Screening colonoscopy: The present and the future
2021-02-04ChelseaHaymanDineshVyas
Chelsea V Hayman, Dinesh Vyas
Abstract In the United States, colorectal cancer (CRC) is the second leading cause of mortality in men and women. We are now seeing an increasing number of patients with advanced-stage diagnosis and mortality from colorectal cancer before 50 years of age, which requires earlier screening. With the increasing need for CRC screening through colonoscopy, and thus endoscopists, easier and simpler techniques are needed to train proficient endoscopists. The most widely used approach by endoscopists is air insufflation colonoscopy, where air distends the colon to allow visualization of the colonic mucosa. This technique is uncomfortable for patients and requires an anesthetist to administer sedation. In addition, patients commonly complain about discomfort post-op as air escapes into the small bowel and cannot be adequately removed. Current research into the use of water insufflation colonoscopies has proved promising in reducing the need for sedation, decreasing discomfort, and increasing the visibility of the colonic mucosa. Future direction into water insufflation colonoscopies which have shown to be simpler and easier to teach may increase the number of proficient endoscopists in training to serve our aging population.
Key Words: Colorectal cancer; Water-insufflation colonoscopy; Air-insufflation colonoscopy; Adenomatous polyps; Adenoma detection rate
INTRODUCTION
In the United States, colorectal cancer (CRC) is the second leading cause of mortality in men and women. The most effective tool for reducing the morbidity and mortality associated with CRC is the use of colonoscopy. With nearly 14.2 million procedures performed in the United States alone[1], the colonoscopy is one of the most common procedures performed. However, colonoscopies can only benefit the population with endoscopists who have proficiency in both technical and cognitive skills. The guidelines for training in colonoscopy techniques and grading proficiency continue to evolve as new advances in the tools used by endoscopists are discovered. In the 1960s, retrograde colonoscopy and endoscopic excision of polyps were developed in Japan to advance the visualization and removal of polyps from the entire large intestine[2]. Previous techniques such as the barium enema were challenging without considerable training and practice, and the presence of polypoid tumors could not be reliably excluded. As it was demonstrated that CRC did not occurde-novobut arose from a premalignant polyp, the use of the colonoscopy as a screening technique increased. Research into the use of the colonoscopy and the colonoscopy polypectomy proved that the detection of cancer at an earlier, pre-symptomatic stage was associated with better survival[3].
For a successful screening colonoscopy, partial distention of the lumen is needed to allow proper visualization and inspection of the colonic mucosa. The current standard technique for colonic distention is the use of air insufflation (AI) using an integrated air pump[4,5]. However, one of the major sources of pain and discomfort for patients undergoing a colonoscopy is the volume of air insufflated which causes significant abdominal distention and looping of the instrument. Potential risks for this procedure include perforation, bleeding, and infection. To minimize discomfort and pain during the procedure, patients undergoing colonoscopy with AI often require sedation which adds additional risks including medication side effects, higher medical costs, and longer recovery time when compared with unsedated colonoscopy[6]. At the end of the procedure, the air can only be partially removed, as some of it escapes into the small bowel. This leads to post-procedure cramping, gas, and bloating which can only be relieved by passing gas.
Recent clinical trials have proposed that using water infusion to distend the colon may reduce patient pain and discomfort and improve colonic visualization through difficult segments of the colon. This was first described by Falchuk and Griffin in 1984 in patients who could not undergo AI due to severe diverticular disease[7]. For water infusion colonoscopy, instead of expanding the colon, the water weighs it down utilizing gravity. It was Japanese endoscopists who evolved this technique by using syringes for water infusion and complete air suction to “collapse” the colonic lumen and continuously infusing water to advance the colonoscope[8]. This method straightens the colon and allows for better navigation of the scope through less extreme angles. As no air is left behind, this technique reduces post-procedure pain and allows for faster recovery. The first randomized control trial in 2010 showed that using the water immersion technique compared to standard AI increases the success rate of minimal sedation colonoscopy[9]. This along with other studies has shown the use of water improves the rate and time of cecal intubation, alleviates abdominal pain, and increases patients’ willingness to undergo a repeat procedure[7]. This technique is shown in Figure 1.
