Morphological changes of the lateral abdominal muscles in adolescent soccer players with low back pain:A prospective cohort study
2020-12-18PwelLinekPrdisNoormohmmdpourMohmmdAliMnsourniTomszWolnyDminSikord
Pwel Linek*,Prdis Noormohmmdpour,Mohmmd Ali Mnsourni,c,Tomsz WolnyDmin Sikord
aDepartment of Kinesitherapy and Special Methods in Physiotherapy,The Jerzy Kukuczka Academy of Physical Education,Katowice,40-065,Poland bSports Medicine Research Center,Neuroscience Institute,Tehran University of Medical Sciences,Tehran,14395-578,Iran cDepartment of Epidemiology and Biostatistics,School of Public Health,Tehran University of Medical Sciences,Tehran,14155-6446,Iran dKinesis Research Team,Department of Kinesitherapy and Special Methods in Physiotherapy,The Jerzy Kukuczka Academy of Physical Education,Katowice,40-065,Poland
Abstract Background:Most papers examining the lateral abdominal muscles(LAMs)and low back pain(LBP)are cross-sectional,with groups of participants being divided into a control and an LBP group.We hypothesized that morphological measurements of the LAMs in adolescent soccer players may predict future LBP incidence.The aim of this study was to examine the associations between the morphology of LAMs and LBP incidence rate among adolescent soccer players.Methods:Ninety-seven adolescent male soccer players with no LBP at baseline were recruited into the prospective cohort study.The thickness of the LAMs was measured at baseline by ultrasound imaging in a supine rest position.Nine cases of LBP occurred during the follow-up 6-month observation.Results:An obliquus internus(OI)asymmetry was related to increasing LBP risk(odds ratio=19.99;95%CI:2.4-167.9).Spearman correlation also showed a linear relationship between OI asymmetry value and duration of LBP(R=0.75,p=0.02).An OI side-to-side difference greater than 1.25mm suggests possible LBP incidence in the 6-month observation among adolescent soccer players.Conclusion:The morphological changes of the OI may be related to LBP's incidence in adolescent soccer players.The presence of OI asymmetry increases the odds of LBP by at least 2.4 times.Hypertrophy of the OI on one side of the body may contribute to trunk muscle imbalance.
Keywords:Abdominal wall;External oblique;Internal oblique;Low back pain;Ultrasound;Transversus abdominis
1.Introduction
In adolescent athletes,the 1-year and lifetime occurrences of low back pain(LBP)were found to be 57%and 66%,respectively;this shows that LBP is a common symptom in adolescent athletes at competitive level.1Soccer is one of the most popular sports in the world,and is intensively cultivated from childhood to middle age.LBP is experienced significantly more often in adolescent soccer players than in non-athletes,with an odds ratio equal to 1.6.2Also,it has been shown that playing soccer is one of the factors associated with adolescent chronic LBP,with an odds ratio equal to 3.07.3
Lateral abdominal muscles(LAMs)play an important role in sports activities,such as kicking and contribute to stabilizing the body.4Thus,researchers have tried to connect morphological changes of the LAMs with LBP in athletes5-7by using ultrasound imaging(USI)or magnetic resonance imaging(MRI).Some studies con firmed asymmetric hypertrophy of the trunk muscles in athletes,8-10which may increase the risk of LBP.9Bearing in mind that most soccer players have a dominant foot for kicking,there is a potential source of LAM sideto-side asymmetry.In adult soccer players,MRI study showed that LAMs were symmetric at all examined levels,10and only the rectus abdominis was an asymmetric muscle.8In a USI study,it was shown that LAM morphology(size)between LBP and no-LBP soccer players was similar,but contraction ability was altered in those with LBP.11All of these studies were conducted only in an adult population and on a relatively small sample size.To date,there has been only 1 study among adolescent soccer players,where no changes in LAM morphology between LBP and no-LBP players was found.12However,the mentioned study was also conducted on a relatively small sample size,took into account participants'reporting of LBP pain over the last year prior to the study and did not analyse possible side-to-side differences.
