthy control leg.These results suggest that individuals with ACL reconstruction exhibit alterations in both spinal-reflex and corticospinal excitability, and these alterations may contribute to poor quadriceps function after ACL reconstruction.Specifically,there appears to be a significant reduction in the excitability of the corticospinal pathways,which is compensated for by an increased excitability of the spinal-reflex pathways.Thus,the findings underscore the importance of targeting both the spinal-reflex and corticospinal pathways to normalize quadriceps function after ACL injury or reconstruction.
4.1. Spinal-reflex excitability
Spinal-reflex excitability has been extensively studied in individuals with ACL reconstruction.20,21,23-25,31-33,43-47However, the magnitude and the direction of the reflex excitability changes have been inconsistent in the literature. The current meta-analysis indicates a significant bilateral increase in spinal-reflex excitability of the reconstructed and nonreconstructed legs when compared with the healthy control leg. There was also a small increase in spinal-reflex excitability of the reconstructed leg when compared with the nonreconstructed leg; however, this change was not statistically significant. These findings suggest that there is a general increase in spinal-reflex pathways after ACL reconstruction,which could potentially be a compensatory mechanism for reductions in excitability of the corticospinal pathways (see below).25From a clinical perspective, alterations in spinalreflex pathways may likely assist in maintaining(or restoring)the level of neural drive (i.e., voluntary activation) and quadriceps strength after ACL reconstruction.25However,additional high-quality longitudinal studies are needed to determine the exact nature of alterations in spinal-reflex pathways after ACL reconstruction and what impact this may have on quadriceps weakness and muscle inhibition.
4.2. Motor threshold
There is an accumulating body of evidence that suggests that the excitability of the corticospinal pathways are altered after ACL reconstruction.20,21,24,25,31-33,43-47These alterations in corticospinal excitability of the quadriceps muscle have also been linked to poor quadriceps strength and incomplete voluntary activation after ACL reconstruction.46When considering changes in the motor threshold for corticospinal excitability, our meta-analysis indicated a significant increase in the motor threshold for both the reconstructed and nonreconstructed legs compared with healthy control leg. Additionally,significant increases in motor threshold were noted in the reconstructed leg relative to the non-reconstructed leg.These findings were consistent among studies, indicating that bilateral alterations in corticospinal excitability may occur after unilateral injury/surgery. The reductions in corticospinal excitability were also paralleled by bilateral reductions in voluntary activation and quadriceps strength, suggesting that altered corticospinal excitability may contribute to the persistent quadriceps dysfunction after ACL reconstruction.
4.3. MEPs
The current meta-analysis found no significant changes in MEPs of the reconstructed or non-reconstructed legs when compared with the healthy control leg. Furthermore, no changes in MEP were noted for the reconstructed leg when compared with the non-reconstructed leg. The similar MEP values in the ACL group and healthy control group suggest no significant alterations in corticospinal excitability following ACL reconstruction, which is contradictory to the findings on the motor threshold. There are several potential explanations for this observation. First, motor threshold and MEP amplitudes measure different dimensions of corticospinal excitability. Motor threshold is considered an estimate for the excitability of the pyramidal cell membrane, whereas MEP amplitude corresponds to the magnitude of stimulus transmission through the corticospinal tract.48Hence, our results indicate that a greater stimulus is required to excite pyramidal cells, but the extent to which the stimulus is transmitted is unchanged.A second explanation is that MEPs in the included studies were measured at a set percentage of motor threshold(typically 120% of active motor threshold). This would mean that the intensity of the stimulator was adjusted to induce a similar amount of MEP between legs and groups,which could have resulted in a lack of significant differences between legs or groups. This is indeed supported by the observation of higher motor threshold in both the reconstructed and the nonreconstructed legs when compared with the control group.Another possible explanation is related to low statistical power due to the limited number of studies that were included in the MEP meta-analysis and the extent of variability in the observed study results. Unfortunately, there were only 3-6 studies that were included in the MEP meta-analysis,and there was significant heterogeneity in the observed effect sizes between studies. Thus, additional high-quality research examining motor evoked responses following ACL reconstruction is critical for drawing definitive conclusions regarding changes in MEPs after ACL reconstruction.
4.4. Quadriceps strength and voluntary activation
Quadriceps strength and voluntary activation are significant predictors of knee joint health and function after ACL reconstruction. Previous systematic reviews and meta-analyses have shown that quadriceps weakness and voluntary activation failure are common in individuals with ACL reconstruction and are often observed bilaterally after the surgery.15,49Although it was not the primary intent of this meta-analysis,our results of bilateral quadriceps weakness and voluntary activation deficits corroborate these findings and highlight the importance of restoring these deficits optimally soon after the surgery. A key barrier to the development of new interventions that focus on restoring quadriceps function is that the sources of these deficits are currently not clear. Based on the results of our study and prior research investigating the relationship between quadriceps strength,voluntary activation,and the excitability of the spinalreflex and corticospinal pathways, there appears to be some association between these variables.However,due to the crosssectional nature of most studies,the causal relationship between corticospinal and spinal-reflex excitability and quadriceps function could not be established.Future studies that longitudinally examine the contribution of the excitability of corticospinal and spinal-reflex pathways to quadriceps dysfunction after ACL reconstruction may shed more light on this issue.