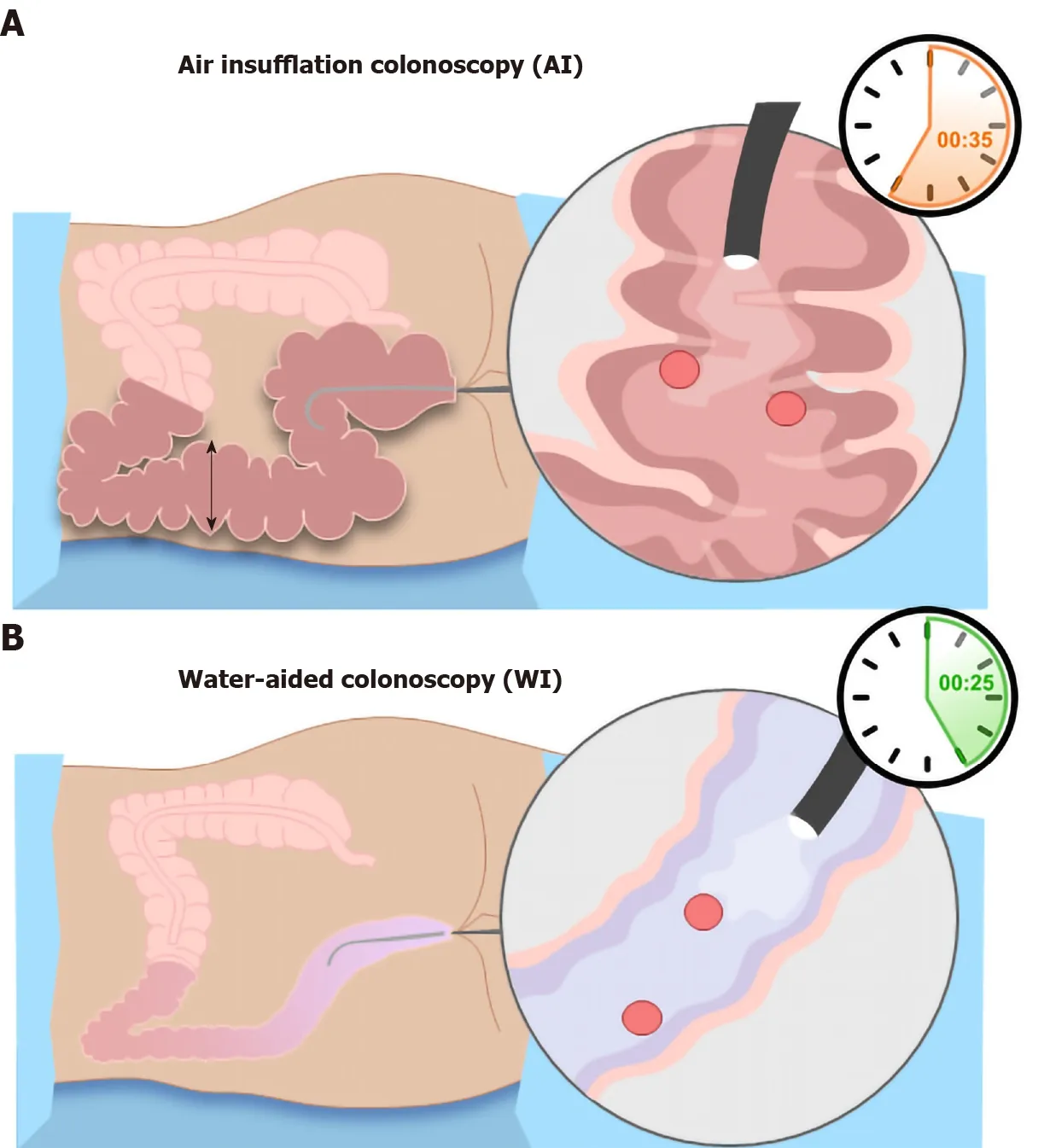
Figure 1 Image of colonic distension and bowel looping in air insufflation colonoscopy vs water-aided colonoscopy. A: Air insufflation colonoscopy causes significant distention of the colon in both length and width. The air promotes looping of the bowl at the flexure points leading to difficult navigation of the colonoscope; B: Water insufflation utilizes gravity to pull the colon down while providing minimal distention and looping. AI: Air insufflation; WI: Water insufflation.
The overall effectiveness of colonoscopy is the achievement of various quality measurements. The most important quality measurement is the adenoma detection rate (ADR) which is the frequency with which adenomas are detected in asymptomatic, average-risk individuals in a screening colonoscopy[10]. Another quality measurement is cecal intubation or the ability to pass the colonoscope through the tip of the ileocecal valve. This ensures adequate visualization of the entire colonic mucosa. Bowel preparation is an important measure as its effectiveness rests in the hands of the patient. Without adequate bowel preparation, clear visualization of the colon is difficult and may require repeat procedures. Sedation and the use of an anesthetist decrease intra-op and post-op pain, yet it is associated with increased cost.