Most papers examining LBP and LAMs have been casecontrol,with groups of participants being divided into a control(without LBP during and/or prior to the study)and an LBP(LBP during or prior to the study)group.Thus,most of the previous studies which inquired the role of LAM morphology as predisposing factors for LBP in athletes suffer from their cross-sectional methodology.This cohort study aimed to detect the role of these muscles as risk factors for LBP.If such associations exist,appropriate preventive and rehabilitative programs for improving the function of LAM could be helpful in the prevention of LBP's occurrence and recurrence in adolescent athletes.We hypothesized that USI morphological measurements of the LAMs in adolescent soccer players may predict future LBP incidence.Therefore,this is the first study on adolescent soccer players,where LAM morphology was measured in a pain-free population and then observed for LBP occurrence.Thus,our study's aims were to:a) find possible LBP predictors from USI measurement of LAM morphology(rest thickness and side-to-side differences);b)assess a correlation between significant LBP predictors and the week of LBP experience.
2.Materials and methods
2.1.Setting and study design
This was a longitudinal study conducted in a sports and recreation center in the Silesian region of Poland.USI data were collected(baseline)on a single cohort(10-17 years)of soccer players,and the occurrence of LBP was observed for 6 months with the use of a weekly questionnaire conducted by a physiotherapist.The study was designed according to the Declaration of Helsinki and was approved by the Bioethics Committee for Scientific Studies at the Academy of Physical Education in Katowice.All participants and their parents or legal guardians received oral and written information about all procedures and gave their signed informed consent to participate.
2.2.Study population
A study population of boys between the ages of 10 and 17 years was selected from a semi-professional soccer club.At the beginning of the study,the participants answered questions related to their medical history.In the case of younger children(under 12 years of age),at least one of their parents was present during the examination.Information from a coach and physiotherapist working at the club regarding the children's health was also analysed.At this stage,individuals who had a surgical procedure on the thoracic cage,abdominal cavity,pelvic girdle and/or spine were excluded.All participants who claimed that they had experienced LBP 4 months prior to or during the USI examination were also excluded from further analysis.The 4-month period was arbitrarily established as a reasonable time in which participants were able to consider their lower back condition.Additionally,in accordance with the proposed definition,13only individuals who had played soccer for at least 2 years(prior the study)and at least twice a week were included in the study.
2.3.Measures
A real-time USI scanner(Honda HS 2100;Honda Electronics Co.Ltd.,Medical Division,Toyohashi,Japan)with a linear array transducer(HLS-575 M;Honda Electronics Co.Ltd.)was used to obtain images of the LAMs.The frequency of the transducer was set at 7.5 MHz.The transducer was placed on the anterolateral wall of the abdomen between the iliac crest and the costal margin,perpendicular to the longitudinal axis of the body,and was finally adjusted to ensure that,at rest,the fascial borders of the LAMs appeared parallel on the screen.
Images of the thickness of the obliquus external(OE),obliquus internal(OI),and transversus abdominis(TrA)muscles were made in the supine rest position.14The thickness of the muscles was stored at the end of normal expiration.To avoid the confounding effect offood consumption on the LAMs,all of the USI measurements were performed with the necessary interval between the last meal of the participants and the time of measurement.15
All images were saved on an external drive in JPG format and transferred to a computer,where they were further processed using Photoshop software(Photoshop x64;Adobe Systems,Inc.,San Jose,CA,USA),which has been used previously for the evaluation of the thickness of the LAMs in adolescents.13,16A detailed protocol for editing the images is presented in Linek et al.'s17study.All USI procedures were performed by 1 investigator(PL,a physiotherapist with 6 years of experience of assessing LAM in adolescent and adult populations)for all participants and the measurements were taken at the baseline of the study.13,14,18-20
The means of 3 measurements(from 3 separate scans at each site)of the OE,OI,and TrA obtained from the USI were used for the analysis of the measurements performed separately for the right and left sides of the body.The allometric parameters necessary for the scaling procedure of the actual muscle thickness were from Linek's study.21The allometric parameters were 0.77 for the OE,0.67 for the OI,and 0.61 for the TrA.
The process took place in the following order:1)to normalize the muscle size measurement to body mass,the following equation was used:21
2)to determine the relative side-to-side differences(from actual values),the following formula was used:
Relative muscle thickness difference

All equations were applied independently for the OE,OI,and TrA muscles.