4.5. Limitations
A key limitation to our study is that there were only a limited number of studies that were included in this meta-analysis.As a result, some of the variables could have been underpowered to determine statistical significance. Furthermore, not all studies examined all outcomes of corticospinal excitability, spinalreflex excitability,quadriceps strength,and voluntary activation.Hence, we were unable to examine the relationship between these variables,which may be interesting to the ACL rehabilitation community.Another limitation is that the participant characteristics and time since surgery varied among the studies,which could have affected the pooled estimate of the effect(i.e.,SMD). However, our pooled SMD is conservative, since we accounted for this issue using a random-effects model. Moreover, we ran a sub-group analysis including only studies with participants greater than 2 years post-reconstruction to address this limitation and observed results that were similar to our overall study findings (Supplementary Table 3). Finally, the conclusions regarding reduced corticospinal excitability changes were primarily derived from the motor threshold variable.It is to be noted that the magnitude of the motor threshold may not be the best indicator of corticospinal excitability because it can be influenced by various factors,such as the skull thickness, the orientation of the corticospinal tract, and the amount of background contraction used during the testing.50,51While there are no reasons to believe that the skull thickness and the orientation of the corticospinal tract would have differed(at a group level) between the ACL reconstructed population and the healthy control population, the amount of background contraction could likely have differed between the groups.This is because the magnitude of the motor threshold is commonly established by having participants perform a slight background contraction of the quadriceps muscle(5%-10%of maximum),and any weakness in the quadriceps muscle will result in an underestimation of maximum voluntary force. Thus, the motor threshold may have been established in participants with ACL reconstruction at a lower background contraction(i.e., absolute force),which could have resulted in the requirement of greater TMS intensity to elicit MEPs (i.e., motor threshold).However,the observed consistency in results between studies that have used active motor threshold20,21and resting motor threshold20suggests that this may not be the case. Future studies should evaluate the effect of different types of standardization of background contraction on motor cortical excitability to determine the best procedure to evaluate corticospinal excitability after ACL reconstruction.
5. Conclusion
This meta-analysis provides valuable insight regarding the alterations in the excitability of the spinal-reflex and corticospinal pathways after ACL reconstruction.The results indicate that there are bilateral reductions in the excitability of the corticospinal pathways(as evaluated by the motor threshold).On the contrary, the excitability of the spinal-reflex pathways was bilaterally increased after ACL reconstruction. These results were paralleled by significant reductions in quadriceps strength and voluntary activation of both the reconstructed and the nonreconstructed legs in comparison with the healthy control leg.Taken together,these findings suggest that alterations in corticospinal and spinal-reflex pathways could influence quadriceps dysfunction after ACL reconstruction;however, the exact relationship between these variables is not clear from our study.Further studies that longitudinally examine the corticospinal and spinal-reflex excitability of the quadriceps muscle and its relationship to quadriceps strength and voluntary activation are needed to fully understand the contribution of these pathways to quadriceps dysfunction after ACL reconstruction.
Acknowledgments
Supported in part by the National Institutes of Health(Grant No. R21-HD092614). The authors thank Dr Aviroop Dutt-Mazumder, Ms Aastha Dharia, and Ms Amanda Vogel for their help in the initial data synthesis.
Authors’contributions
KMR participated in data acquisition, quality rating of the papers, analysis and interpretation of data, and writing of the manuscript; RMPS conceived conception and study design,analyzed, interpreted the data, and critically reviewed and edited the manuscript;CK conceived the study and its design,assisted with data acquisition, supervised data collection and analysis, rated the quality of the included studies, statistically analyzed and interpreted the data,and assisted in writing,critically reviewing, and editing the manuscript. All authors have read and approved the final version of the manuscript, and agree with the order of the presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2020.07.005.
杂志排行

Journal of Sport and Health Science的其它文章
- Factors associated with concussion-symptom knowledge and attitudes toward concussion care seeking in a national survey of parents of middle-school children in the US
- Effects of purposeful soccer heading on circulating small extracellular vesicle concentration and cargo
- The diagnostic and prognostic utility of the dual-task tandem gait test for pediatric concussion
- Impaired eye tracking is associated with symptom severity but not dynamic postural control in adolescents following concussion
- Slowed driving-reaction time following concussion-symptom resolution
- Impaired motor control after sport-related concussion could increase risk for musculoskeletal injury:Implications for clinical management and rehabilitation