New advances in colonoscopy have led to the development of virtual colonoscopy and robotic colonoscopy. Virtual colonoscopies, or computed tomography colonography (CTC), use helical CT scanners and AI to take 3D images of the colon. This technique is non-invasive, requires no sedation, can be completed in 10-15 min, and is overall much safer[11]. However, there are some limitations to this approach. Incomplete distention of colonic segments and flat lesions can lead to false-negative diagnoses. In addition, CTC does not allow for removal or biopsy of lesions. Robotic colonoscopy has benefits over the traditional endoscope approach including better viewing of the gastrointestinal tract, decreased pain, and the ability to navigate tortuous colons successfully. Multiple models of robotic instruments are currently being studied including robotic capsules and robotically controlled advanced colonoscopies. These new advances and the ease with which they can be used may aid in the training of future endoscopists. New research shows that training residents in water insufflation colonoscopic technique leads to increased patient comfort and decreased complications with comparable success rates[12]. As the number of people needing screening colonoscopies continues to grow, so will the need for competent endoscopists and successful endoscopic techniques.
ADR
ADR is the proportion of screening colonoscopies that detect at least one adenoma[13]. The goal of endoscopic screening is checking for CRC, so detection of adenoma in the large bowel can limit the advancement to larger adenomas. The recommended ADR is 20%, based on studies that showed adenoma prevalence in asymptomatic adults to be between 25% to 40%[14,15]. In a study with over 10000 patients, the overall ADR (95% confidence interval) for water insufflation was 34.4% and 30.2% for AI[16]. ADRs are inversely correlated with interval cancers which makes them an important measure in colonoscopies. Interval cancers, or post-colonoscopy CRCs, are cancers detected within the surveillance interval, or 6-36 mo post-cleared colonoscopy. The incidence of interval cancers is 3.4%-9.2%, and improving ADR and colonoscopy techniques can decrease this number substantially[17].
CECAL INTUBATION
Cecal intubation is successfully achieved when the tip of the colonoscope is passed through the ileocecal valve into the caput. This allows for a complete examination of the colonic mucosa at the medial wall of the cecum. AI distends the length of the colon, often farther than the length of the colonoscope. This attributes to the difficulty of adequate cecal intubation with AIC. Gravity allows water infusion into the sigmoid colon to open a passage through the loops and bends of the colon. In addition, abdominal compression and proper positioning of the patient facilitates the passage of the colonoscope and enhances cecal intubation. Some studies have reported that warm water insulation reduces colonic spasms which may also contribute to a higher cecal intubation rate. Some studies have shown that WIC improved cecal intubation time compared with AIC[7,18]. Increasing cecal intubation time can decrease the total OR time and thus, decrease the overall cost.
BOWEL PREP QUALITY
In order to optimize the effectiveness of colonoscopy as a screening tool, patients need to accept the procedure and the necessity of adequate bowel preparation[19]. Preparation quality affects the mucosal visualization, the ability to complete the exam, and the procedure duration. Only three-quarters of colonoscopies have adequate colon preparation[20]. Poor bowel prep can lead to lower ADRs and may force patients to undergo follow-up colonoscopies sooner. In water insufflation (WI), the suction of dirty water and infusion of clean water in the colonic lumen provides serendipitously salvage bowel cleaning in patients with suboptimal bowel preparation[21]. Ineffective bowel preparation may lead to cancelations or rescheduling procedures, which is a major contributor to costs[22].
SEDATION
Sedation for colonoscopy procedure increases the cost and post-procedure recovery time for patients. Patients who have more challenging anatomy often require more sedation as they experience more pain. Studies have shown that water exchange has minimized the requirement for sedation compared with AI. In one study, only 11.5% of patients required on-demand sedation with water exchange compared with 26% in the AI group[23]. Another benefit of limiting sedation is to decrease the risk of cardiopulmonary complications associated with anesthesia. In a study that used the Clinical Outcomes Research Initiative database, cardiopulmonary complications occurred in 0.9% of procedures and made up 67% of unplanned events in endoscopic procedures with sedation[24]. Patients with increased risk of CVP complications include those with advanced age and presence of comorbidities. These patients could benefit greatly from water insufflation colonoscopy, which requires little if any, pain management.
LIMITING PRE AND POST-PROCEDURE PAIN
Intraoperatively, AI causes more pain during colonoscopy as it elongates and distends the colon. Post-operatively, patients experience discomfort as the gas escapes the colon into the small bowel and leads to abdominal distention. Water insufflation reduces intraoperative pain by weighing down and straightening the sigmoid and decreasing colonic spasm[25]. Fewer patients require sedation with water insufflation compared with AI[26]. Several studies revealed that WIC significantly increased the number of patients who were willing to undergo another colonoscopy due to limited pain during the procedure; this was found to be significantly higher in WIC than in AIC[18,27,28]. With AI, undesired outcomes including perforation and bleeding are partly due to increased colonic distention, angulations exaggeration at flexures, and the increased looping of the instrument. The current rate of perforation is low, ranging from 0.08% to 0.3% in various studies[29]. Pain during colonoscopy indicates the risk of perforation, but sedation can mask this important warning[30]. WI colonoscopy minimizes colonic distention, improves visibility, and reduces the need for sedation, thus reducing the risk of perforation.