At baseline,all participants answered a question regarding having LBP over the last 4 months.Participants who answered“no”to this question were recruited into the study.LBP was defined as a pain between the last rib and lower gluteal fold,which is bad enough to limit or change athletes'daily routine or sports activities for more than 1 day.22
The included participants were then observed for 6 months by answering 4 key questions(the Oslo Sports Trauma Research Center questionnaire;OSTRC)asked at the beginning of each week.23The printed version of the OSTRC was given to the participants by the physiotherapist.If an athlete achieved the minimum score for each of these questions(full participation without problems/no training reduction/no performance reduction/no symptoms),the questionnaire was finished for that week.However,if the athlete reported anything other than the minimum value for any question,the questionnaire continued by asking them to define the problem.23Participants whose symptoms fitted the above-mentioned LBP definition were considered LBP participants.Additionally,the usual LBP Visual Analogue Scale(VAS)was asked.Other participants who did not report LBP during the 6 months of the study were considered as no-LBP.
2.4.Statistical analysis
The basic parameters(age,weight,height,body mass index(BMI),and sports practice)between LBP and no-LBP participants were assessed with the use of attest for independent samples.To assess the relationship between LAM and LBP's incidence,the binary(1-LBP present;0-LBP absent)logistic regression was used.For the established logistic models,to assess fitting,the Hosmer-Lemeshow test was used.For significant variables,the odds ratio(OR)was also presented.To assess the correlation between the significant variables and the week of LBP experience in the LBP group,Spearman's rank test was used.All statistical analyses were performed with the use of Statistica 12 PL software(StatSoft Inc.,Tulsa,OK,USA),and for all tests,p<0.05 was considered significant.
3.Results
3.1.Participants
The inclusion criteria were met by 97 of the 120 initially invited participants.In the 6-month observation,from the 97 participants,9 players reported LBP and their VAS was found to be 6.A comparison of 9 LBP athletes with the remaining participants(n=88)did not demonstrate any statistically significant difference in terms of height,body weight,BMI,age or years of practicing soccer(Table 1).
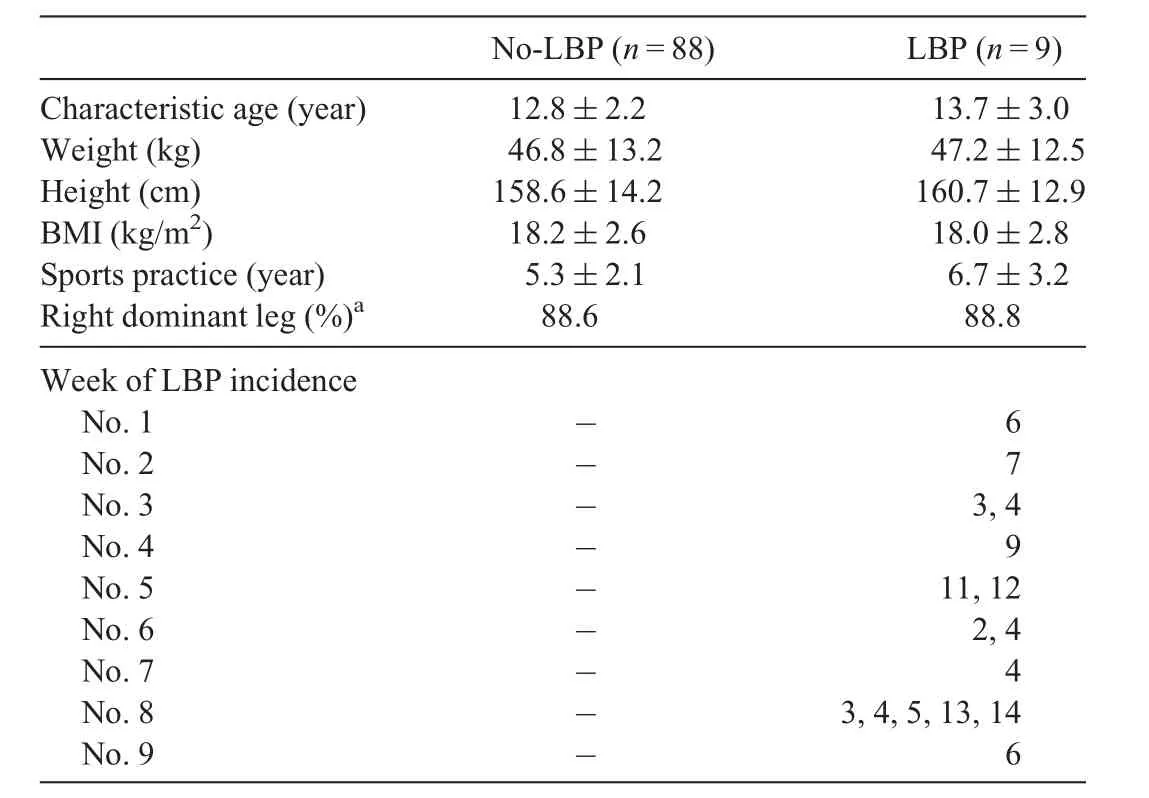
Table 1Basic data of participants(mean±SD).
3.2.LAMs
The binary logistic regression showed that increases in the OI side-to-side difference is strongly linked to a higher probability of LBP occurrence(OR=19.99;95%CI:2.4-167.9).For the established logistic model the Hosmer-Lemeshow test was insignificant(x2=7.83,p=0.35),which indicates that the model was a good fit.For the remaining variables(LAM actual values,LAM allometric-scaled values,asymmetry for TrA and OE),there were no statistical relationships in the x2Wald test(Table 2).
The mean±SD values for OI side-to-side difference were 0.59±0.41 and 1.50±1.02 for no-LBP and LBP subjects,respectively.In the LBP subjects,there were 2 participants(22%)with an OI side-to-side difference lower than 0.60mm,but in the no-LBP subjects there were no participants with an OI side-to-side difference higher than 1.27mm(the highest value was 1.25mm).The additionally performed Spearman's correlation found a linear relationship between the OI side-toside difference value and the number of weeks with LBP(R=0.75,p=0.02).The mean actual value of OI muscle thickness on both sides(dominant and non-dominant)of the body in no-LBP and LBP participants also indicated that hypertrophy on non-dominant side of the body in LBP subjects is responsible for higher side-to-side asymmetry(Fig.1).
4.Discussion
This was the first longitudinal study where initially assessed LAM morphology and LBP's incidence in adolescent soccer players were observed.The results show that asymmetrical OI morphology in pain-free subjects assessed in the supine rest position can be later connected with LBP