TEACHING ENDOSCOPY TECHNIQUES IN TRAINING PROGRAMS
There are multiple different methods currently used for colonoscopy training, including mechanical simulators, virtual reality simulators, computer-simulating endoscopy, magnetic endoscopic imaging, and composite and explanted animal organ simulators. One of the main factors that leads to a lack of polyp discovery is the inexperience of the endoscopist[30,31]. However, there have been some limitations to colonoscopy instruction, including time management and potential trauma to patients involved. Endoscopists in training may benefit from learning the water insufflation technique, as the scope becomes easier to navigate through a minimally looped colon. In addition, detorsion becomes easier for trainees with water insufflation as there is a decreased risk of perforation from AI. Studies have shown that WIC has significantly shorter cecal intubation time for endoscopists in training compared with AIC[7]. The increasing need for colonoscopy screening has increased the demand for high-quality training. Stimulation models are a key tool that many programs use to ease the learning curve of colonoscopy techniques. Another tool that should be introduced into training programs is the use of water insufflation colonoscopy. Trainees may benefit from training with the water insufflation technique as there is the ease of insertion, reduced cecal intubation time, more comfort for the patient, and less looping of the bowel[12]. The strengths and weaknesses of these two techniques are shown in Table 1.
CONCLUSION
Colorectal cancer is the second leading cause of mortality in men and women in the United States. Since the onset of screening colonoscopies, the conventional colonoscope has not changed much since its development. Many colonoscopy practices use deep sedation to provide comfort for the patients, which adds to the overall cost of the procedure. There is still a lack of widespread acceptance of the use of colonoscopies (vsother non-invasive screening techniques), as up to 75% of patients diagnosed with colon cancer present with locally advanced disease[32]. In addition, 1 in 10 patients has developed interval cancers after clear colonoscopies. Beyond the water insufflation technique, there have been new advances in the use of robotic endoscopic techniques for screening colonoscopies. These devices can give a more in-depth view of the gastrointestinal tract, decrease pain associated with endoscopy, and perform well in more challenging colons[33]. Future directions should aim at getting a true 360-degree view of the colon with minimal pain, sedation, and total procedure time. In addition, colonoscopy practices should be geared toward practices that can be safely done during the COVID pandemic without the risk of aerosolizing viral particles.
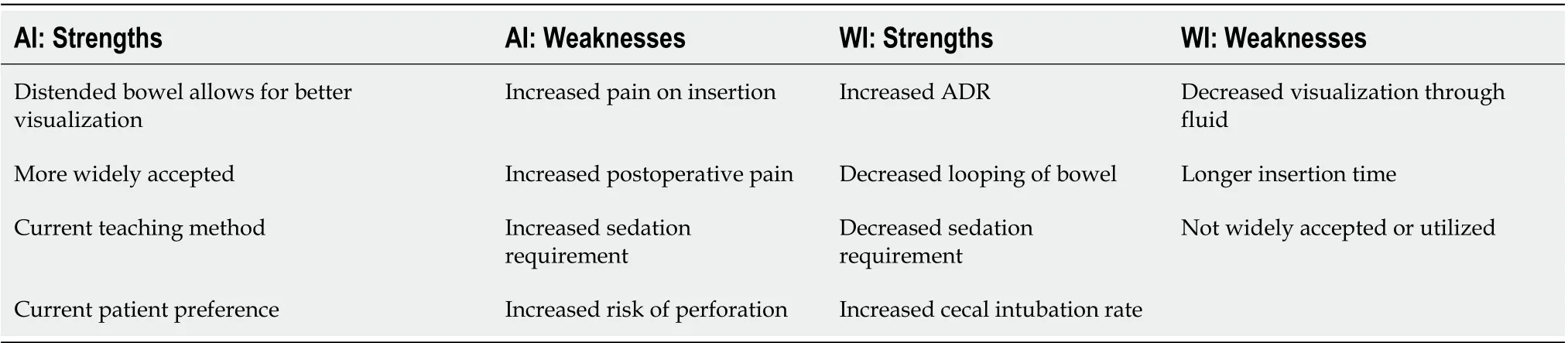
Table 1 Strengths and weaknesses of air insufflation vs water insufflation
杂志排行

World Journal of Gastroenterology的其它文章
- Peritoneal dissemination of pancreatic cancer caused by endoscopic ultrasound-guided fine needle aspiration: A case report and literature review
- Comparative study on artificial intelligence systems for detecting early esophageal squamous cell carcinoma between narrow-band and white-light imaging
- Trends in the management of anorectal melanoma: A multi-institutional retrospective study and review of the world literature
- Serum vitamin D and vitamin-D-binding protein levels in children with chronic hepatitis B
- Circular RNA AKT3 governs malignant behaviors of esophageal cancer cells by sponging miR-17-5p