incidence.The presence of an OI side-to-side difference can increase the odds for LBP by at least 2.4 times.Also,detailed analysis showed that a side-to-side difference in the USI thickness measurement of OI that is more than 1.25 mm can be a predictive factor offuture LBP occurrence among adolescent soccer players.
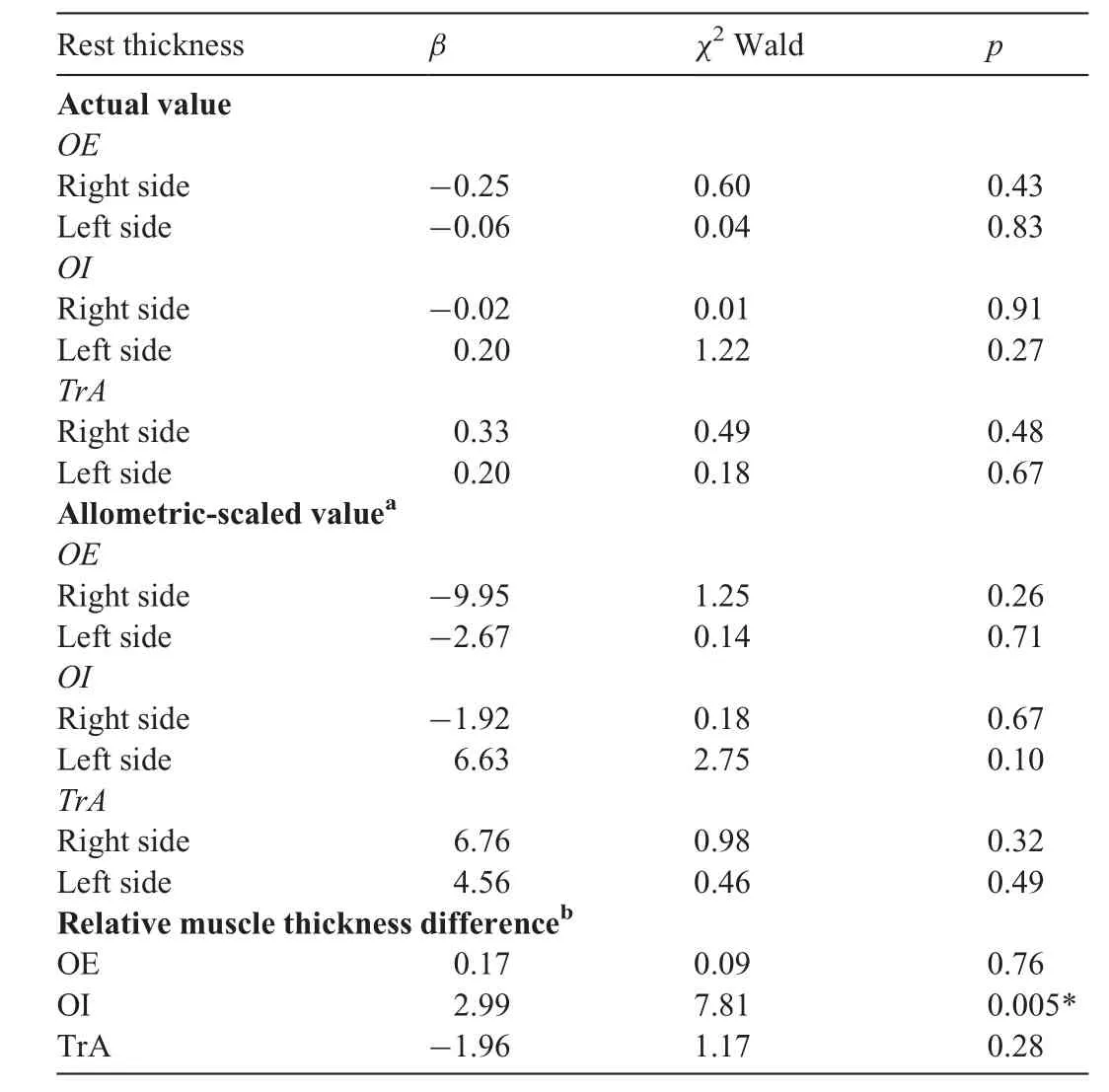
Table 2The results of binary logistic regression analysis for all variables.
The above-mentioned result is in contrast to recently published research by Gray et al.,24where greater OI muscle asymmetry in adolescent cricket fast bowlers was connected with being a protective rather than a provocative factor for LBP.Unlike cricket,soccer seems to be a more symmetrical sport where the use of both legs is usually encouraged during modern sports training even at amateur level.Hence,LAMs,such as the OI,which generate rotation and side flexion,are similarly loaded on both sides of the body during soccer practice.In line with our results,an MRI study on healthy adult soccer players showed that LAMs had similar volumes on both sides of the body.10Previously,a study of young soccer players also showed that the OI and OE were similar on both sides of the body.12Some other studies indicated that healthy adolescent volleyball players and physically active adolescent girls had on average a side-to-side OI thickness asymmetry of 1mm and 0.61 mm,respectively.13,16
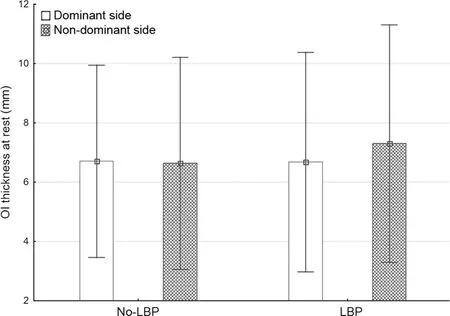
Fig.1.The rest thickness of the oblique internal abdominis muscle in LBP and no-LBP subjects.LBP=low back pain;OI=obliquus internal.
In our study,an analysis of LAMs revealed non-significant differences in size between the 2 groups for the right and left sides of the body.Similar results were presented in recently published papers on adolescent and adult LBP soccer players.11,12Unfortunately,in these articles,side-to-side asymmetry was not taken into account.In our study,asymmetrical OI morphology in pain-free adolescent footballers may be connected with LBP incidence.The OI mean thickness value on the dominant side was almost identical in LBP and no-LBP athletes(mean difference 0.02 mm),whereas on the non-dominant side of the body the mean value of OI thickness was higher by 0.67mm in the LBP participants(Fig.1).This implies that OI side-to-side differences occurring in LBP participants may be due to hypertrophy of the OI muscle on the non-dominant side of the body rather than atrophy of the OI on the dominant side.Thus,overuse of the OI muscle on the non-dominant side of the body may contribute to OI imbalance during the stabilization of the trunk(i.e.,non-dominant leg is used as supporting base when kicking with dominant leg),which may increase the risk of LBP among adolescent soccer players.
In other studies on healthy adolescent athletes and nonathletes,some level of OI side-to-side asymmetry was usually present.In a healthy adult population,the LAMs were also quite symmetrical or sometimes had minor asymmetry.25,26Thus,it can be suggested that in healthy athlete and non-athlete populations,side-to-side OI muscle differences exist.This indicates that in predicting LBP the magnitude of the asymmetry is more important than the mere presence of asymmetry.From our study results,we can hypothesize that in adolescent soccer players an asymmetry of the OI muscle higher than 1.25mm may be a predictor of possible LBP.This suggestion is supported by a study in which the rehabilitation protocol that enhanced symmetry in the LAMs was associated with pain reduction among athletes with LBP.27Thus,adolescent soccer players with OI asymmetry should also consider a rehabilitation protocol,which will enhance OI symmetry.
With regard to allometric-scaled values,this was the first study where LAMs were analysed with the confounding effect of body mass having been removed.Hence,at this stage of knowledge it is impossible to compare the results found with different studies.Other future studies on LBP with the use of allometric-scaled values will enable a comparison to be made between the study results from different populations without the in fluence of body mass.
Some possible limitations have to be taken into account when interpreting the results presented.The first limitation is a probable overestimation of the OR result because the result was prone to sparse-data bias due to the small simple size.28-30Small number of participants with LBP may also increase the possibility of non-significant results.The threshold difference of 1.25 mm for OI side-to-side asymmetry can only be applied to the adolescent population.Therefore,this threshold needs to be used with caution,and only applied as a basis for further research.The next limitation was the lack of a detailed and radiological assessment of the lumbar spine in LBP participants;it is suggested that in order to rule out other possible LBP etiologies,such as spondylolysis,such an assessment is considered for future studies.All participants claimed that they were free of LBP 4 months prior to the study but this aspect could have been controlled in a more objective way.Finally,the study was undertaken in male soccer players,therefore the generalizability of the findings to adolescent female soccer populations may be questioned.For this reason,the study results and conclusions should be interpreted cautiously.Future study is warranted to assess these findings in a much broader population.
5.Conclusion
The morphological changes of the OI can play a role in LBP's incidence in adolescent soccer players.The presence of an OI side-to-side difference in the supine rest position increases the odds of LBP by at least 2.4 times.Hypertrophy(or overuse)rather than atrophy of the OI on non-dominant sideof the body may contribute to a trunk muscle imbalance in LBP footballers.An OI side-to-side difference greater than 1.25 mm suggests a possible increase in LBP incidence during a 6-month observation of adolescent soccer players.This threshold should be used only as a basis for further research on different athletes with LBP.
Authors’contributions
PL conceived the study,participated in its design,and drafted the manuscript;PN conceived the study,participated in its design,and helped to draft the manuscript;MAM was involved in the statistical analysis and helped to draft the manuscript;DS and TW collected data and helped to draft the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
杂志排行

Journal of Sport and Health Science的其它文章
- Reasons why older adults play sport:A systematic review
- Isokinetic trunk flexion-extension protocol to assess trunk muscle strength and endurance:Reliability,learning effect,and sex differences
- Walking pace and the risk of stroke:A meta-analysis of prospective cohort studies
- Application of network meta-analysis in the field of physical activity and health promotion
- Sedentary Behavior Research Network members support new Canadian 24-Hour Movement Guideline recommendations
- Are we really “screening”movement?The role of assessing movement quality in exercise settings